
[box type=”bio”] Learning Points for this Article: [/box]
Iliacus hematoma and consequent femoral nerve palsy are a possible, even if rare, complication of hip surgery, especially in patients under anticoagulant therapy; surgical drainage is advised for wider hematoma and severe neurological symptoms.
Case Report | Volume 7 | Issue 5 | JOCR September – October 2017 | Page 3-6| L Andreani, A M Nucci, M Giuntoli, M Lisanti. DOI: 10.13107/jocr.2250-0685.872
Authors: L Andreani [1], A M Nucci [1], M Giuntoli[1], M Lisanti [1]
[1] Department of Orthopaedics and Traumatology, University of Pisa, Pisa 56126, Italy.
Address of Correspondence
Dr. Anna Maria Nucci,
Department of Orthopaedics and Traumatology, University of Pisa, Pisa 56126, Italy.
E-mail: annamarianucci90@gmail.com
Abstract
Introduction: Femoral nerve compression caused by iliopsoas hematoma is a rare complication after hip surgery. To the best of our knowledge, this is the first case after hemiarthroplasty. In this case, iliacus hematoma resulted from spontaneous bleeding favored by anticoagulant therapy.
Case Report: A 78-year-old female developed left groin pain associated with typical symptoms of femoral nerve palsy about 2 weeks after left hip hemiarthroplasty [1, 2, 3]. Computed tomography revealed the presence of a left iliopsoas hematoma that was surgically drained. Inguinal pain was immediately relieved, while nerve palsy recovered only partially, but the quality of life drastically improved and she was able to walk using a walker without pain.
Conclusion: Even if it is a rare condition, the formation of a hematoma of iliopsoas muscle should be considered in patients that present symptoms of femoral nerve palsy, especially if treated with heparin or other anticoagulant drugs. Surgical drainage of the hematoma is indicated when symptoms are severe and disabling, and in this way, surgery could improve quality of life.
Keywords: Case report, femoral nerve palsy, hip hemiarthroplasty, iliopsoas hematoma, proximal femoral fracture.
Introduction
Iliacus hematoma and consequent femoral nerve compression are a rare complication after hip surgery. In the literature, there are only a few cases of patients who presented this complication after total hip replacement or after revision hip arthroplasty. We report the case of a patient that was diagnosed with iliopsoas hematoma 2 weeks after left hemiarthroplasty. In this case, the formation of the hematoma was probably favored by the administration of anticoagulants rather than the surgical act. Surgical drainage of the iliacus hematoma was performed, and even though, neurologic symptoms recovered only partially, it was essential to solve the severe inguinal pain and improve patient quality of life.
Case Report
A 78-year-old Caucasian female was admitted to our Emergency Department after an accidental domestic fall on her left hip. The patient cannot bear any weight on her left leg that was painful, shorter, and in external rotation. Her general status appeared good, and she had no neurological symptoms. She had no significant past medical history apart from high blood pressure in treatment with angiotensin-converting-enzyme-inhibitor. Conventional radiograms of her left hip showed a transcervical fracture of the femur (AO classification 31-B2) (Fig. 1). Laboratory blood tests did not reveal any kind of alteration. The day after, the patient underwent left cemented hip hemiarthroplasty using a posterolateral approach and a spinal anesthesia (Fig. 2).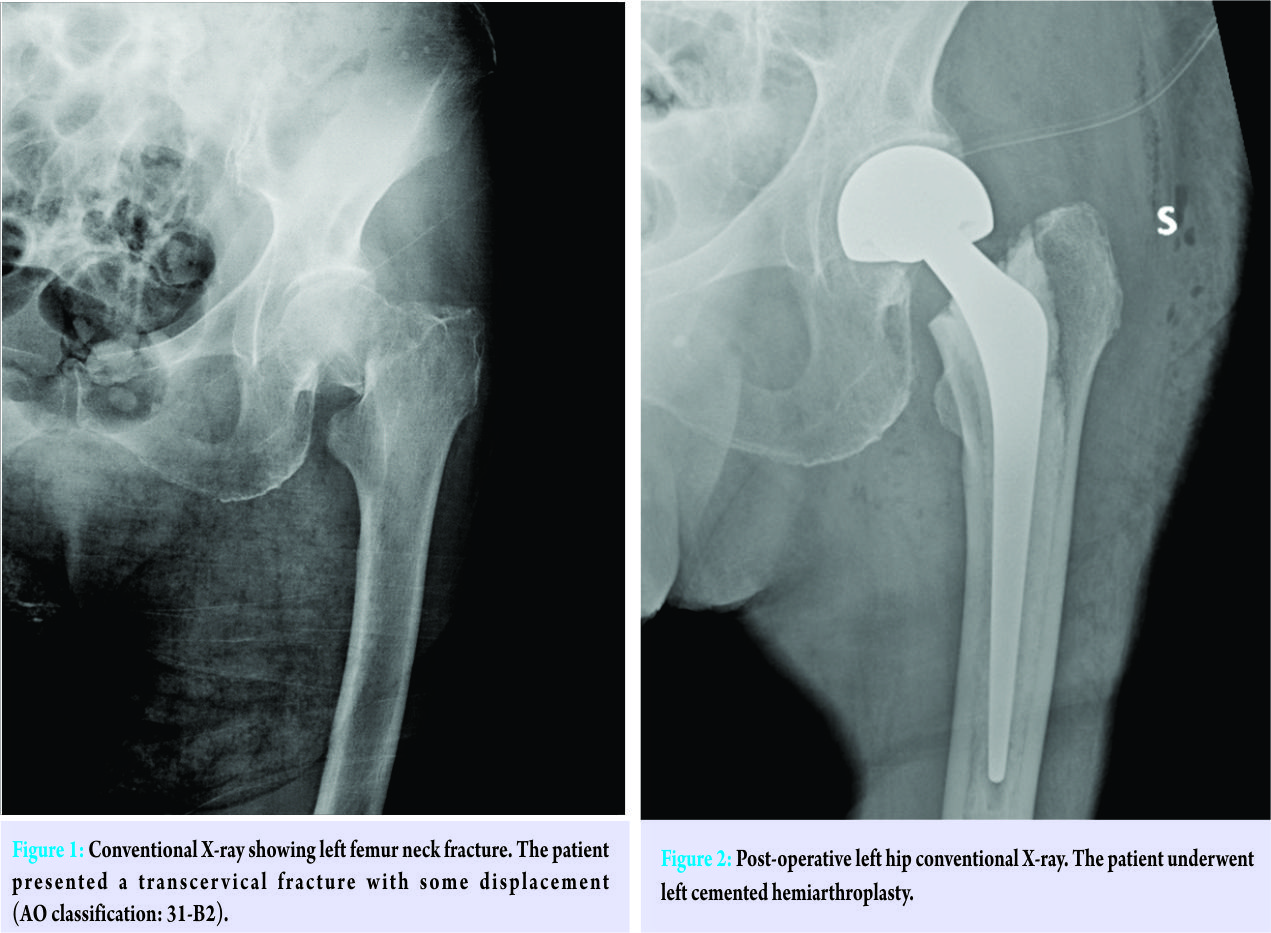 According to our thromboembolism prophylaxis protocol, the patient received 4000 UI of enoxaparin (Clexane) subcutaneously once daily since the day of the trauma for a month. The post-operative course was regular apart from moderate anemia treated with blood transfusions. In the following days, hemoglobin level returned in the normal range, and the patient started a rehabilitation program. When the patient was discharged on the 5th post-operative day, she had no motor or sensitive peripheral deficit and was able to walk with a walker. 15 days after surgery, the patient was admitted again to our Emergency Department because of worsening left groin pain and left leg muscular weakness. She denied any other trauma or fever episode. She could not bear any weight on her left leg. She had reduced sensibility in her left thigh and was unable to extend actively her left knee. From a clinical point of view, left patellar reflex was absent, left quadriceps force was 0/5 (Medical Research Council scale), while left tibialis anterior and left extensor longus hallucis were normal (5/5). Surgical wound was completely closed and showed no signs of infection. At that time, conventional X-rays of the hip and the pelvis showed no abnormalities. The hip prosthesis appeared well integrated and had no signs of mobilization or mechanic dysfunction. An enhanced computed tomography (CT) scan of the abdomen and pelvis demonstrated the presence of three voluminous left hematomas with a diameter ranging from 5 up to 11 cm involving psoas and iliac muscles dislocating the femoral neurovascular bundle under the inguinal canal and in absence of active bleeding (Fig. 3).
According to our thromboembolism prophylaxis protocol, the patient received 4000 UI of enoxaparin (Clexane) subcutaneously once daily since the day of the trauma for a month. The post-operative course was regular apart from moderate anemia treated with blood transfusions. In the following days, hemoglobin level returned in the normal range, and the patient started a rehabilitation program. When the patient was discharged on the 5th post-operative day, she had no motor or sensitive peripheral deficit and was able to walk with a walker. 15 days after surgery, the patient was admitted again to our Emergency Department because of worsening left groin pain and left leg muscular weakness. She denied any other trauma or fever episode. She could not bear any weight on her left leg. She had reduced sensibility in her left thigh and was unable to extend actively her left knee. From a clinical point of view, left patellar reflex was absent, left quadriceps force was 0/5 (Medical Research Council scale), while left tibialis anterior and left extensor longus hallucis were normal (5/5). Surgical wound was completely closed and showed no signs of infection. At that time, conventional X-rays of the hip and the pelvis showed no abnormalities. The hip prosthesis appeared well integrated and had no signs of mobilization or mechanic dysfunction. An enhanced computed tomography (CT) scan of the abdomen and pelvis demonstrated the presence of three voluminous left hematomas with a diameter ranging from 5 up to 11 cm involving psoas and iliac muscles dislocating the femoral neurovascular bundle under the inguinal canal and in absence of active bleeding (Fig. 3).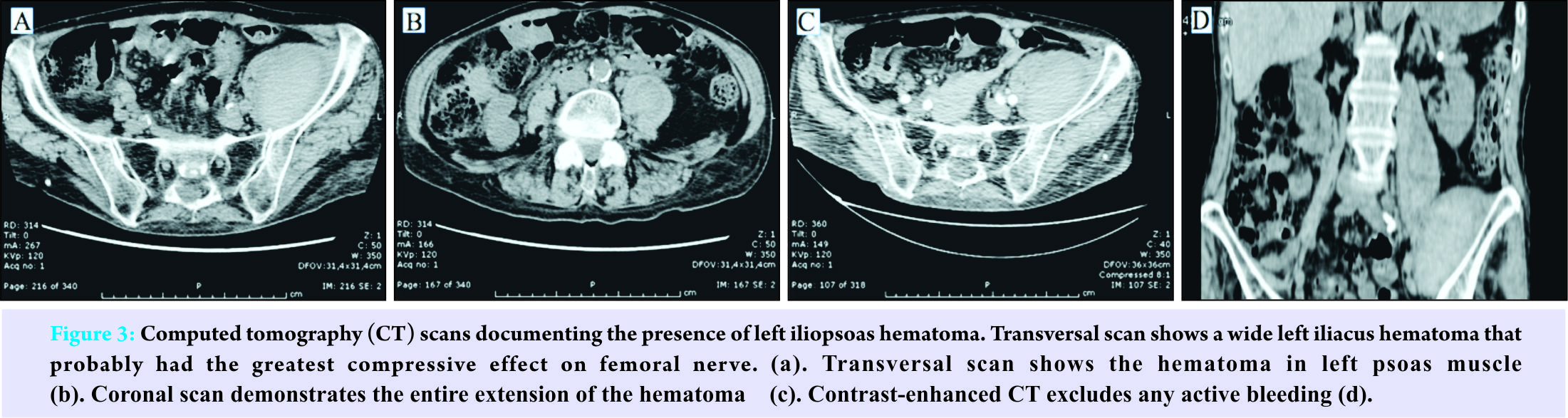 Electromyography (EMG) and nerve conduction study were performed, and they evidenced a compression of the left femoral nerve with the weakness of left vastus medialis, vastus lateralis, and iliopsoas muscles. Blood tests only revealed a mild anemia (hemoglobin was 9,7 g/dL), and no alterations of coagulation, renal function, and liver function were found. Given the severe pain and functional disability, we decided to perform surgery to drain the hematomas. We decided to use the first window of the ilioinguinal approach to reach the greatest one, and in our opinion, the most compressive one on the neurovascular bundle. The biggest hematoma was found between iliac muscle and iliac fossa and was drained, extracting about 280 cc of blood partly clotted. Post-operative CT scan of the abdomen and pelvis evidenced a drastic size reduction of the hematomas (Fig. 4). Even if neurological deficits remained, inguinal pain disappeared immediately after surgery, and 4 weeks after surgery, the patient was able to stand up and to walk using a walker for small distances. The patient underwent a protocol of physical rehabilitation, and after 6 months, she was able to walk with crutches, and a new EMG documented a partial recovery of left femoral nerve lesion.
Electromyography (EMG) and nerve conduction study were performed, and they evidenced a compression of the left femoral nerve with the weakness of left vastus medialis, vastus lateralis, and iliopsoas muscles. Blood tests only revealed a mild anemia (hemoglobin was 9,7 g/dL), and no alterations of coagulation, renal function, and liver function were found. Given the severe pain and functional disability, we decided to perform surgery to drain the hematomas. We decided to use the first window of the ilioinguinal approach to reach the greatest one, and in our opinion, the most compressive one on the neurovascular bundle. The biggest hematoma was found between iliac muscle and iliac fossa and was drained, extracting about 280 cc of blood partly clotted. Post-operative CT scan of the abdomen and pelvis evidenced a drastic size reduction of the hematomas (Fig. 4). Even if neurological deficits remained, inguinal pain disappeared immediately after surgery, and 4 weeks after surgery, the patient was able to stand up and to walk using a walker for small distances. The patient underwent a protocol of physical rehabilitation, and after 6 months, she was able to walk with crutches, and a new EMG documented a partial recovery of left femoral nerve lesion.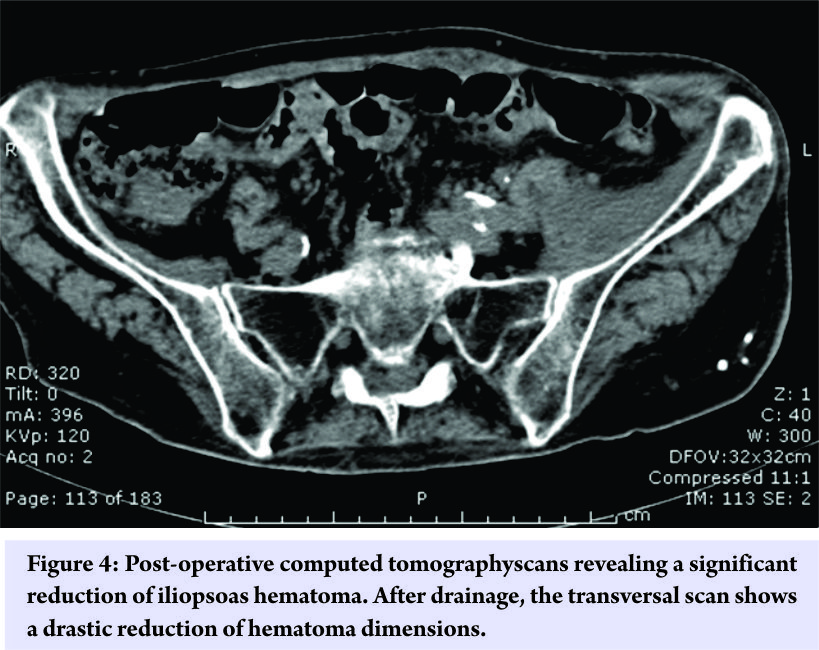
Discussion
Femoral nerve palsy is a rare condition in clinical practice. Most often compression is the causative phenomenon [4]. The formation of a compressive hematoma could derive from trauma or from spontaneous bleeding, especially in predisposing conditions such as administration of anticoagulants or bleeding diathesis. The association between iliacus hematoma and hemophilia was largely investigated by Goodfellow et al. who even described the precise mechanism of nerve compression. In their work, they explained how the rapid flow of blood could easily distend the close space between the iliacus fascia and the osseous wall of the iliacus fossa. The femoral nerve contained in this inextensible compartment is likely to be compressed in case of large hematomas [5]. In the literature, different authors have described cases of iliacus hematoma with femoral nerve compression during anticoagulant treatment [6, 7, 8, 9]. Wada et al. even reported a case of bilateral iliacus hematoma with bilateral femoral palsy in a patient receiving anticoagulant therapy [10]. It has been estimated that the incidence of retroperitoneal hemorrhage ranges from 1.3 to 6.6% in patients receiving anticoagulant treatment and from 5.5 to 10.4% in hemophiliac patients, while post-traumatic and iatrogenic hematomas seem much more uncommon [11]. Femoral nerve palsy associated with iliacus hematoma is a rare complication after hip surgery. Femoral neuropathy is described in only few cases of intrapelvic perforation of the acetabular wall during total hip arthroplasty and consequent formation of iliopsoas hematoma [1, 2], while Ha et al. reported a case after revision hip arthroplasty [3]. Even if our patient developed an iliopsoas hematoma after hemiarthroplasty, in this case, the most probable explanation is a spontaneous bleeding favored by the post-operative anticoagulant therapy rather than a muscular lesion caused by the surgical act. In fact, the implant of an endoprosthesis does not include an acetabular surgical phase, but only a femoral one, it was used a posterolateral approach, and last but not least, symptoms appeared nearly 2 weeks after surgery. Iliacus hematoma with compression of the femoral nerve may have a sudden clinical onset or may be insidious with a gradual worsening of symptoms. Typical clinical manifestations are groin pain that can migrate to the lumbar region or the thigh, flexion contracture of the hip, paralysis of the quadriceps femoris, absent or reduced patellar reflex, and absent or reduced sensibility of the anterior region of thigh [5]. In our case, the presentation was subacute with progressive worsening of pain and femoral nerve palsy until the patient became unable to stand up and walk. In this case, diagnosis was suggested by clinical examination and confirmed by means of CT scan, while EMG study was used to assess the entity of nerve lesion. In an alternative to CT, magnetic resonance imaging has proved to be a useful diagnostic instrument in previous cases, while ultrasound can be limited by body habitus, bowel gas, and operator skill [12, 13, 14]. As reported in the literature, treatment of iliacus hematoma is still controversial. There are three main options: Conservative treatment, surgery, and radiological intervention. Conservative management is preferred in case of early diagnosis and mild nervous symptoms in hemodynamically stable patients. Surgical drainage is recommended for wide hematomas or severe neurological symptoms. Due to its minor morbidity, radiological transcatheter embolization may be chosen in patients with active bleeding or hemodynamically instable [11, 12. 13, 14, 15]. In our case, we opted for surgical treatment because the patient had severe sensitive-motor deficit and persistent inguinal pain. Furthermore, when she came to visit, she had been already experiencing the symptomatology for about 15 days. After drainage of the hematoma, pain immediately disappeared, and the patient was able to restart rehabilitation protocol with a progressive recovery of femoral nerve deficit in the following months. Given the patient advanced age and late diagnosis of the lesion, neurological recovery after 6 months was only partial. However, the patient is now able to walk with a walker, and her quality of life is drastically improved.
Conclusion
Femoral neuropathy consequent to iliopsoas hematoma is a rare complication. Most frequently, it is associated with bleeding diathesis or anticoagulant therapy. We report the case of a patient who developed this type of complication about 2 weeks after hemiarthroplasty, while she was treated with anticoagulant prophylaxis. Surgical drainage proved to be a good therapeutic strategy, as pain immediately disappeared and the patient experienced a gradual, even if partial, recovery of femoral nerve function and deambulation in the following months. This case illustrates how a rare condition like femoral nerve palsy associated with iliacus hematoma may be successfully diagnosed and managed.
Clinical Message
Iliacus hematoma and consequent femoral neuropathy, even if rare, must be considered as a possible complication of hip surgery, especially in patients under anticoagulant therapy. Surgical drainage should be reserved to patients with wider hematomas or severe neurological symptoms.
References
1. Wooten SL, McLaughlin RE. Iliacus hematoma and subsequent femoral nerve palsy after penetration of the medical acetabular wall during total hip arthroplasty. Report of a case. Clin Orthop Relat Res 1984;191:221-3.1. Wooten SL, McLaughlin RE. Iliacus hematoma and subsequent femoral nerve palsy after penetration of the medical acetabular wall during total hip arthroplasty. Report of a case. Clin Orthop Relat Res 1984;191:221-3.
2. Gogus A, Ozturk C, Sirvanci M, Aydogan M, Hamzaoglu A. Femoral nerve palsy due to iliacus hematoma occurred after primary total hip arthroplasty. Arch Orthop Trauma Surg 2008;128:657-60.
3. Ha Y, Ahn I, Jeong S, Park H, Koo K. Iliacus hematoma and femoral nerve palsy after revision hip arthroplasty: A case report. Clin Orthop Relat Res 2001;283:100-3.
4. Seijo-Martínez M, Castro del Río M, Fontoira E, Fontoira M. Acute femoral neuropathy secondary to an iliacus muscle hematoma. J Neurol Sci 2003;209:119-22.
5. Goodfellow J, Fearn CB, Matthews JM. Iliacus haematoma. A common complication of haemophilia. J Bone Joint Surg Br 1967;49:748-56.
6. Retselas I, Vaiopoulos C, Chronopoulos P, Kaisidis G, Fotopoulou C, Skandalos I. Spontaneous iliopsoas muscle haematoma during anticoagulant treatment. Hell J Surg 2015;87:434-6. Available from: http://www.emj.bmj.com/ content/26/12/863.full.pdf\n ; http://www.ovidsp.ovid.com/ ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE =fulltext&D=emed9&AN=2009654854.
7. Kim SW, Kim DH, Jung SN. Spontaneous iliopsoas hematoma: A Rare Complication of Anticoagulant Use. Arch Plast Surg 2015;42:507-10.
8. Canelles E, Bruna M, Roig JV. Spontaneous hematoma of the iliopsoas muscle, The report of three vases and review of the literature. Rev Esp Cir Ortop Traumatol 2010;54:234-7. Available from: http://www.linkinghub.elsevier.com /retrieve/pii/S1988885610702388.
9. Fearn CB. Iliacus haematoma syndrome as a complication of anticoagulant therapy. Br Med J 1968;4:97-8.
10. Wada Y, Yanagihara C, Nishimura Y. Bilateral iliopsoas hematomas complicating anticoagulant therapy. Intern Med 2005;44:641-3.
11. Lefevre N, Bohu Y, Klouche S, Chemla N, Herman S. Complete paralysis of the quadriceps secondary to post-traumatic iliopsoas hematoma: A systematic review. Eur J Orthop Surg Traumatol 2015;25:39-43.
12. Choa GP, Lim CS. Iliopsoas haematoma: An uncommon differential diagnosis for groin pain. Hong Kong J Emerg Med 2011;18:173-6.
13. Marquardt G, Barduzal Angles S, Leheta F, Seifert V. Spontaneous haematoma of the iliac psoas muscle: A case report and review of the literature. Arch Orthop Trauma Surg 2002;122:109-11.
14. Parmer SS, Carpenter JP, Fairman RM, Velazquez OC, Mitchell ME. Femoral neuropathy following retroperitoneal hemorrhage: Case series and review of the literature. Ann Vasc Surg 2006;20:536-40.
15. Kong WK, Cho KT, Lee HJ, Choi JS. Femoral neuropathy due to iliacus muscle hematoma in a patient on warfarin therapy. J Korean Neurosurg Soc 2012;51:51-3.
 |
 |
 |
 |
| Dr. L Andreani | Dr. A M Nucci | Dr. M Giuntoli | Dr. M Lisanti |
| How to Cite This Article: Andreani L, Nucci, AM Giuntoli M, Lisanti M: Compressive Femoral Neuropathy Associated with Iliopsoas Hematoma Complicating Hip Hemiarthroplasty: A Case Report. Journal of Orthopaedic Case Reports 2017 Sep-Oct ; 7(5): 3-6 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


