
[box type=”bio”] Learning Points for this Article: [/box]
Spinal gout should be considered as one of the differential diagnosis in patients who have multiple risk factors for gout and present with back problems.
Case Report | Volume 7 | Issue 6 | JOCR November – December 2017 | Page 50-54| Wesley Ng, Cheuk Hang Sin, Chong Hing Wong, Wing Fat Chiu, On Ming Chung. DOI:10.13107/jocr.2250-0685.946
Authors: Wesley Ng [1], Cheuk Hang Sin [1], Chong Hing Wong [1], Wing Fat Chiu [1], On Ming Chung [1]
[1] Department of Orthopaedics and Traumatology, Princess Margaret Hospital, Hong Kong.
Address of Correspondence:
Dr. Wesley Ng, Resident, Princess Margaret Hospital, Department of Orthopaedics and Traumatology, 2-10 Princess Margaret Hospital Road, Lai Chi Kok, Kowloon, Hong Kong.
E-mail: wesleyng1000@gmail.com
Abstract
Introduction: Gouty spondyloarthropathy is generally believed to be uncommon. Together with the fact that it can mimic a variety of disease entities, it imposes significant diagnostic challenge in our clinical practice. In this article, we report two patients diagnosed with spinal gout, and both were initially suspected to have a pyogenic infection.
Case Reports: The first patient, a 66-year-old man, was admitted for fever and a short history of bilateral upper limb weakness. Clinical, biochemical, and radiological investigation results were suggestive of C5/6 infective spondylodiscitis with resultant cervical myelopathy. The second patient, a 68-year-old man, was admitted for fever and bilateral lower limb weakness and numbness compatible with cauda equina syndrome. Imaging showed L4/5 lytic spondylolisthesis with suspected abscesses formation around the pars defects. Both underwent emergency operations. Histological examinations of intraoperative specimens in both cases revealed tophaceous gout and microbiological studies were all negative. Urate-lowering agent was started for hyperuricemia. They both had partial neurological recovery.
Conclusion: These two cases highlight how axial gout can mimic infective spondyloarthropathy clinically. In patients with multiple risk factors for gout presenting with back conditions, spinal gout should be considered as one of the differential diagnosis. With the availability of advanced imaging modality, dual-energy computed tomography scan, pre-operative diagnosis of axial gout is now possible which may have implications on subsequent surgical approaches and medical treatment. Collaboration with the medical team to achieve good serum urate control is important to prevent disease recurrence.
Keywords: Axial, spine, gout, crystal, tophus, gout imaging, dual-energy computed tomography.
Introduction
Gout is a metabolic disease characterized by deposition of monosodium urate deposition in synovial fluid, most commonly affecting peripheral appendages. It is the most common crystal arthropathy with a global prevalence of 0.08%. The prevalence of gout is still on a rising trend imposing significant health burden on our society. Spinal involvement is generally believed to be uncommon. However, this belief has been challenged by some recent publications that spinal gout might be more common than we previously thought [1, 2, 3]. Together with its associated morbidities, it is of clinical importance that we are able to suspect and diagnose axial gout promptly. In this article, we report two patients with gouty spondyloarthropathy which were initially treated as a pyogenic infection. Gout was not suspected in the first place.
Case 1
A 66-year-old man was admitted through emergency department for neck pain, bilateral upper limbs weakness and clumsiness for 1 week. He has a history of Type 2 diabetes mellitus, hypertension and chronic renal insufficiency. He is a chronic drinker. He was febrile on presentation. Physical examination revealed bilateral upper limb weakness with muscle power of Medical Research Council (MRC) Grade 4/5. Hoffmann’s sign was positive, and there was presence of reverse supinator jerk and brisk upper limbs reflexes. Laboratory tests revealed leukocytosis (white cell count 10.5 × 109 /L), elevated C reactive protein level (7.7 mg/L), and elevated creatinine level (222 umol/L) which was similar to his baseline level. X-ray of the cervical spine showed loss of disc height at C5/6 level with adjacent endplate erosions and C5 vertebral body destruction (Fig. 1). In view of suspected C5/6 infective spondylodiscitis, contrast computed tomography (CT) and plain magnetic resonance imaging (MRI) of the cervical spine were performed. On the contrast CT scan, in addition to the bony erosions evident on X-ray, a thin layer of prevertebral fluid was present from C2 to C5 level. No rim enhancing collection was seen. The plain MRI scan showed moderate cervical spondylosis. The cervical cord was also shown to be moderately impinged between the posteroinferior margin of C5 vertebral body and C6 lamina with mild focal myelomalacia changes (Fig. 2). Overall, clinical and radiological features were suggestive of infective spondylodiscitis with resultant cervical myelopathy.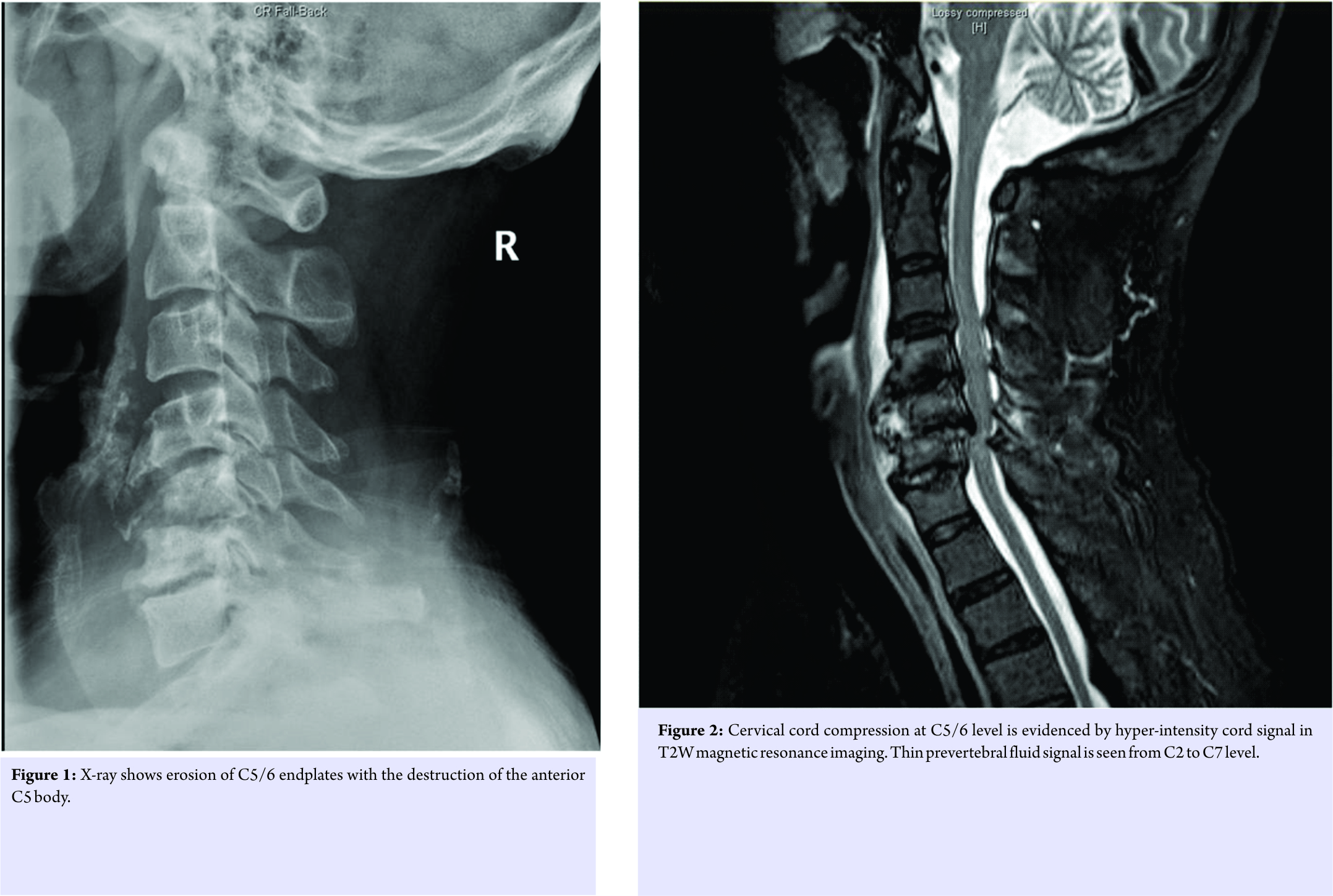
Broad spectrum antibiotic was given empirically. Operation was performed 4 days after admission. Posterior instrumentation with lateral mass screws from C4 to C6 was performed first with the patient in prone position. He was then turned to supine position for anterior approach to the cervical spine. During the anterior approach, thickened prevertebral tissue over C5 was noted with purulent fluid inside. Intraoperative frozen section showed crystal deposition with no sign of malignancy or frank infection. C5 corpectomy with tricorticate bone graft harvested from left iliac crest was performed (Fig. 3a and b). A rigid neck collar was given postoperatively. Cultures for bacteria, mycobacterium, and fungus were all negative. Histological examination revealed foreign body reaction and aggregates of needle-shaped crystals with negative birefringence under polarizing microscopy. Tophaceous gout was diagnosed. The empirical antibiotic was stopped in view of histological diagnosis of axial gout with negative microbiological studies. Postoperative recovery was uneventful. Serum urate level was found to be elevated to 0.45 mmol/L (normal range: 0.21–0.43 mmol/L). There was no previous history of gouty arthritis or clinical evidence of peripheral gouty tophus. Dietary restriction was advised and allopurinol was started at low dose 50 mg daily in view of chronic kidney disease. He underwent further rehabilitation and was discharged 7 weeks after the operation. 11 months after the surgery, he had a fair functional recovery. However, there was still residual upper limb weakness which affected his daily function. Radiologically, there was satisfactory fusion at the corpectomy site. There was no graft subsidence or displacement. He developed delayed hypersensitivity reaction to all opurinol with intolerable pruritis and skin rash. All opurinol was stopped as a result. He had been referred to an endocrinologist for consideration of another urate-lowering agent.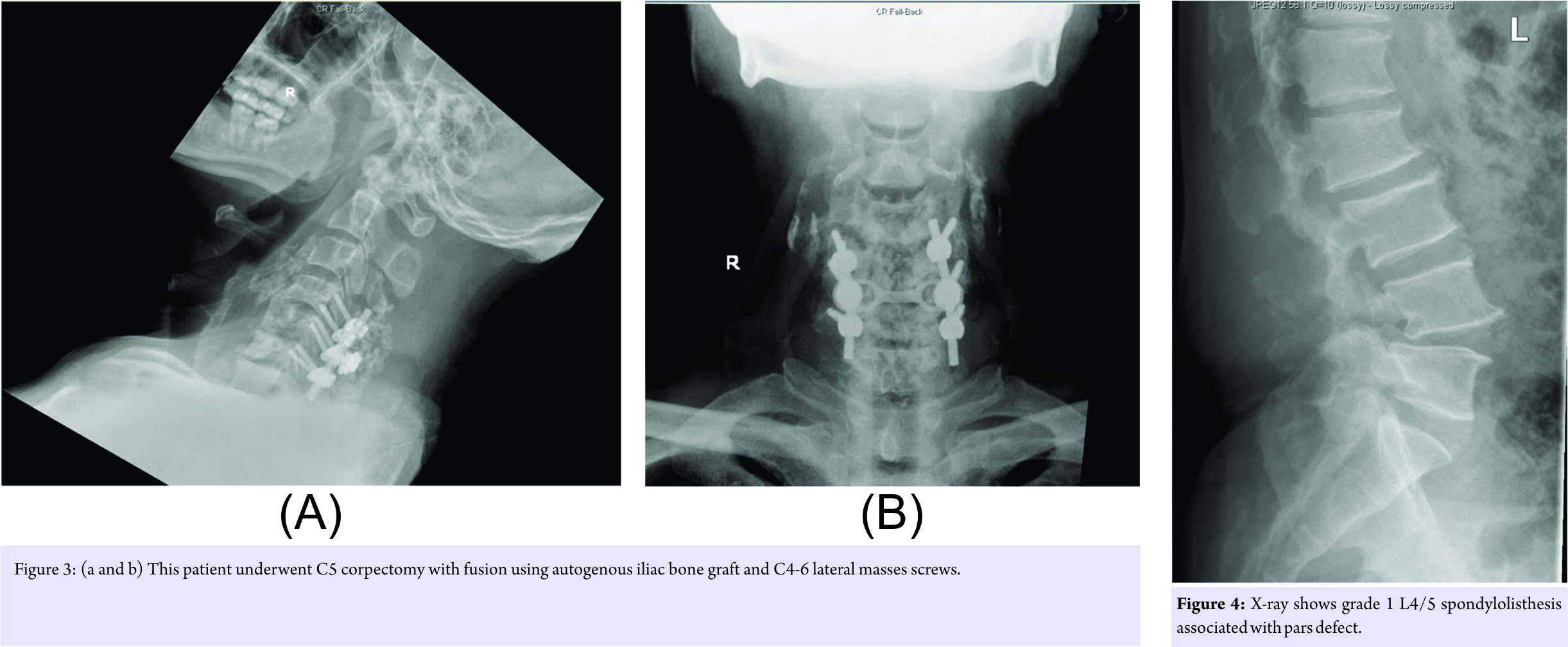
Case 2
A 68-year-old man was admitted through emergency department for 2-month history of low back pain with recent exacerbation associated with bilateral lower limb weakness and numbness. There was an episode of acute left middle finger proximal interphalangeal joint arthritis 1 week before this admission. He was treated as gouty arthritis with colchicine as blood test revealed hyperuricemia of 0.54 mmol/L. He was febrile on admission. There was bilateral lower limb motor weakness with MRC Grade of 4/5, and paresthesia of bilateral legs and feet. He developed acute retention of urine after admission. X-ray of lumbosacral spine showed L4/5 spondylolisthesis with pars defect and severe lumbar spondylosis (Fig. 4). Laboratory tests showed elevated white cell count of 17.9 × 109/L (neutrophilic predominance) and C reactive protein of 197 mg/L. He also had a renal impairment with creatinine level of 136 umol/L. Urgent contrast MRI lumbosacral spine was performed. It showed prominent enhancing epidural soft tissue signals around bilateral L4/5 pars defects causing severe stenosis of the central spinal canal and bilateral intervertebral foramina and hence cauda equina compression. There were associated ill-marginated posterior paraspinal enhancing soft tissue signals from L3 to L5 and multiple small rims are enhancing collections (Fig. 5a and b).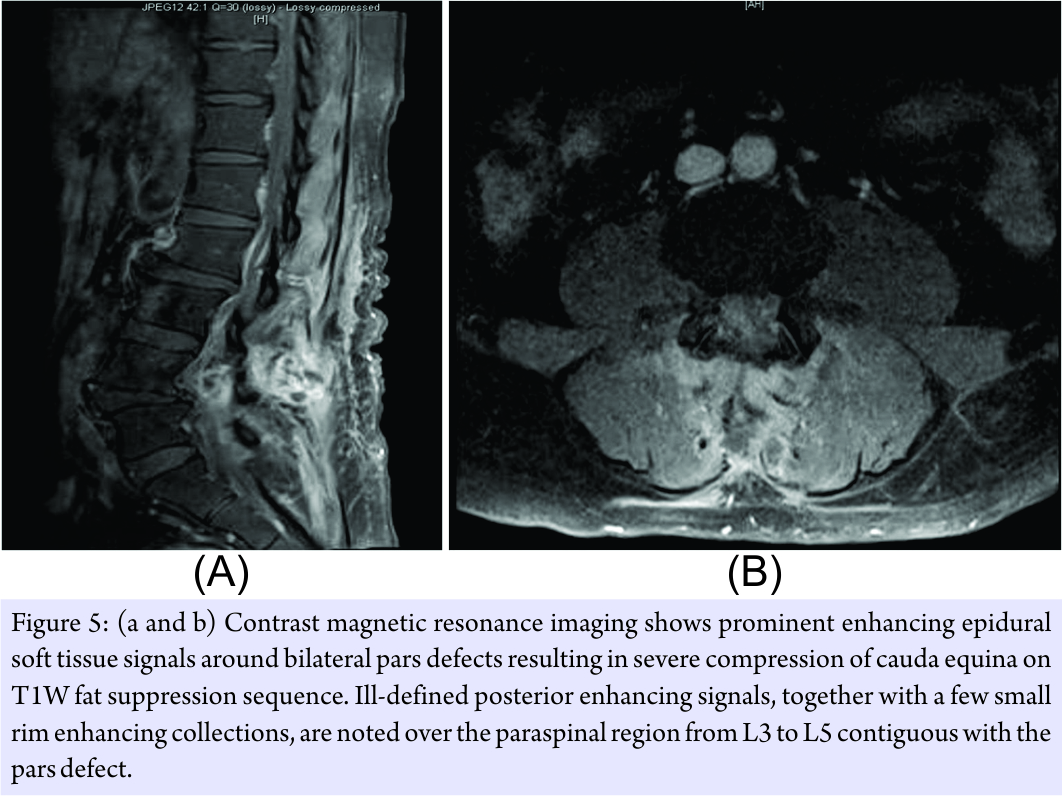
With a clinical diagnosis of infective spondylolysis of L4/5 with cauda equina syndrome, emergency operation was arranged. Intraoperatively, a large amount of crystal deposition was noted around both spondylolytic sites, ligamentum flavum, interspinous, and supraspinous ligament. The interspinous and supraspinous ligaments were eroded by the tophi. Debridement of the tophi and ligamentum flavum was performed with adequate decompression achieved. No purulent fluid or abscess was found. Small amount of tophaceous material was left behind due to dense adhesion to the dura mater. Pathological examination of the specimen revealed fibrillary eosinophilic material surrounded by multinucleated giant cells, consistent with gouty tophus. Bacterial cultures were negative. Despite good recovery of sphincter function, there was residual lower limbs weakness, and he needed to walk with a frame. Allopurinol was started at 100 mg daily and gradually titrated upward to 300 mg daily to achieve serum urate target. Follow-up MRI 16 months after the operation revealed no radiological evidence of reaccumulation of gouty tophus.
Discussion
Axial gout is a great mimicker of various clinical conditions. Patients can present with acute back pain with inflammatory symptoms and signs mimicking infective spondylodiscitis as in our cases. Atlantoaxial subluxation due to tophaceous gout mimicking rheumatoid arthritis has also been reported [1]. It is associated with various degrees of neurological involvement including cervical myelopathy or lumbar radiculopathy [4, 5, 6, 7]. In general, cervical spine involvement is much rarer than lumbar spine. As far as spinal gout is concerned, hyperuricemia is the single most characteristic laboratory finding. Urate level was elevated in both of our patients. This coincides with the literature finding that nearly 80% of patients with spinal gout were found to have elevated serum urate level [8]. However, we need to interpret the serum urate result carefully because serum urate level may be normal in acute inflammatory phase due to increased renal excretion of urate. It is suggested by latest guideline for diagnosis of gout that serum urate should be repeated 4 weeks after an acute episode unless the initial urate is higher than 0.60 mmol/L [9]. It has a bearing on subsequent medical treatment. Imaging plays an important role in investigating patients with spinal gout. While the commonly used imaging modalities, e.g., contrast CT or MRI could hint the diagnosis of axial gout, they are not specific enough for detection of urate crystal deposition. In our patients, CT and MRI failed to differentiate gouty tophus from abscess even by experienced radiologists. In clinical practice, we often have to rely on invasive investigations such as image-guided needle biopsy or even surgical biopsy to establish the diagnosis. The newly innovated dual-energy CT (DECT) emerges as a promising imaging modality in the identification and even volumetric quantification of gouty tophus. It has been shown to be both sensitive and specific. A meta-analysis of 11 studies by Ogdie et al. showed a pooled sensitivity of 87% and specificity of 84% [10]. Positive identification of urate deposition in DECT has already been included as one of the diagnostic criteria of gout [9]. However, most published studies of DECT focused on peripheral joints only. Furthermore, there is known limitation of imaging of the axial skeleton and the large proximal joints, namely, hips or shoulders. In a recent review article by Chou et al. [11], there was no strong validated data in the literature for DECT of the shoulder, hip or spine regions. Another study by Bongartz et al. found a false negative rate of 20% among patients with a first gouty attack or short duration of a symptom of <6 weeks [12]. A logical postulation is that the sensitivity of DECT in the identification of gouty typhus is lower in patients with small tophus burden. Presence of metal implants can also cause artifact leading to false positive results. To conclude, while DECT appeared to be a promising imaging modality, further study is needed to validate its accuracy in patients with spinal gout. In our cases, both patients presented with the severe neurological deficit. With suspicion of infection, urgent operative treatment was indicated. For the first patient, one-stage anterior debridement, decompression, and autogenous bone graft followed by posterior instrumentation were performed. In the second case, simple debridement and decompression were done. In both cases, spinal gout was not initially suspected. In retrospect, both patients did have multiple risk factors for gout including alcoholism, diabetes mellitus, chronic renal impairment, and recent gouty attack. This might have led us to suspect spinal gout as one of the differential diagnosis. Pre-operative diagnosis of spinal gout might have been made by either image-guided needle biopsy or DECT scan which is now available in our center. It may have surgical implication because, in case of pyogenic spondylodiscitis, two-stage procedure, anterior debridement and fusion followed by delayed instrumentation, will be preferred over the one-stage operation in some centers [13]. Furthermore, it may affect the decision of metal cage use during fusion procedure and the decision on whether anterior or posterior instrumentation should be performed. These are all debatable topics in treating septic spondylodiscitis. However, single-stage operation as in our first case appeared to be a safe option to provide immediate stability, satisfactory alignment and infection control even in case of spinal infection [14]. In axial gout, we should remember medical treatment remains the mainstay of treatment as surgery is not curative and can only decrease the tophus burden. Indeed, for the second patient, small amount of tophus could not be debrided in view of its dense adhesion to dura mater. Pharmacologic urate-lowering therapy is recommended for long-term management of patients having tophaceous gout according to guidelines of American College of Rheumatology. Xanthine oxidase inhibitor, namely, allopurinol is the first line medications recommended, and should be started at a low dose, e.g., 100 mg/day. Serum urate level should be monitored regularly to guide subsequent dosage adjustment. Potential drug toxicity to allopurinol, e.g., rash, elevated hepatic transaminases is not uncommon as occurred in our first patient. In the long run, stringent control of uric acid level below 6 mg/dL is recommended. Any blood level below the saturation point can facilitate urate crystal dissolution. Indeed radiological regression of intraspinal gouty tophi has been observed with medical treatment on serial MRI in reported case series [15].
Conclusion
Both patients reported in this article presented at the late stage of axial gout with severe neurological compromise resulting in an irreversible functional deficit. Indeed, with increasing prevalence of gout, it is believed that spinal gout may be an underestimated source of axial pain. Being able to understand how it manifests is important because it allows us to diagnose and start treatment timely for this reversible condition. Early involvement of medical team is advised. It may help prevent the morbidity as a result of the late presentation of untreated or under-treated spinal gout.
Clinical Message
Axial gout can mimic a variety of spinal conditions clinically, and orthopedic surgeons should be aware of its different clinical presentation. Both surgical and medical treatment plays important roles in spinal gout management.
References
1. de Mello FM, Helito PV, Bordalo-Rodrigues M, Fuller R, Halpern AS. Axial gout is frequently associated with the presence of current tophi, although not with spinal symptoms. Spine (Phila Pa 1976) 2014;39:E1531-6.
2. Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the united states. Part II. Arthritis Rheum 2008;58:26-35.
3. Choi HK, Ford ES, Li C, Curhan G. Prevalence of the metabolic syndrome in patients with gout: The third national health and nutrition examination survey. Arthritis Rheum 2007;57:109-15.
4. Sanmillan Blasco JL, Vidal Sarro N, Marnov A, Acebes Martín JJ. Cervical cord compression due to intradiscal gouty tophus: Brief report. Spine (Phila Pa 1976) 2012;37:E1534-6.
5. Wazir NN, Moorthy V, Amalourde A, Lim HH. Tophaceous gout causing atlanto-axial subluxation mimicking rheumatoid arthritis: A case report. J Orthop Surg (Hong Kong) 2005;13:203-6.
6. Mahmud T1, Basu D, Dyson PH. Crystal arthropathy of the lumbar spine: A series of six cases and a review of the literature. J Bone Joint Surg Br 2005;87:513-7.
7. King JC, Nicholas C. Gouty arthropathy of the lumbar spine: A case report and review of the literature. Spine (Phila Pa 1976) 1997;22:2309-12.
8. Toprover M, Krasnokutsky S, Pillinger MH. Gout in the spine: Imaging, diagnosis, and outcomes. Curr Rheumatol Rep 2015;17:70.
9. Neogi T, Jansen TL, Dalbeth N, Fransen J, Schumacher HR, Berendsen D, et al 2015 gout classification criteria: An American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis 2015;74:1789-98.
10. Ogdie A, Taylor WJ, Weatherall M, Fransen J, Jansen TL, Neogi T, et al. Imaging modalities for the classification of gout: Systematic literature review and meta-analysis. Ann Rheum Dis 2015;74:1868-74.
11. Chou H, Chin TY, Peh WC. Dual-energy CT in gout – A review of current concepts and applications. J Med Radiat Sci 2017;64:41-51.
12. Bongartz T, Glazebrook KN, Kavros SJ, Murthy NS, Merry SP, Franz WB 3rd, et al. Dual-energy CT for the diagnosis of gout: An accuracy and diagnostic yield study. Ann Rheum Dis 2015;74:1072-7.
13. Dimar JR, Carreon LY, Glassman SD, Campbell MJ, Hartman MJ, Johnson JR, et al. Treatment of pyogenic vertebral osteomyelitis with anterior debridement and fusion followed by delayed posterior spinal fusion. Spine (Phila Pa 1976) 2004;29:326-32.
14. Park KH, Cho OH, Lee YM, Moon C, Park SY, Moon SM, et al. Therapeutic outcomes of hematogenous vertebral osteomyelitis with instrumented surgery. Clin Infect Dis 2015;60:1330-8.
15. Dhôte R, Roux FX, Bachmeyer C, Tudoret L, Daumas-Duport C, Christoforov B, et al. Extradural spinal tophaceous gout: Evolution with medical treatment. Clin Exp Rheumatol 1997;15:421-3.
 |
 |
 |
| Dr. Wesley NG | Dr. Cheuk Hang Sin | Dr. Chong Hing Wong |
| How to Cite This Article: Ng W, Sin CH, Wong CH, Chiu WF, Chung OM. Unusual Presentation of Spinal Gout: 2 Cases Report and Literature Review. Journal of Orthopaedic Case Reports 2017 Nov-Dec; 7(6): 50-54 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


