
[box type=”bio”] Learning Points for this Article: [/box]
Obturator dislocation and ipsilateral fracture neck femur is a rare injury. In the presence of a significant sized chondral injury, it is sensible perform head replacing surgery. The Antero-lateral or lateral approach is best suited to deal with this kind of injuries.
Case Report | Volume 7 | Issue 5 | JOCR September – October 2017 | Page 16-19| Sumit Kumar Jain, Parit Aggarwal, Arun Yadav. DOI: 10.13107/jocr.2250-0685.878
Authors: Sumit Kumar Jain [1],Parit Aggarwal [1], Arun Yadav [1]
[1] Department of Orthopaedic, North DMC Medical College and Hindu Rao Hospital, Malkaganj, New Delhi, India.
Address of Correspondence
Dr. Sumit Kumar Jain,
Department of Orthopaedic, North DMC Medical College and Hindu Rao Hospital, Malkaganj, New Delhi, India.
E-mail: jainsumit24@gmail.com
Abstract
Introduction: Traumatic dislocation of hip with ipsilateral fracture neck femur is a rare injury because the different mechanism of both these injuries. The management of such injuries is a challenge as the chances of nonunion and avascular necrosis of femoral head are very high with fixation methods. We report a case of obturator dislocation of the hip with ipsilateral fracture neck of the femur which was treated with uncemented total hip replacement.
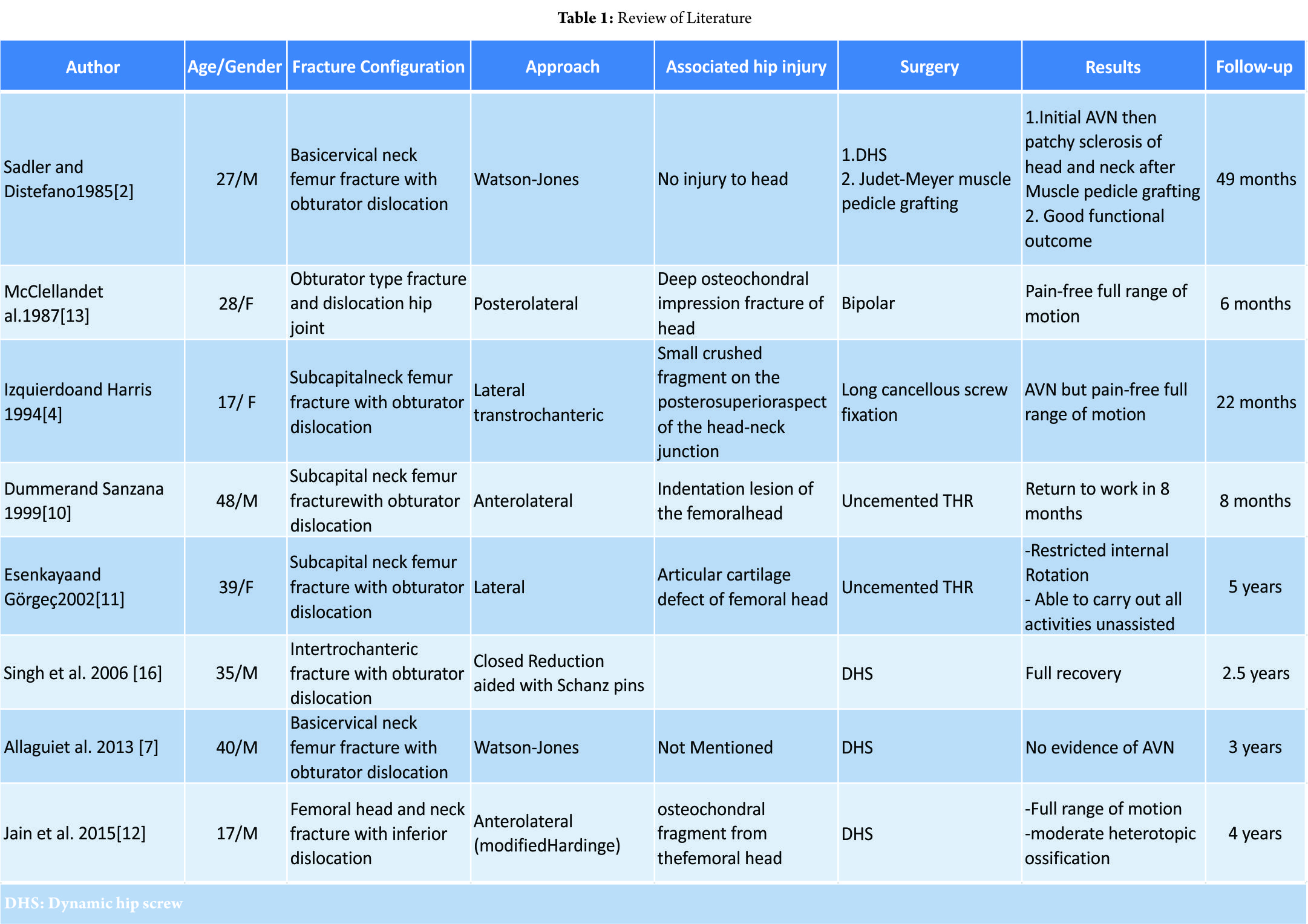
Case Report: A 32-year-old male sustained obturator dislocation with ipsilateral fracture neck femur following road traffic accident. After initial assessment and treatment, definitive treatment was carried out. Hip was approached through Watson-Jones approach. The head and neck was found to be dislocated and lying close to obturator foreman. A button hole through the anterior capsule and medium-sized chondral defect of the femoral head articular surface was noted. An uncemented total hip arthroplasty was performed. Post-operative period was uneventful and the patient was mobilized weight-bearing as tolerated with walker. He was discharged on the 5 thpost-operative day. He regained pain-free good range of motion over a period of 6 weeks.
Conclusion: Fracture pattern combining obturator dislocation and ipsilateral fracture neck femur is a rare injury. Although both head preservation and replacement methods of treatment are available, the choice of treatment depends on duration of injury, age of the patient, associated chondral injuries of femoral head, and the choice of the patient. The anterolateral or lateral approach helps to deal with the anteriorly lying head in a better way as compared to the posterolateral approach.
Keywords: Obturator dislocation, ipsilateral, neck femur fracture.
Introduction
Traumatic dislocation of the hip with ipsilateral fracture neck femur is a rare injury because the mechanisms of both these injuries are different. Anterior dislocation of the hip is caused by forcible abduction and external rotation. In abduction, the femoral neck and trochanter impinge on the acetabular rim, and as a result, the femoral head is levered out of the acetabulum and is pushed toward anterior part of the capsule resulting in anterior dislocation of the hip. Flexion of the hip during this maneuver results in obturator type of dislocation[1]. If this abduction force continues, the capsule tears anteriorly and head gets stuck inside the capsule (buttonholing), resisting further movements of the head and leading to fracture neck of femur [2]. The management of such injuries is a challenge as the chances of avascular necrosis of femoral head are very high with fixation methods [2, 3, 4]. We came across a 32-year-old male who sustained head-on collision while driving a two-wheeler resulting in obturator type of hip dislocation with ipsilateral fracture neck femur. He was treated with uncemented total hip replacement.
Case Report
A 32-year-old male patient was brought to the emergency department following a road traffic accident. He was driving two wheeler and sustained a head-on collision with four wheeler resulting in sudden halt and fall from the bike. His hip was in flexion, abduction, and external rotation with shortening of the affected leg. After initial stabilization and examination, radiographs were done which showed an obturator type anterior dislocation with fracture neck of the femur. Computed tomography scan was done to rule out for any acetabulum fracture and any other associated injury (Fig. 1). 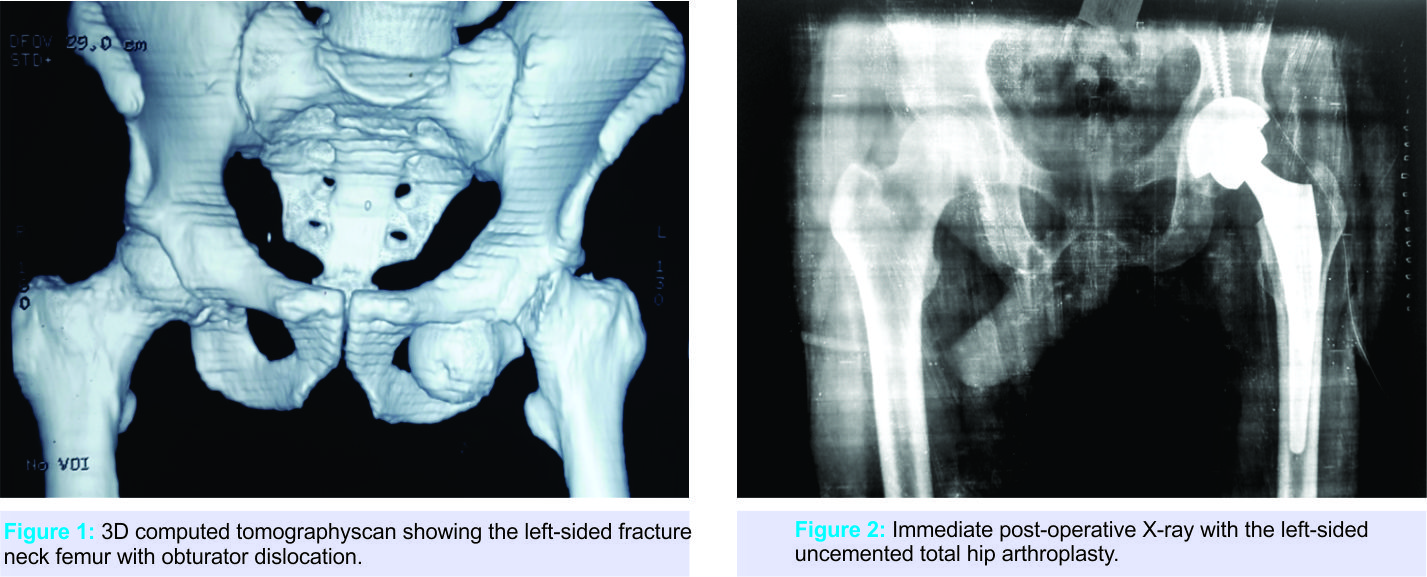 Patient and family members were consulted and detailed discussion was done regarding the type of injury and the possible treatment options. After knowing all the treatment options and their prognosis, the patient was more inclined toward undergoing a single surgery. After admission, definitive treatment was carried out within about 10 h of injury. A lateral skin incision was made starting from distal and lateral to anterosuperioriliac spine and curved distally and posteriorly over the greater trochanter. Interval between gluteus medius and tensor fascia lata was located (Watson-Jones approach). The anterior capsule was incised longitudinally. Acetabulum was found to be empty. A button hole through the anterior-inferiorcapsule was noted. The head and neck found to be dislocated and lying close to obturator foreman. Head and neck was retrieved and the articular surface of the femoral head showed the medium-sized chondral defect. Keeping in mind the size of chondral defect, the decision was made to perform an uncemented total hip arthroplasty. An uncemented total hip arthroplasty was performed with standard surgical technique (Fig. 2). Post-operative period was uneventful and the patient was mobilized weight-bearing as tolerated with walker. He was discharged on the 5th post-operative day. He regained pain-free good range of motion over a period of 6 weeks.
Patient and family members were consulted and detailed discussion was done regarding the type of injury and the possible treatment options. After knowing all the treatment options and their prognosis, the patient was more inclined toward undergoing a single surgery. After admission, definitive treatment was carried out within about 10 h of injury. A lateral skin incision was made starting from distal and lateral to anterosuperioriliac spine and curved distally and posteriorly over the greater trochanter. Interval between gluteus medius and tensor fascia lata was located (Watson-Jones approach). The anterior capsule was incised longitudinally. Acetabulum was found to be empty. A button hole through the anterior-inferiorcapsule was noted. The head and neck found to be dislocated and lying close to obturator foreman. Head and neck was retrieved and the articular surface of the femoral head showed the medium-sized chondral defect. Keeping in mind the size of chondral defect, the decision was made to perform an uncemented total hip arthroplasty. An uncemented total hip arthroplasty was performed with standard surgical technique (Fig. 2). Post-operative period was uneventful and the patient was mobilized weight-bearing as tolerated with walker. He was discharged on the 5th post-operative day. He regained pain-free good range of motion over a period of 6 weeks.
Discussion
Anterior hip dislocation with ipsilateral fracture neck of femur is a rare injury. An attempt of closed reduction of this type of injuries can further damage the retinacular vessels resulting in definite devascularization [5, 6]. The treatment of such injuries is essentially surgical because the reduction of the button holed femoral head back into acetabulum by a closed maneuver is almost impossible once the neck has lost continuity with the shaft [2, 7]. The biggest dilemma a surgeon faces after open reduction of the femoral head into acetabulum is whether to preserve the head or replace it. There are no clear recommendations in literature regarding the management of this type of injuries. The proponents of preserving the head think that it restores the natural bone stock and avoids the future complications of implant loosening and revision arthroplasty. Furthermore, arthroplasty can be carried out any time later if complications such as nonunion, avascular necrosis, or degenerative arthritis occur [8, 9].While head preservation seems logical for younger patients, but it can lead to increase in morbidity and mortality in elderly patients due to the possible requirement of another surgery if complications such as nonunion, avascular necrosis, or arthritis develop. The proponents of replacing the head think that it is a definitive procedure, especially for elderly patients, keeping in mind the high risk of avascular necrosis of femoral head and nonunion.
Literature(Table1)
On literature search, we could identify 8 articles on obturator dislocation with ipsilateral neck femur fracture reporting 5 men and 3 women with average age of the patient was 31.4 (17–48) years. The majority of the cases were treated with open reduction (7 out of 8) and various type of head preservation or head replacement procedures were carried out. Only one case was reduced with closed reduction method aided with Schanz p in and dynamic hip screw fixation was done. This observation clarifies the fact that closed reduction is almost impossible once the neck has lost continuity with the shaft [2, 7]. The single case where the closed reduction was done with the aid of Schanz pin had associated intertrochanteric fracture with comparatively large proximal fragment as compared to neck femur fracture in rest of the cases, which could have made the closed reduction possible. Any attempt of closed reduction in cases of fracture neck femur with obturator dislocation could have disrupted the remaining retinacular vessels resulting in definite devascularization and poor outcome[5, 6].
 Another point of debate in obturator dislocation and ipsilateral fracture neck femur is the approach to be used. Review of literature shows that majority of the cases cited were approached through anterolateral or lateral exposure [2, 4, 7, 10, 11, 12] and very few were approached through posterolateral approach [13]. The possible reason to use anterolateral or lateral approach by most of the authors could be due to the anteriorly lying femoral head and neck fragment. It is easier to approach anteriorly lying head through anterolateral or lateral approach rather than going through posterolateral approach and disturbing the posterior structures also. Tannast et al. [3]described head preserving surgery based on the structural integrity of medial femoral circumflex artery (MFCA) through posterolateral approach by performing trochanteric flip osteotomy and a Z-shaped capsulotomy. However, the lack of any intraoperative modality to confirm the intactness of MFCA can result in avascular necrosis. Five out of 8 reported cases of obturator dislocation with associated neck femur fracture had osteochondral injuries. 3 out of these 5 cases underwent head replacement surgery while two underwent head preserving surgery. One patient with head preserving surgery developed avascular necrosis of femoral head at 22-month follow-up and while other was doing good functionally except the formation of moderate heterotrophic ossification of the affected hip at 4-year followup. The three patients who underwent head replacement surgery were functionally well from 6months to 5-year follow-up except one patient had restriction of internal rotation but was able to carry out all the activities unassisted. Associated femoral head osteochondral injuries may result in degenerative arthritis. DeLee et al. [14] noted that an indentation fracture of more than 4 mm in femoral head results in degenerative arthritis. Fissures and indentations of femoral head have been implicated as a cause of avascular necrosis of femoral head [5,15]. In the case mentioned above, because there was a medium-sized chondral defect and patient was not willing to take any chance to undergo another surgery in the near future, the uncemented total hip replacement was performed.
Another point of debate in obturator dislocation and ipsilateral fracture neck femur is the approach to be used. Review of literature shows that majority of the cases cited were approached through anterolateral or lateral exposure [2, 4, 7, 10, 11, 12] and very few were approached through posterolateral approach [13]. The possible reason to use anterolateral or lateral approach by most of the authors could be due to the anteriorly lying femoral head and neck fragment. It is easier to approach anteriorly lying head through anterolateral or lateral approach rather than going through posterolateral approach and disturbing the posterior structures also. Tannast et al. [3]described head preserving surgery based on the structural integrity of medial femoral circumflex artery (MFCA) through posterolateral approach by performing trochanteric flip osteotomy and a Z-shaped capsulotomy. However, the lack of any intraoperative modality to confirm the intactness of MFCA can result in avascular necrosis. Five out of 8 reported cases of obturator dislocation with associated neck femur fracture had osteochondral injuries. 3 out of these 5 cases underwent head replacement surgery while two underwent head preserving surgery. One patient with head preserving surgery developed avascular necrosis of femoral head at 22-month follow-up and while other was doing good functionally except the formation of moderate heterotrophic ossification of the affected hip at 4-year followup. The three patients who underwent head replacement surgery were functionally well from 6months to 5-year follow-up except one patient had restriction of internal rotation but was able to carry out all the activities unassisted. Associated femoral head osteochondral injuries may result in degenerative arthritis. DeLee et al. [14] noted that an indentation fracture of more than 4 mm in femoral head results in degenerative arthritis. Fissures and indentations of femoral head have been implicated as a cause of avascular necrosis of femoral head [5,15]. In the case mentioned above, because there was a medium-sized chondral defect and patient was not willing to take any chance to undergo another surgery in the near future, the uncemented total hip replacement was performed.
Conclusion
Fracture pattern combining obturator dislocation and ipsilateral fracture neck femur is a rare injury. Although both head preservation and replacement methods of treatment are available, the choice of treatment depends on the duration of injury, age of the patient, associated femoral head chondral injuries, and the choice of the patient. Anterolateral or lateral approach help to deal with the anteriorly lying head in a better way as compared to the posterolateral approach.
Clinical Message
Obturator dislocation of the hip with ipsilateral neck femur fracture is a rare injury. The treatment of such injuries depends on multiple factors such as time since injury, age of the patient, associated injuries, and patient’s choice. It is easier to approach anteriorly lying femoral head and neck through anterolateral or lateral approach.
References
1. Epstein HC, Harvey JP Jr. Traumatic anterior dislocations of the hip: Management and results. An analysis of fifty-five cases. J Bone Joint Surg [Am] 1972;54:1561-2.
2. Sadler AH, DiStefano M. Anterior dislocation of the hip with ipsilateralbasicervical fracture. A case report. J Bone Joint Surg Am 1985;67:326-9.
3. Tannast M, Mack PW, Klaeser B, Siebenrock KA. Hip dislocation and femoral neck fracture: Decision-making for head preservation. Injury 2009;40:1118-24.
4. Izquierdo RJ, Harris D. Obturator hip dislocation with sub capital fracture of the femoral neck. Injury 1994;25:108-10.
5. Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. ClinOrthopRelat Res 1985;9-17.
6. Polesky RE, Polesky FA. Intrapelvic dislocation of the femoral head following anterior dislocation of the hip. A case report. J Bone Joint Surg Am 1972;54:1097-8.
7. Allagui M, Touati B, Aloui I, Hamdi MF, Koubaa M, Abid A. Obturator dislocation of the hip with ipsilateral femoral neck fracture: A case report. J ClinOrthop Trauma 2013;4:143-6.
8. Klasen HJ, Binnendijk B. Fracture of the neck of the femur associated with posterior dislocation of the hip. J Bone Joint Surg Br 1984;66:45-8.
9. Henderson L, Johnston A, Mockford B, Craig B. Posterior hip dislocation and ipsilateral isolated femoral neck fracture: A novel fixation method. J Surg Case Rep 2012;2012:14.
10. Dümmer RE, Sanzana ES. Hip dislocations associated with ipsilateral femoral neck fracture. IntOrthop 1999;23:353-4.
11. Esenkaya I, Görgeç M. Traumatic anterior dislocation of the hip associated with ipsilateral femoral neck fracture: A case report. ActaOrthopTraumatolTurc 2002;36:366-8.
12. Jain S, Haughton BA, Grogan RJ. Inferior dislocation of the hip: A case report and literature review. J OrthopSurg (Hong Kong) 2015;23:123-6.
13. McClelland SJ, Bauman PA, Medley CF Jr, Shelton ML. Obturator hip dislocation with ipsilateral fractures of the femoral head and femoral neck. A case report. ClinOrthopRelat Res 1987;164-8.
14. DeLee JC, Evans JA, Thomas J. Anterior dislocation of the hip and associated femoral-head fractures. J Bone Joint Surg Am 1980;62:960-4.
15. Brown RF, Simmonds FA. An unusual dislocation of the hip. Br J Surg 1972;59:326-8.
16. Singh R, Sharma SC, Goel T. Traumatic inferior hip dislocation in an adult with ipsilateral trochanteric fracture. J Orthop Trauma 2006;20:220-2.
 |
 |
 |
| Dr. Sumit K Jain | Dr. Parit Aggarwal | Dr. Arun Yadav |
| How to Cite This Article: Jain SK, Aggarwal P, Yadav A. Obturator Dislocation of Hip with Ipsilateral Fracture Neck Femur-A Case Report. Journal of Orthopaedic Case Reports 2017 Sep-Oct ; 7(5): 16-19. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


