
[box type=”bio”] Learning Point for this Article: [/box]
A K wire inserted in the distal femur, after determining the neutral version of the limb and comparing the lesser trochanter profile with the normal side, can be used for determining the version of femoral stem.
Case Report | Volume 8 | Issue 1 | JOCR Jan – Feb 2018 | Page 75-79| Nirmal D Patil, Hiren B Patel, Naushad Hussain, Kalpesh Saidane. DOI: 10.13107/jocr.2250-0685.1008
Authors: Nirmal D Patil[1], Hiren B Patel[1], Naushad Hussain[1], Kalpesh Saidane[1]
[1]Department of Orthopaedics, T.N.M.C and B.Y.L Nair Hospital, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Nirmal D Patil,
Department of Orthopaedics, T.N.M.C and B.Y.L Nair Hospital, Doctor Anandrao Nair Marg, RTO Colony, Mumbai Central, Mumbai, Maharashtra-400008. India.
E-mail: nirmalpatil2008@gmail.com
Abstract
Introduction: Standard references such as knee and lower leg position cannot be used in patients with knee arthrodesis with destroyed distal femur anatomy. The resulting component malposition can culminate in dislocation, decreased range of motion, impingement, and wear. To our knowledge, no cases on surgical techniques have been reported in such patients. We describe a simple technique that guides a surgeon in assessing the femoral stem version in such cases.
Case Report: A 80-year-old female sustained right sided neck of femur fracture. She had a history of bone tumor, which was treated with resection and arthrodesis. Subsequently, the patient developed osteomyelitis which healed gradually. The difficulties, in this case, were inability to flex the knee, to determine the trans-epicondylar axis and to use the ankle as a reference. Using lesser trochanter as reference neutral rotation of the limb was determined and K wire was inserted in distal femur of the patient. A post-operative computed tomography (CT) was done to assess the stem version.
Conclusion: Our main aim in presenting this case was to emphasize on the surgical technique. A pre-operative CT scan should be done to evaluate the distal femur anatomy and calculate the lesser trochanter versions of the normal limb. We recommend the use of K wire inserted into the distal femur after determining the neutral version of the limb and comparing the lesser trochanter profile with the normal side.
Keywords: Knee arthrodesis, femoral anteversion, stem anteversion, intraoperative estimation, hemiarthroplasty
Introduction
The techniques for intraoperative assessment of femoral stem version are (1) by measuring the angle between the lower-leg axis and trial stem axis by flexing the knee and placing the tibia vertically [1]. (2) By measuring the angle between the trial stem and the transepicondylar axis [2]. Both these techniques are futile in attempting hip arthroplasty in a patient with ipsilateral knee arthrodesis (flexural limitations of the knee [1]) with destroyed distal femur anatomy. The ankle cannot be used as a guide in these cases, as the rotation of leg with respect to the femur could have been altered during the knee arthrodesis procedure. We face a perilous problem in such cases, which can culminate in component malposition. Component malposition is known to cause dislocation [3], decreased range of movement [4], bony impingement [5], and component wear [6]. We describe a technique that guides a surgeon in assessing the femoral stem version in such cases.
Case Report
A 80-year-old female had a fall and sustained right-sided neck of femur fracture. She had a history of bone tumor 20 years ago (details are not known), which was treated with resection and arthrodesis with a bi-pillar plating at the time of diagnosis. Postoperatively patient developed skin breakdown and discharge of purulent material. She was kept on daily dressing, and 6 months later, the plate was removed, and the limb was immobilized in a posterior knee cast. After wound healed, patient was started gradual weight bearing. On examination, the right limb was in the external rotation and shortened. There was a surgical scar measuring 10 cm on the anterior aspect of the right knee, healed with primary intention. The knee was fixed at 10° of flexion. A radiograph of the pelvis showed a subcapital type of femur neck fracture with a Dorr type C canal (Fig. 1). A radiograph of the knee showed arthrodesis of the knee (Fig. 2).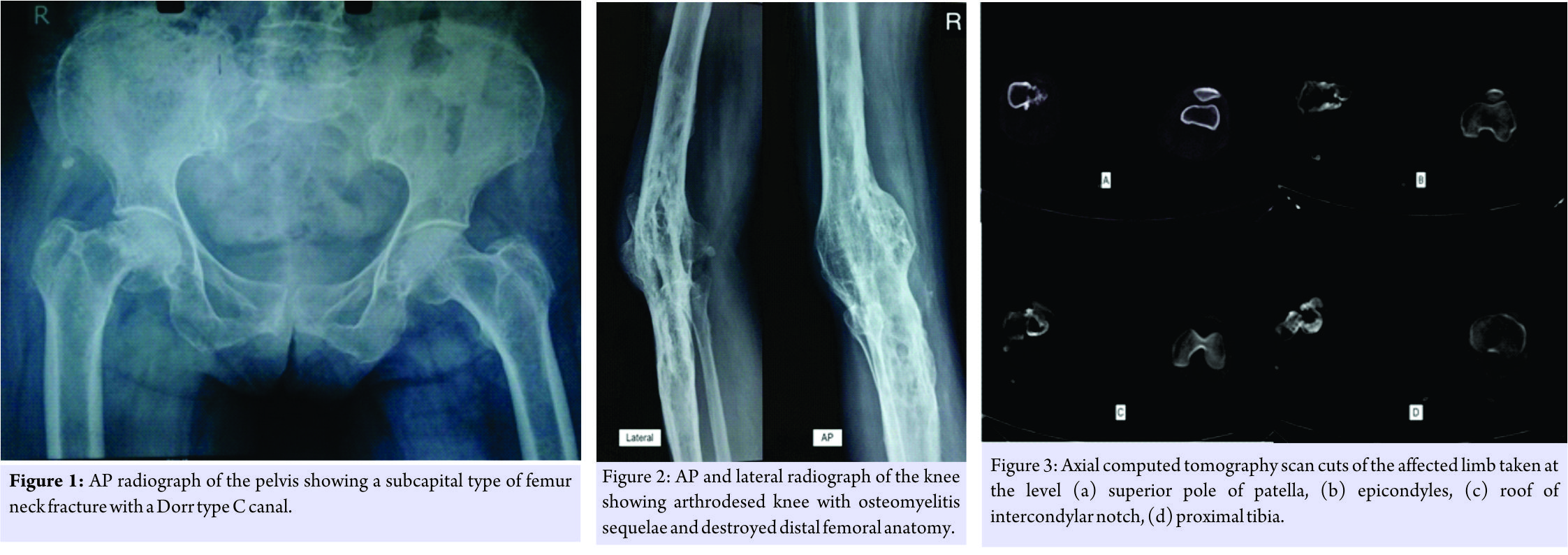 The patella was absent, and the native distal femoral anatomy was distorted. After primary resuscitation, the patient was posted for cemented bipolar hemiarthroplasty. The posterior condyles, medial and lateral epicondyles could not be appreciated on pre-operative computerised tomography (CT) scan (Fig. 3). We decided to use the lesser trochanter as the reference guide for femoral stem version. On CT scan, the version of lesser trochanter with respect to the posterior bicondylar axis and the femur neck was measured on the unaffected side as per the technique described by Imai et al. and Unlu et al.
The patella was absent, and the native distal femoral anatomy was distorted. After primary resuscitation, the patient was posted for cemented bipolar hemiarthroplasty. The posterior condyles, medial and lateral epicondyles could not be appreciated on pre-operative computerised tomography (CT) scan (Fig. 3). We decided to use the lesser trochanter as the reference guide for femoral stem version. On CT scan, the version of lesser trochanter with respect to the posterior bicondylar axis and the femur neck was measured on the unaffected side as per the technique described by Imai et al. and Unlu et al.
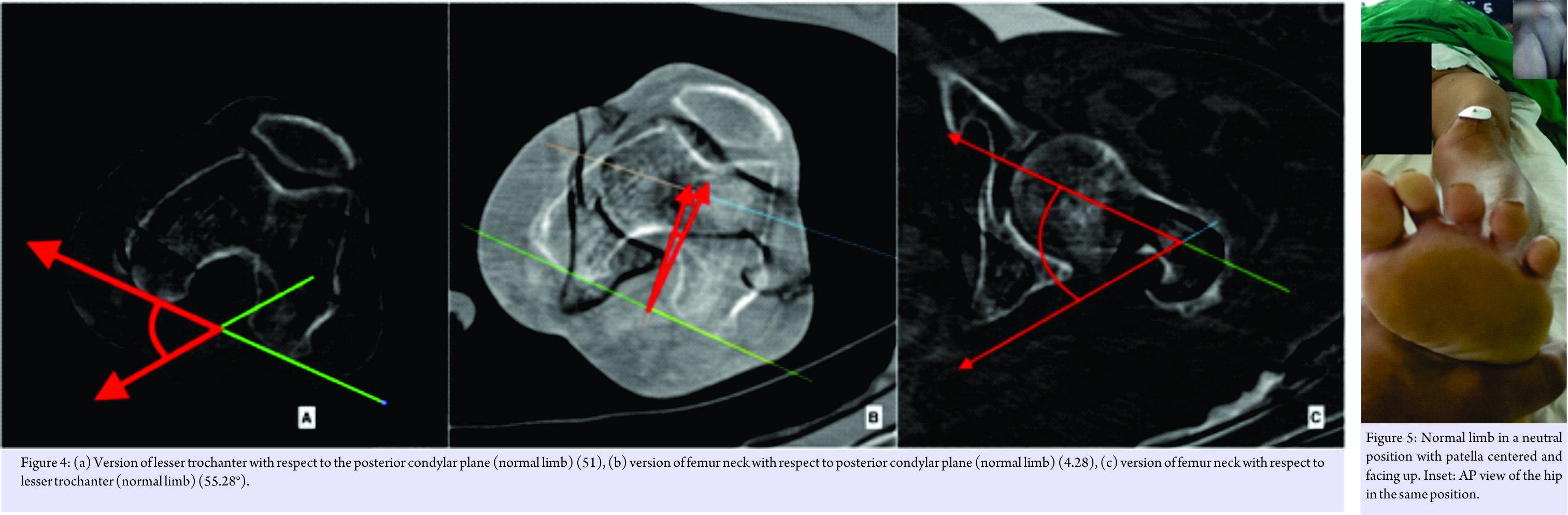
(Fig. 4) [7, 8]. Since the patient did not have any anomaly involving the proximal femur, we assumed the version of lesser trochanter would be the same as on the opposite side [9].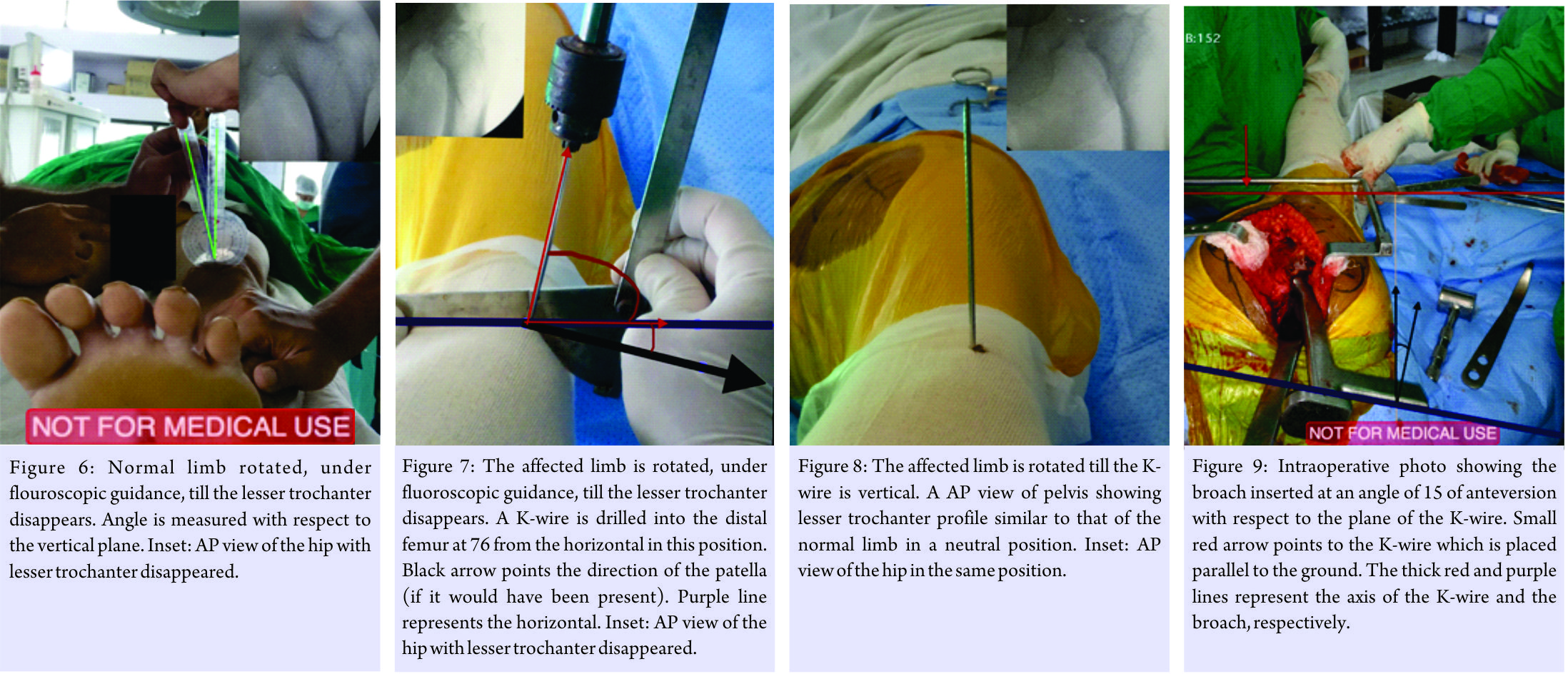
Surgical technique
A spinal + epidural analgesia was given to the patient. In the supine position, the unaffected limb was held in neutral position with patella in center and facing upward. An electrocardiography lead was stuck on the patella of the unaffected side such that the knob is facing vertical. A C-arm shoot of the pelvis was taken to identify the lesser trochanter profile (Fig. 5). Under fluoroscopic guidance, the limb was then internally rotated till the lesser trochanter disappears (Fig. 6). The angle of the patella with respect to the vertical was measured with a goniometer and found to be 14°. The patient was placed in lateral position, taking care to ensure the tangential plane passing through both the anterior superior iliac spine is perpendicular to the horizontal and the tangential plane passing through the anterior superior iliac spine and angle of acromion on the same side is parallel to the horizontal. The operative site was scrubbed, painted, and draped. A C-arm was positioned to show an anteroposterior view of the hip. The affected limb was then internally rotated, under fluoroscopic guidance, till the lesser trochanter disappears. Assuming lesser trochanter version is same as on opposite side [9], this limb now should be in 14° of internal rotation. A through and through K wire was avoided as it would interfere with the leg positioning in lateral position. Hence, a wire (2 mm K-wire) is inserted percutaneously, in the distal femur, from the lateral side at 76° from the horizontal (90°–14°= 76°) (Fig. 7). If now the limb is rotated such that the wire is vertical, this will be a neutral rotation of the limb. This can be confirmed by checking the profile of lesser trochanter and comparing it with the normal side (Fig. 8). We now have a reference for the neutral rotation of the limb. A standard posterior approach to the hip joint is made. The external rotators are cut flush to the bone. Neck cut is taken 1 cm above the lesser trochanter. The capsule is slit radially at the superolateral corner, and the head is removed. Head size was measured to be 47 mm. The posterolateral corner of the neck cut is identified, and the canal finder is inserted. The canal is reamed with 7 mm and 8 mm canal reamers. The limb is now placed in 80° flexion, 10° adduction and internally rotated such that the k wire is parallel to the horizontal (neutral rotation of the limb). A box cut is taken with 15° of anteversion from the horizontal. The canal is sequentially broached maintaining the version. A large Muller collarless stem was then cemented into place maintaining 15° of anteversion (Fig. 9). A standard 47 mm head was inserted. The hip was reduced, the limb length compared and test for stability were performed and found satisfactory. Wound was closed in layers over a drain. Method of version calculation (Fig. 10) A CT scan (from pelvis to proximal tibia bilaterally) is done postoperatively to measure the version of the stem with respect to the lesser trochanter. The version is calculated using the software Osirix lite v 8.5.2. The axial cut showing the broadest part of the lesser trochanter on the unaffected side is selected. Keeping the profile of the lesser trochanter in mind, another or same (if limb lengths are equal postoperatively) axial cut is selected, with a similar profile of lesser trochanter on the operated side. An axial cut through the femoral epicondyle is selected. Using the subtraction tool of Osirix, the images are superimposed.
A. Lesser trochanter version with respect to posterior femoral condyle on unaffected side = 51° (Fig. 10 b). B. Femoral stem version with respect to lesser trochanter = 68.95 (Fig. 10 c). C. Anteversion of femoral stem = (B-A) 68.95-51 = 17.95°. D. The measurements were repeated by the remaining authors to remove inter-observer bias.
Post-operation
During the immediate post-operative period (Fig. 10 d), the patient was clinically stable without any complication. Isometric exercises were started after 48 h, and the patient was mobilized with the help of walker on the 2nd day with a posterior knee splint. The patient was discharged on the 5th post-operative day. Suture removal was done on the 14th day. The splint was discontinued 2 months postoperatively, 6 months postoperatively, the patient is comfortable, pain-free and walking full weight bearing without any support.
Discussion
PubMed search of keywords “Knee Arthrodesis” and “Hip arthroplasty” do not yield any relevant results. As per our knowledge, there is no literature on the surgical techniques for performing hip arthroplasty in patients with ipsilateral knee arthrodesis. A well-performed knee arthrodesis has intact distal femur anatomy (medial and lateral epicondyles) for estimating the stem version; which was absent in our case. The concerns in operating this case were
1. Inability to flex the knee.
2. Inability to determine the coronal plane of femur as the distal femur anatomy was destroyed.
3. Inability to use the foot as a reference since during the index procedure the rotational alignment could have been altered.
There are chances of component malposition in such situations. This is more relevant in cemented stems where the surgeon can change the version of the stem during cementing, compared to a un-cemented stem, where the final implant fits into the canal.
The anatomical structures remaining intact in this case were (1) lesser trochanter, (2) proximal femoral cut geometry. We have described a simple technique using the lesser trochanter to determine the neutral rotation of the limb and aid the surgeon. Perumal et al. [10] in a case of bipolar hemiarthroplasty described inserting a Shantz pin in sagittal and coronal planes with the limb in neutral position; when anatomical landmarks such as patella, foot, epicondyles are absent, clinically determining the neutral position of the limb can be challenging; they have also not described the technique for determining the neutral version of the limb. We inserted a 2 mm long K-wire in the distal femur to avoid any stress riser arising in the already osteoporotic distal femur. This pins provided a simple reference for rotational orientation of the limb.
Unlu et al. [8] and Yun [11] have described using posterior lesser trochanter line as a guide for determining the femoral stem version based on a CT based anatomical study. Furthermore, inserting the stem parallel to the “T-line” can be used in such cases [2]. However, practical aspects of these references have not been studied yet.
The limitation of this technique is a slightly prolonged (10 min) post-anesthesia to pre-incision time (required to determine the neutral version of the limb) and need for inserting a K-wire in the distal femur which can act as a stress riser in an osteoporotic bone.
Conclusion
Our main aim in presenting this case was to emphasize on the surgical technique. A pre-operative CT scan should be done to evaluate the distal femur anatomy and calculate the lesser trochanter versions of the normal limb. We recommend the use of K-wire inserted into the distal femur after determining the neutral version of the limb and comparing the lesser trochanter profile with the normal side.
Clinical Message
In cases with altered distal femoral anatomy with knee arthrodesis, lesser trochanter can be used as a reference for calculation of the femoral stem version.
References
1. Masanobu Hirata, M. Y. (2013). Surgeon Error in Performing Intraoperative Estimation of Stem Anteversion in Cementless Total Hip Arthroplasty. The Journal of Arthroplasty , 28, 1648-1653.
2. Tadashi Tsukeoka, M. P. (2015). A Useful Anatomical Reference Guide for Stem Anteversion during Total Hip Arthroplasty in the Dysplastic Hip . The Journal of Arthroplasty , 30, 1393-1396.
3. Lewinnek GE, L. J. (1978). Dislocations after total hip-replacement arthroplasties. . J Bone Joint Surg [Am] 1978 , 60, 217-220.
4. D’Lima DD, U. A. (2000). The effect of the orientation of the acetabular and femoral components on the range of motion of the hip at different head-neck ratios. . J Bone Joint Surg [Am] , 82, 315-321.
5. Malik A, M. A. (2007). Impingement with total hip replacement. . J Bone Joint Surg [Am] , 89, 1832-1842.
6. Patel AB, W. R. (2010). Guidelines for implant placement to mini- mize impingement during activities of daily living after total hip arthroplasty. . J Arthro- plasty 2010;25:1275–1281. , 25, 1275-1281.
7. Norio Imai*, T. I. (2013). Do Femoral Neck and Stem Anteversion Affect Final Femur Rotation and Pelvic Positioning after Total Hip Arthroplasty? . Open Journal of Orthopedics , 3, 183-188.
8. Unlu MC, K. H. (2011). Intraoperative estimation of femoral anteversion in cementless total hip arthroplasty using the lesser trochanter. Arch Orthop Trauma Surg. , 131 (9), 1317-23
9. Young EY, G. J. (2013). Are the Left and Right Proximal Femurs Symmetric? Clinical Orthopaedics and Related Research. , 471 (5), 1593-1601.
10. Ramesh Perumal, S. R. (2017). Bipolar Hemiarthroplasty in a Patient with above-knee Amputation: Surgical Technique. Journal of Orthopaedic Case Reports , 7 (1), 54-57.
11. Ho Hyun Yun, M. i.-H. (2013). A Validation Study for Estimation of Femoral Anteversion Using the Posterior Lesser Trochanter Line . Journal of arthroplasty , 28 (20), 1776- 1780.
 |
 |
 |
 |
| Dr. Nirmal Patil | Dr. Hiren Patel | Dr. Naushad Hussain | Dr. Kalpesh Saidane |
| How to Cite This Article: Patil ND, Patel HB, Hussain N, Saidane K. Cemented Hemiarthroplasty of the Hip in a Patient with Ipsilateral Knee Arthrodesis: Surgical Difficulties and Techniques. Journal of Orthopaedic Case Reports 2018 Jan-Feb; 8(1): 75-79. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


