
[box type=”bio”] What to Learn from this Article?[/box]
Compression of LACN should be considered as a cause of anterior elbow pain when other common pathology are excluded.
Case Report | Volume 7 | Issue 5 | JOCR September – October 2017 | Page 63-66| Sean M Booth, Abdulbaset Abosala, Chris Peach. DOI: 10.13107/jocr.2250-0685.898
Authors: Sean M Booth[1], Abdulbaset Abosala[2], Chris Peach[1]
[1] Department of Orthopaedics, University Hospital South Manchester, UK, 2Department of Orthopaedics, Dr Gray’s Hospital, NHS Grampian, IV30 1SN, UK.
Address of Correspondence:
Dr. Abdulbaset Abosala,
Department of orthopaedics, Dr Gray’s Hospital,
IV30 1SN, NHS Grampian, UK.
E-mail: abosala@hotmail.com
Abstract
Introduction: The complex anatomy and biomechanics of the elbow joint can lead to diagnostic uncertainty when a clinician is determining the cause of a patient’s anterior elbow pain. We present a case of anterior elbow pain with an uncommon and often overlooked etiology. Elbow pain due to compression of the lateral antebrachial nerve (LACN) has an unknown incidence or prevalence.
Case Report: A 27-year-old left-hand dominant male presented to our orthopedic elbow clinic complaining of bilateral elbow clicking and discomfort which had been present for several years. His painful symptoms were localized to the anterior aspect of both elbows and had slowly become more painful despite simple analgesia and physiotherapy. Examination revealed the full range of movement of both elbows with no instability or weakness. Plain imaging and magnetic resonance imaging scans of both elbows did not reveal any pathology, and the decision was made to explore the right elbow, as this was the most symptomatic. Under general anesthesia with tourniquet an anterior curvilinear antecubital fossa incision was made. The lateral border of the distal biceps tendon showed evidence of compression of the LACN at the musculotendinous junction. The tendon was partially resected, and the nerve confirmed to move freely without further entrapment. At 4 weeks after surgery, he was completely asymptomatic. The patient was later listed to undergo a similar procedure to the left side; however, he could not go ahead with surgery so far due to work commitment.
Conclusion: Entrapment or compression of the LACN is an uncommon and often misdiagnosed differential diagnosis with patients presenting with anterior elbow pain, which can lead to permanent neurological damage if left untreated. A high index of suspicion is required to enable prompt diagnosis and investigation as surgical treatment has a high success rate, often with complete resolution of symptoms.
Keywords: Elbow, nerve compression syndromes, musculoskeletal nerve, nerve entrapment.
Introduction
The complex anatomy and biomechanics of the elbow joint can lead to diagnostic uncertainty when a clinician is determining the cause of a patient’s anterior elbow pain. Key features to illicit include the onset of symptoms, exacerbating movements, occupation, and hobbies in addition to focused physical examination with resistance testing. Plain radiography has uses in acute presentations showing fractures or joint effusions and in more chronic settings revealing changes of the osteochondral degenerative disease. Magnetic resonance imaging (MRI) can be used primarily in investigating chronic symptoms. A less costly imaging modality is ultrasound, which has the added benefit of allowing for dynamic testing. This is particularly useful in cases where symptoms are maximal on elbow movement as is commonly the case in anterior elbow pain. The differential diagnosis includes biceps tendinopathy, partial thickness tears of the distal biceps tendon, brachialis tendinitis, capsular strain, pronator syndromes, gout, arthritis, radial tunnel syndrome, lateral epicondylitis, and C6 radiculopathy. We present a case of anterior elbow pain with an uncommon and often overlooked etiology. Compression of the lateral antebrachial nerve (LACN) causing elbow pain has an unknown incidence or prevalence. The largest published case series to date involves 17 patients [1].
Case Report
A 27-year-old left-hand dominant male presented to our orthopedic elbow clinic complaining of bilateral elbow clicking and discomfort which had been present for several years. His painful symptoms were localized to the anterior aspect of both elbows and had slowly become more painful despite simple analgesia and physiotherapy treatments. He also described intermittent paraesthesia in the forearm, in particular after physical activity with the arm. The pain was exacerbated when working out in the gym, in particular with pull-ups, and while heavy lifting as a storeman. He was otherwise fit and well.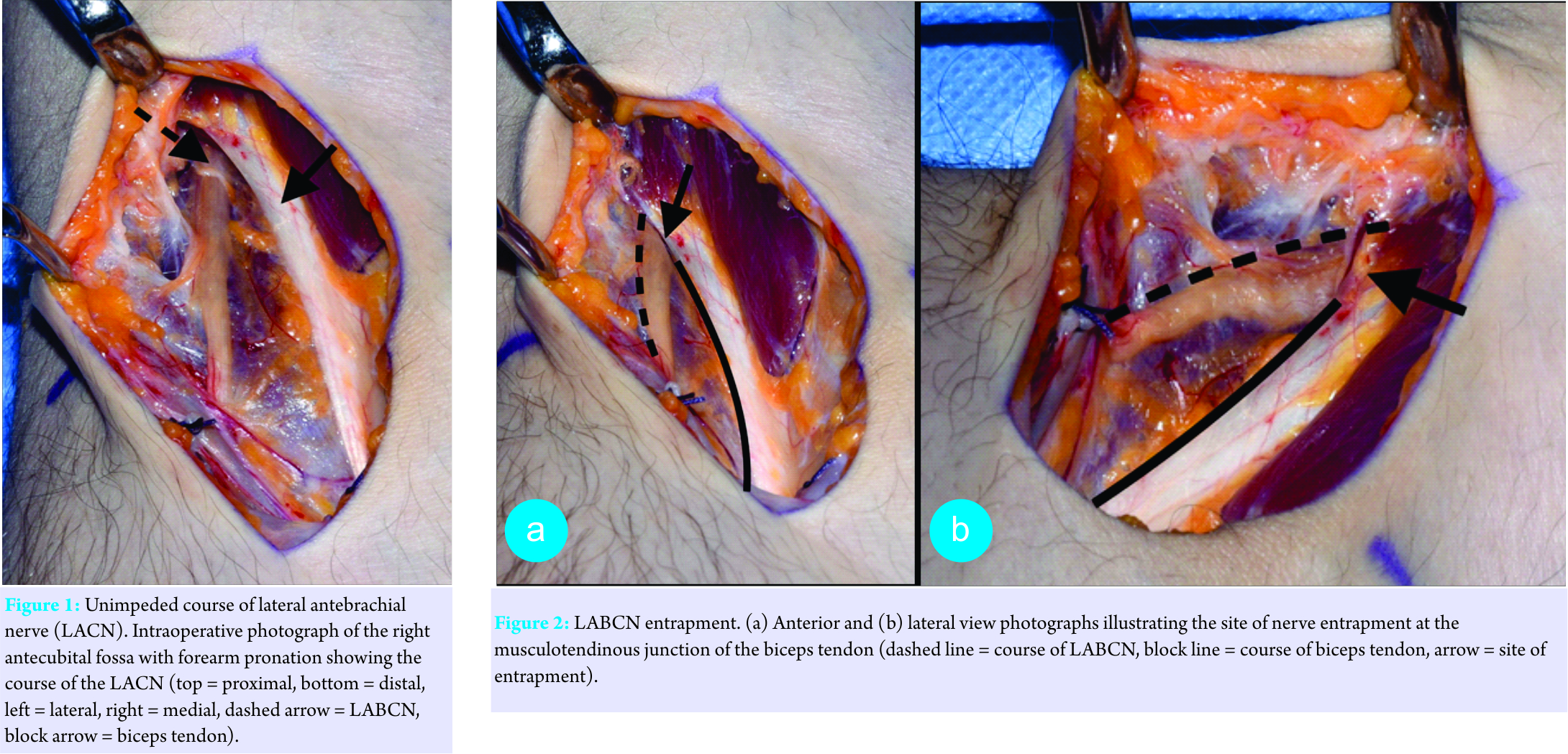
Examination revealed the full range of movement of both elbows with no instability or weakness. Grip and grind tests were negative for pain bilaterally. There was no objective sensory disturbance, and Tinel’s sign was negative. Hook test for distal biceps rupture was negative and provocative testing of the biceps produced no pain. While moving the joint on the left side, a clicking sensation could be palpated over the lateral aspect of the biceps tendon that reduced digital pressure.
Plain imaging and MRI scans of both elbows did not reveal any pathology, and the decision was made to explore the right elbow, as this was the most symptomatic.
Under general anesthesia with tourniquet, an anterior curvilinear antecubital fossa incision was made. The lateral border of the distal biceps tendon showed evidence of compression of the LACN at the musculotendinous junction in forearm supination as illustrated in Fig. 1 and 2. The tendon was partially resected, and the nerve confirmed to move freely without further entrapment (Fig. 3). An associated partial thickness tear of the long head of biceps distal hemitendon was debrided endoscopically. Postoperatively the patient was allowed an immediate gentle range of movement in a polysling. At 4 weeks after surgery, he was completely asymptomatic.
The patient has given written consent for intraoperative images to be used for medical teaching.
Discussion
The LACN is the peripheral sensory nerve of the musculocutaneous nerve, itself the continuation of the lateral cord of the brachial plexus. Running under cover of the lateral border of the biceps tendon, the nerve emerges from the anterior surface of brachialis just lateral to biceps tendon at the level of interepicondylar line [2]. It traverses the antecubital fossa deep to and between the median cubital and cephalic veins becoming subcutaneous after it pierces the antebrachial fascia. It then divides into an anterior and posterior branch which provides sensation to one-third of the anterior and posterior forearm, respectively [3]. As with other cutaneous nerves considerable anatomical variations exist with one study reporting the nerve piercing the fascia an average of 3.5 cm proximal to the lateral epicondyle and cases where the nerve pierced the biceps muscle belly itself and another stating it emerged from the lateral border of biceps tendon 2–4 cm above the elbow crease [4, 5].
Proximal to the elbow crease the nerve can become entrapped by the lateral border of biceps tendon or aponeurosis and compressed between biceps aponeurosis and brachialis fascia with the elbow extended and pronated [6, 7]. One study demonstrated that entrapment by the lateral border of the biceps is worse in supination most likely due to active compression of the biceps muscle [1]. This mechanism matches our patient’s symptoms, as he was most symptomatic when performing biceps curls and pull-ups and he had recently developed significant muscular bulk in the gym. There has been one case report of compression distal to the skin crease by a fibrous band and one of an aberrant brachial fascia band compressing the nerve in the antecubital fossa [8, 9].
Typical symptoms consist of anterior elbow pain and paraesthesia from the elbow, along with the forearm to base of the thumb in the distribution of the anterior and posterior branches. The onset can be acute after a twisting injury or more insidious in onset and progressively worsens with continued elbow usage. Clinical examination often reveals a normal range of movement, positive compression test exacerbating symptoms when pressing over the LABCN just lateral to the biceps tendon and pain on resisted elbow flexion and forearm supination. If left untreated, permanent neurological deficit and chronic pain can result [6].
Electromyography and nerve conduction studies rarely help with the diagnosis as it is often clinical, having a high index of suspicion and by excluding other causes [5]. Patients with LACN compression have characteristic features detectable on ultrasound which include: Nerve enlargement, increased echogenicity, and loss of the usual honeycomb fascicular pattern [10]. They are frequently associated with distal biceps tendon tears as in our case. Ultrasound can also be used to guide perineural injections for the purpose of diagnostic and therapeutic advantages. A relatively new technique of MR neurography uses high-resolution thin slice acquisition of peripheral nerves and can detect areas of entrapment [11].
Conservative measures include elbow splinting and anti-inflammatory medication. Focused ultrasound guided injections can be helpful in some cases if symptoms persist. If symptoms progress despite this, then surgical decompression is necessary. The three largest case series of operative intervention involve 40 patients in total. Davidson et al. report complete resolution of symptoms in 15 patients, with average, follow-up of 13 years, after wedge tenotomy of the lateral edge of the distal biceps tendon [12]. Dailiana et al. operated on eight nerves with follow-up of 5.5 years [5]. All had a resolution of symptoms bar one who has an associated neuroma. The authors released the nerve from the fascia in those patients without an associated biceps injury and only performed tenotomy in those with severe compression. They were able to perform the procedure through transverse incisions in some enabling a better esthetic result. The most recent published series by Naam and Massoud describes 17 operative cases with wedge resections of the biceps tendon with average follow-up of 45 months [1]. They reported 14 patients had complete resolution of symptoms and the rest all had some degree of improvement. One reported variation in technique is to perform a wedge reflection rather than resection [13].
Conclusion
Entrapment or compression of the LACN is an uncommon and often misdiagnosed differential diagnosis with patients presenting with anterior elbow pain, which can lead to permanent neurological damage if left untreated. A high index of suspicion is required to enable prompt diagnosis and investigation as surgical treatment has a high success rate, often with complete resolution of symptoms.
Clinical Massage
The diagnosis of anterior elbow pain is too often difficult. With normal investigation including, nerve conduction study, MRI and ultrasound, in addition to failed conservative treatment, the compression of LANC should be considered.
References
1. Naam NH, Massoud HA. Painful entrapment of the lateral antebrachial cutaneous nerve at the elbow. J Hand Surg Am 2004;29:1148-53.1. Naam NH, Massoud HA. Painful entrapment of the lateral antebrachial cutaneous nerve at the elbow. J Hand Surg Am 2004;29:1148-53.
2. Bourne MH, Wood MB, Carmichael SW. Locating the lateral antebrachial cutaneous nerve. J Hand Surg Am 1987;12:697-9.
3. Bassett FH 3rd, Nunley JA. Compression of the musculocutaneous nerve at the elbow. J Bone Joint Surg Am 1982;64:1050-2.
4. Rosen JE, Rokito AS, Khabie V, Zuckerman JD. Examination of the lateral antebrachial cutaneous nerve: An anatomic study in human cadavers. Am J Orthop (Belle Mead NJ) 1998;27:690-2.
5. Dailiana ZH, Roulot E, Le Viet D. Surgical treatment of compression of the lateral antebrachial cutaneous nerve. J Bone Joint Surg Br 2000;82:420-3.
6. Waldman SD. Lateral Antebrachial Cutaneous Nerve Entrapment at the Elbow. In: Atlas of Common Pain Syndromes. 3rd ed. Philadelphia, PA: Saunders; 2012. p. 149-50.
7. Seoighe DM, Baker JF, Mulhall KJ. Surgical trainees neuropraxia? An unusual case of compression of the lateral cutaneous nerve of the forearm. Orthop Traumatol Surg Res 2010;96:603-5.
8. Belzile E, Cloutier D. Entrapment of the lateral antebrachial cutaneous nerve exiting through the forearm fascia. J Hand Surg Am 2001;26:64-7.
9. Paraskevas G, Tsitsopoulos PP, Papaziogas B, Natsis K, Kitsoulis P. Evidence of lateral antebrachial cutaneous nerve entrapment during autopsy. Folia Morphol (Warsz) 2008;67:218-20.
10. Chiavaras MM, Jacobson JA, Billone L, Lawton JM, Lawton J. Sonography of the lateral antebrachial cutaneous nerve with magnetic resonance imaging and anatomic correlation. J Ultrasound Med 2014;33:1475-83.
11. Yung H, Lagemann GM, Lin A, Orebaugh SL, Cortazzo MH. Lateral antebrachial cutaneous nerve entrapment after shoulder arthroscopy: A Case report. PM R 2015;7:889-94.
12. Davidson JJ, Bassett FH 3rd, Nunley JA 2nd. Musculocutaneous nerve entrapment revisited. J Shoulder Elbow Surg 1998;7:250-5
13. Gillingham BL, Mack GR. Compression of the lateral antebrachial cutaneous nerve by the biceps tendon. J Shoulder Elbow Surg 1996;5:330-2.
 |
| Dr. Sean M Booth |
| How to Cite This Article: Booth SM, Abosala A, Peach C. Anterior Elbow Pain Caused by Compression of the Lateral Antebrachial Cutaneous Nerve. Journal of Orthopaedic Case Reports 2017 Sep-Oct ; 7(5):63-66 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


