
[box type=”bio”] Learning Points for this Article: [/box]
Although classically described as a hyperostosis of cortical bone, intra-articular soft tissue masses are an important cause of recurrent morbidity in melorheostosis. Excision of these masses leads to a symptomatic improvement in joint function and can help delay an eventual arthroplasty.
Case Report | Volume 7 | Issue 5 | JOCR Sep – Oct 2017 | Page 29-33| Anirudh Sharma, Bobby John, Ritesh A Pandey. DOI: 10.13107/jocr.2250-0685.884
Authors: Anirudh Sharma [1], Bobby John [1], Ritesh A Pandey [1]
[1] Department of Orthopaedics, Christian Medical College and Hospital, Ludhiana, Punjab, India.
Address of Correspondence:
Dr. Anirudh Sharma,
Department of Orthopaedics, No. 2023, Junior Doctors Hostel, Christian Medical College and Hospital, Brown Road, Ludhiana, Punjab – 141 008, India.
E-mail: anirudh_utd@yahoo.co.in
Abstract
Introduction: Melorheostosis is a rare benign sclerosing dysplasia affecting bone, which causes significant morbidity in the form of pain and restriction of joint movement. Treatment options are varied, and recurrence is common after surgical treatment (known to occur after surgical procedures). Choosing the most appropriate treatment option in the management of a recurrent case is challenging, with very little supporting evidence in literature owing to the rarity of the disease. We hereby present a case of recurrent melorheostosis involving the knee; discuss treatment options and the rationale of our treatment.
Case Report: We present the case of a 42-year-old female who was operated at our institution previously 7 years ago for melorheostosis of her left knee and had undergone excision of intrarticular hyperostotic masses. However, pain and limitation of motion recurred in the operated knee 4 years later, and radiographs and computed tomography revealed a mineralized mass situated behind the patella in the patellofemoral joint. She was treated with repeat open excision of the mass and put on a regimen of physiotherapy and bisphosphonates.
Conclusion: Open excision of symptomatic hyperostotic or mineralized soft tissue masses is perhaps the favored treatment option in such cases, the other options being arthroscopic excision and total knee arthroplasty. Limited knee motion and size of the mass often make arthroscopy an unfeasible option. Total knee arthroplasty should be reserved for cases with significant flexion contractures of the knee, or where multiple excisions have failed.
Keywords: Recurrent melorheostosis, soft tissue masses, open excision.
Introduction
Melorheostosis, also known as Leri’s disease, candle disease of bone, or osteosis eburnisans monomelica is a rare condition, which affects both bone and soft tissues [1]. It is a benign disorder with an incidence of 0.9 per million, and in essence, a sclerosing dysplasia involving mainly diaphyseal and epiphyseal bone. It is known to occur in all age groups and affects both sexes equally [1]. Although the disorder is understood to be a congenital aberration, research on the disease so far has been unable to pinpoint a specific genetic correlation [2]. Clinically, the manifestation of the disease depends on the site it involves, and the age at which symptoms begin. The appendicular skeleton is much more commonly involved than the axial skeleton, although there have been reports of myelopathy resulting from melorheostosis of the spine. The disease progresses significantly faster in children than in adults, and in this age group is also known to cause disordered growth, including shortening and angular deformity of the limbs [3]. The most common symptoms include pain and stiffness typically involving a single limb, usually the lower [4]. This can result in significant morbidity in terms of walking and mobility. Restricted range of motion of involved joints can be subsequent to soft tissue masses, contractures, or intraarticular extension of the hyperostosis [4]. The classical radiological appearance of melorheostosis is that of flowing hyperostosis along the length of the involved bone, resembling dripping candle wax. Whereas a computed tomography (CT) scan is helpful to assess the mineralization and relation of the hyperostotic masses to the parent bone, magnetic resonance imaging (MRI) may help to appreciate nonmineralized paraarticular soft tissue masses [5]. Management of pain and restricted motion in a joint involved by melorheostosis is challenging, which is further compounded by lack of enough supporting evidence in literature. Various treatment options described in literature include splinting and physiotherapy, soft tissue release, tendon lengthening, capsulotomy, excision of the hyperostotic and soft tissue masses, arthroscopic release, and arthroplasty [6]. Recurrence is known to occur in a number of cases despite surgical treatment. We hereby describe a case of recurrent melorheostosis involving the knee joint, with challenges involved in its management.
Case Report
The patient presented to us for the first time in 2009 at the age of 36 years, with complaints of severe pain and restriction of motion of her left knee, which had initially started 11 years before this presentation (in 1998) but had gradually progressed to significantly limit her day-to-day mobility. She was asymptomatic till the age of 24 years when she started to develop pain in her right knee, which started insidiously and was mild to start with. There were periods of exacerbation with intervening periods of relief, and she was treated with occasional analgesics during the episodes of pain. She gives a history of mild swelling of her knee during the exacerbations, which eventually used to subside. She, however, noticed a gradual restriction of flexion of her left knee over the next few years. Such treatment with occasional analgesics continued till a further period of 11 years when she presented to us at the age of 36 years with severe pain and limitation of knee movement.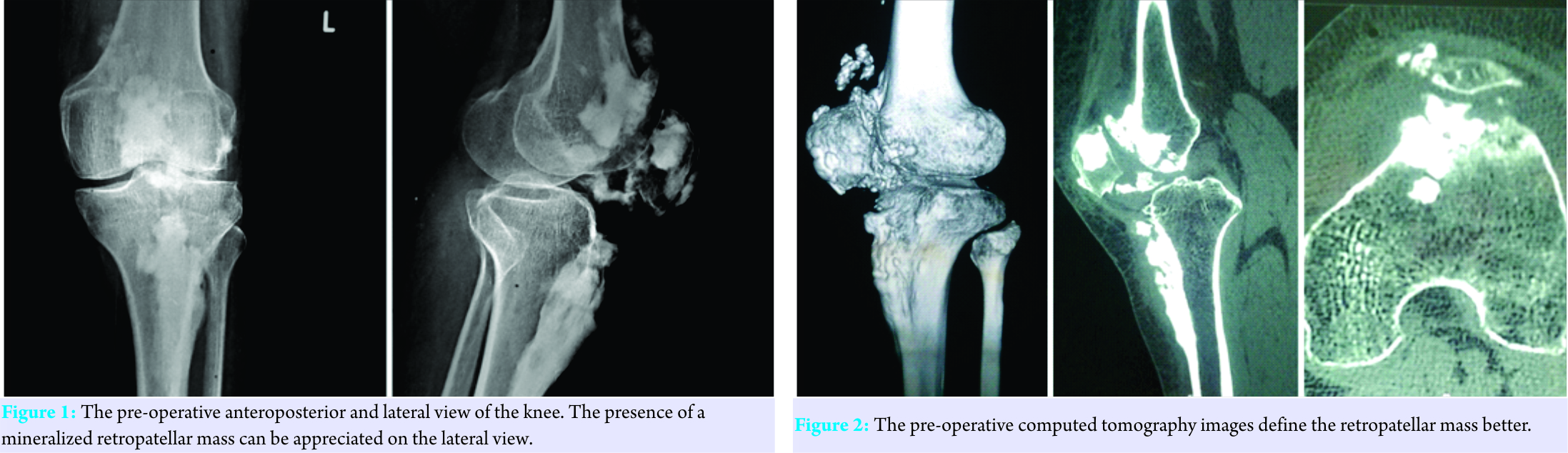
On examination, she had a tender joint line with a 5° flexion deformity of her knee. The range of motion was from 5° to 40°. She underwent radiographic (X-ray) examination, which confirmed the diagnosis of melorheostosis by its typical radiological appearance. Hematological and biochemistry investigations revealed no significant abnormality. It was decided to excise the hyperostotic infrapatellar masses extending into the joint, and this was performed through a combined anterolateral and medial approach to the knee. Postoperatively, she had significant symptomatic pain relief and her active knee motion improved to 80°. Thereafter, she was asymptomatic till 4 years after surgery when the pain recurred. However, this was mild and the patient was able to walk fairly well until recently (in 2016), when she presented at the age of 42 years with worsening of pain, which was affecting walking.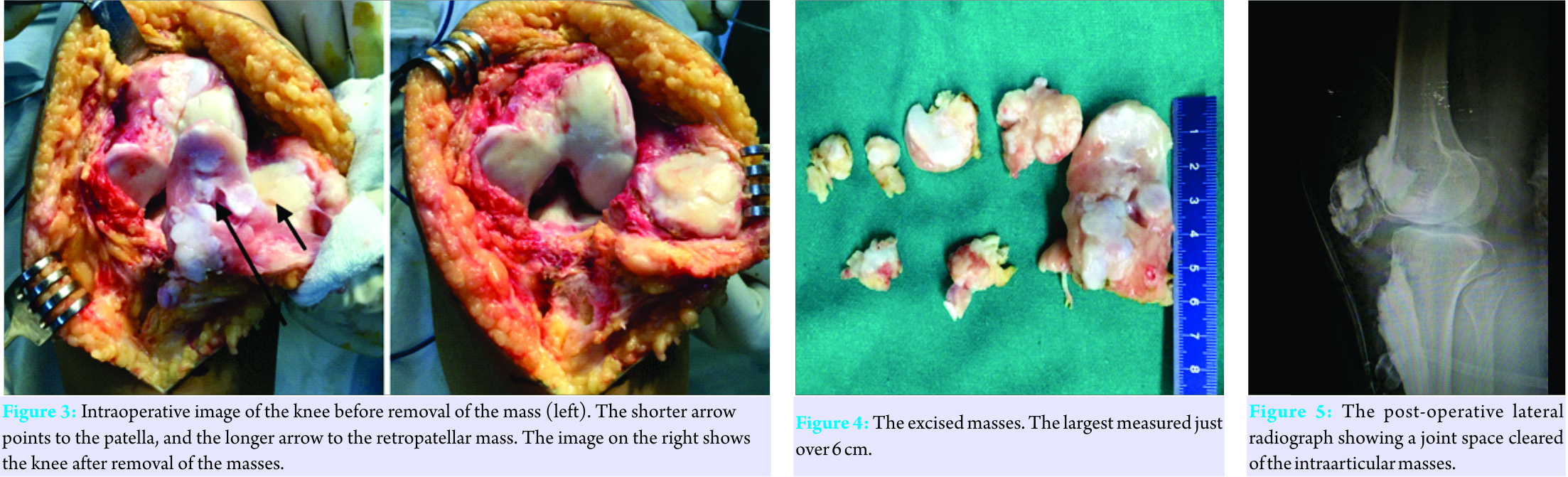
Examination revealed a 5° flexion deformity and range of motion limited to 35°. She underwent radiographs (Fig. 1) and a CT scan (Fig. 2), which revealed a mineralized mass located just posterior to the patella, to be the main cause of the pain and loss of movement. It was decided to again perform an excision of this mass, which was done this time by a medial parapatellar approach. Intraoperatively (Fig. 3), the mass was found to be 6.1 cm × 3.5 cm and excised along with other smaller mineralized masses found in the joint space (Fig. 4). A full range of motion could be achieved at surgery after excision of this mass (Fig. 5). These were sent for histopathological examination, which revealed thickened haphazard lamellae of bone lined by osteoblasts and few osteoclasts. There was no atypia or increase in mitotic activity. Postoperatively, the patient was started on a regimen of physiotherapy and was given bisphosphonates. At 1-year follow-up, she was walking unaided with no pain and knee flexion of 90°.
Discussion
Melorheostosis was first described in 1922 by Leri and Joanny, after whom the disease is frequently referred to as Leri’s disease. The etiology of melorheostosis so far remains unclear, and the hypothesis proposed by Murray and McCredie [7], is considered the most probable pathophysiology underlying its occurrence. They suggested that the development of melorheostosis is linked to sclerotomes, which are areas of bone supplied by a single spinal sensory nerve. This hypothesis is somewhat successful in explaining the peculiar monomelic limb involvement in melorheostosis. A definitive genetic link to the disease has so far not been identified, but a number of reports have linked melorheostosis with osteopoikilosis, which has led to the suspicion that the LEMD3 or MAN1 gene may be associated with the development of both these conditions [2]. Most interesting is the observation that corticotomy performed in a bone affected by melorheostosis, resulted in a regenerate that resembled the melorheostotic bone. This led to the hypothesis that the disease results from an abnormality of intramembranous ossification.
The radiological appearance classically described as a flowing cortical hyperostosis along the shaft of a long bone resembling wax flowing down a candle remains the mainstay of diagnosis. Soft tissue masses in melorheostosis have been described in literature [5, 8], and it is known that these may not necessarily be mineralized. CT reveals that in many instances these are not attached to the underlying bone [9]. The importance of imaging lies not only in establishing the diagnosis but also in identifying those paraarticular and intraarticular soft tissue masses that may be primarily responsible for the patient’s symptoms. This is well illustrated in our case description. In our case, we found 3D CT images very helpful to identify the paraarticular and intraarticular masses, correlate their location with the patient’s symptoms, and thus help plan the surgery. We recognized that the patient’s symptoms were primarily due to a retropatellar, intraarticular mass. Although we did not perform an MRI of the affected knee, literature suggests that this may show enhancement of the tissue surrounding the soft tissue masses, indicating inflammatory edema, and the cause of the patient’s symptoms [9]. However, MRI appearance of the soft tissue masses is extremely variable and may not be the best imaging modality to study these. Joint contractures are a well-known association of melorheostosis and occur due to the process of abnormal ossification extending into the soft tissues. In the series of Campbell et al. [10], the most common location for the soft tissue contracture was found to be the plantar fascia. These contractures, especially in children, are extremely difficult to treat and may be permanent. In our case, we did not find any significant contracture, other than the patient having a 5° flexion deformity of the knee. In our extensive search of literature regarding recurrent intraarticular melorheostosis affecting the knee, we found that Moulder and Marsh described a patient, who was successfully treated by them with a total knee arthroplasty [11]. The patient was 40-year-old, with a 30° flexion contracture of the knee. There had been two previous arthroscopic attempts at removing a calcified fat pad and intraarticular loose bodies. Rooney et al. described a case of melorheostosis of the knee where a 2 cm loose body was removed by arthroscopic means [12]. Claramunt et al. described a case where an arthroscopic assisted release of a knee contracture was performed, requiring five portals and a mini-open approach to excise the bone fragments [6]. Similar to our case, Hasegawa et al. [13] described a case in which excision of an ossified melorheostotic soft tissue mass from the lateral side of the knee was performed, which required a reexcision 6 months later. Recurrence requiring reoperation is extremely common in patients treated surgically, and relief provided by surgery is temporary. In a retrospective analysis of 24 patients at the Mayo clinic [14], 54% of patients who underwent surgery required a repeat procedure. The mean number of surgeries required per patient was found to be 2.09. One-third of all total knee arthroplasties performed for melorheostosis required revision. In treating this recurrent case of intraarticular melorheostosis, we considered the options of open and arthroscopic excision. We chose an open excision instead of an arthroscopic procedure since performing arthroscopy in a knee with flexion limited to 35° would have been difficult. The CT scan also revealed a large mass 6 cm × 3.5 cm in size, which was mineralized and would have been an arthroscopic challenge. Bisphosphonates have been found useful in relieving the pain in melorheostosis [15]. We started the patient on bisphosphonates postoperatively in a hope to reduce the pain, and possibly reduce the chances of a recurrence. The patient was started on knee range of motion exercises from the second post-operative day and a range of motion up to 70° was achieved before discharge. At 1-year follow-up, the patient was walking pain-free, with a range of motion till 90° flexion. We believe that our procedure, although associated with a significant risk of recurrence can provide the patient with a number of symptom-free years. We also recognize that the patient will likely require a total knee replacement in the future. However, delaying the primary procedure would preclude the need for a revision.
Conclusion
Recurrent intraarticular melorheostosis is a rare entity with little reporting in literature and poses a challenge in management. Treatment options vary and it is important to choose the most effective option. Arthroscopic excision and debridement may be the preferred option where range of motion at the knee is fairly good, with small sized intraarticular masses. Total knee arthroplasty should be the preferred modality of treatment when the disease is associated with a significant flexion contracture, or where multiple open excisions have failed. However, correlating clinical examination with imaging findings is important to identify the periarticular and intraarticular masses responsible for symptoms, and selective excision of these can be a successful (albeit temporary) method of relieving pain and stiffness.
Clinical Message
Although melorheostosis is commonly understood as a hyperostosis of cortical bone, soft tissue masses, especially those that are intraarticular, are an important cause of morbidity in this disease. Excision of these masses can provide a reasonable symptom-free interval and is helpful in delaying an eventual arthroplasty.
References
1. Long HT, Li KH, Zhu Y. Case report: Severe melorheostosis involving the ipsilateral extremities. Clin Orthop Relat Res 2009;467:2738-43.
2. Mumm S, Wenkert D, Zhang X, McAlister WH, Mier RJ, Whyte MP. Deactivating germ line mutations in LEMD3 cause osteopoikilosis and buschke-ollendorff syndrome, but not sporadic melorheostosis. J Bone Miner Res 2007;22:243-50.
3. Younge D, Drummond D, Herring J, Cruess RL. Melorheostosis in children. Clinical features and natural history. J Bone Joint Surg Br 1979;61:415-8.
4. Greenspan A, Azouz EM. Bone dysplasia series. Melorheostosis: Review and update. Can Assoc Radiol J 1999;50:324-30.
5. Yu JS, Resnick D, Vaughan LM, Haghighi P, Hughes T. Melorheostosis with an ossified soft tissue mass: MR features. Skeletal Radiol 1995;24:367-70.
6. Claramunt RT, López XP, Palou EC, García JC, Verdie LP. Arthroscopically assisted knee contracture release secondary to melorheostosis: A case report. Knee Surg Sports Traumatol Arthrosc 2011;19:264-6.
7. Murray RO, McCredie J. Melorheostosis and the sclerotomes: A radiological correlation. Skeletal Radiol 1979;4:57-71.
8. Goldman AB, Schneider R, Huvos AS, Lane J. Case report 778. Melorheostosis presenting as two soft-tissue masses with osseous changes limited to the axial skeleton. Skeletal Radiol 1993;22:206-10.
9. Suresh S, Muthukumar T, Saifuddin A. Classical and unusual imaging appearances of melorheostosis. Clin Radiol 2010;65:593-600.
10. Campbell CJ, Papademetriou T, Bonfiglio M. Melorheostosis. A report of the clinical, roentgen graphic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-304.
11. Moulder E, Marsh C. Soft tissue knee contracture of the knee due to melorheostosis, treated by total knee arthroplasty. Knee 2006;13:395-6.
12. Rooney RC, Fernicola PJ, Pitcher JD. Arthroscopic excision of intra-articular ossifications. A case report and review of the literature. Am J Orthop (Belle Mead NJ) 1996;25:437-40.
13. Hasegawa S, Kanda S, Imada H, Yamaguchi T, Akiyama T. Melorheostosis with recurrent soft-tissue components: A histologically confirmed case. Skeletal Radiol 2017;46:399-404.
14. Smith GC, Pingree MJ, Freeman LA, Matsumoto JM, Howe BM, Kannas SN, et al. Melorheostosis: A retrospective clinical analysis of 24 patients at the mayo clinic. PM R 2017;9:283-8.
15. Slimani S, Nezzar A, Makhloufi H. Successful treatment of pain in melorheostosis with zoledronate, with improvement on bone scintigraphy. BMJ Case Rep 2013;2013. pii: Bcr2013009820.
 |
 |
 |
| Dr. Bobby John | Dr. Anirudh Sharma | Dr. Ritesh A. Pandey |
| How to Cite This Article: John B, Sharma A, Pandey RA. Managing Recurrence in Intraarticular Melorheostosis Involving the Knee Joint: A Case Report. Journal of Orthopaedic Case Reports 2017 Sep-Oct;7(5):29-33 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


