
[box type=”bio”] Learning Point for this Article: [/box]
To detect palmar medial fragment pre-operatively and to know the significance of the reduction of this fragment through the volar approach with capsulotomy is crucial in such cases.
Case Report | Volume 8 | Issue 1 | JOCR Jan – Feb 2018 | Page 27-31|Kemal Gökkus, Ergin Sagtas, Engin Kesgin, Ahmet Turan Aydin DOI: 10.13107/jocr.2250-0685.984
Authors: Kemal Gökkus[1], Ergin Sagtas[2], Engin Kesgin[3], Ahmet Turan Aydin[1]
[1]Department of Orthopaedics and Trauma, Memorial Antalya Hospital, Kepez, Antalya, Turkey,
[2]Department of Radiology, Memorial Antalya Hospital, Kepez, Antalya, Turkey.
[3]Antalya Tip Merkezi . Çaybasi Mah.Ali Çetinkaya Cad. No: 156 (Kiziltoprak PTT Karsisi) 07300 Muratpasa / Antalya/Turkey.
Address of Correspondence:
Dr. Kemal Gokkus,
Department of Orthopaedics and Trauma, Memorial Antalya Hospital, Zafer Mahallesi, Yildirim Beyazit Cad Number 91, Kepez/Antalya, Turkey.
E-mail: kgokkus@yahoo.com, kgokkus@gmail.com
Abstract
Introduction: Intra-articular distal radius fractures have long been massively discussed in the literature, but regarding to fractures that possess rotated volar medial fragment in the joint a few amount papers has been written. In this article, we would like to emphasize the significance of the rotated palmar medial (lunate facet) fragment.
Case Report: A 39-year-old man fell from a height of about 3 m and landed on his right outstretched hand; within 40 min, he arrived at our clinic presenting with a severe pain and swelling in his right wrist. Initial X-rays of the wrist revealed dorsal subluxation of the radiocarpal joint with dorsal comminution of the radial articular surface and fracture of the radial styloid process, with (nearly inverted) ~ 140–150° rotation of the palmar medial fragment. With an additional volar approach, the fragment reduced and stabilized with two K-wires and wrist immobilized in external fixator. The patient returned to daily activities without any discomfort and pain after the 1 year from the surgery.
Conclusion: Overlooking of palmar rotated osteochondral fragment will cause deficiency to build proper pre-operative strategy to approach the reduction of the fragment. The incompetence of reduction will deteriorate the articular surface and lead to early osteoarthritis of the wrist. The surgeon should detect this fragment and should be familiar with volar approaches of the wrist. Above average surgical experience would be needed for successful reduction.
Keywords: Comminuted distal radius fracture, Intra-articular fracture, Palmar ulnar rotated fragment, Lunate facet fragment, K-wire fixation.Introduction:
Introduction
Intra-articular fractures of the distal radius are more challenging to treat than extraarticular fractures [1]. Displaced fractures of the articular surface of the distal radius have a worse prognosis than extraarticular fractures because of potential for incongruity and arthrosis of radiocarpal and distal radioulnar joints, carpal subluxation and associated intercarpal ligament injuries [1]. Intra-articular distal radius fractures have long been massively discussed in the literature, but regarding to fractures that possess rotated palmar medial fragment a few amount paper has been written [2, 3, 4, 5, 6, 7, 8, 9, 10] (Table 1). In this article, we would like to emphasize the significance of the palmar medial rotated osteocartilaginous fragment.
Case report
A 39-year-old man fell from a height of about 3 m and landed on his right side with outstretched hand. Within 40 min, he arrived at our clinic presenting with a severe pain and swelling in his right wrist. Initial X-rays of the wrist revealed dorsal subluxation of the radiocarpal joint (Fig. 1a and b) with dorsal comminution of the radial articular surface (Fig. 1b) and fracture of the radial styloid process, with (nearly inverted) ~ 140–150° rotation of the palmar medial fragment. Computed tomography (CT) was carried out to detail the comminution and to understand the 3D configuration of the fragments (Fig. 2). The fingers were warm and capillary refill after applying pressure to distal fingertip was normal. The sensorial and motor functions of the nerves (median, ulnar, and radial nerve) were normal. No open wound was detected. The patient had no previous illness that would negatively affect emergent anesthesia. The surgery was performed that same day, only 6 h after initial admission.
Treatment
Under general anesthesia with tourniquet application, the initial closed reduction was attempted with longitudinal traction and the rotated fragment could not be reduced. For reduction of the volar rotated fragment, the modified Henry approach [11, 12, 13] was utilized. The plane between the flexor carpi radialis and radial artery was opened and the pronator quadratus muscle is incised on its radial border, exposing the distal radius. It is stripped off the distal radius together with the periosteum.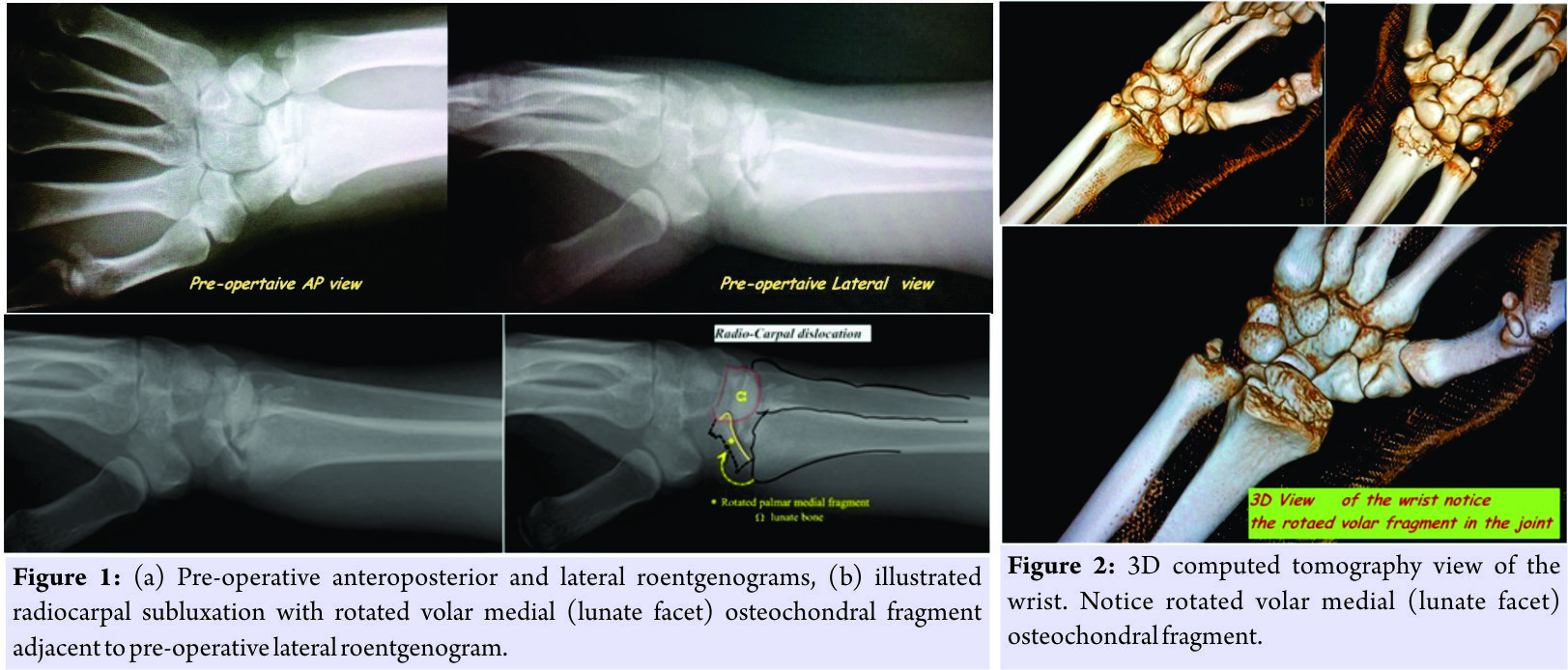 The horizontal capsulotomy parallel with the border lunate facet of the radius was carried out to approach the intra-articular rotated fragment. The radial styloid fragment was reduced with the aid of finger pressure in a dorsal-to-volar direction. The entrapped and rotated volar medial fragment was reduced by a maneuver in the opposite direction and the fragment was gripped using Kelly hemostatic forceps, gently pivoted on its own axis (with the aid of soft tissue attachments) and reduced. These reduced fragments were stabilized using two K-wires. Following this, the joint spanning external fixator was utilized to keep the reduced fragment together with initial reduction position (the wrist was positioned in palmar flexion with slide ulnar deviation). At the end of procedure, the final confirmation reduction was performed with C-arm and before discharging the patient postoperative radiography was taken (Fig. 3).
The horizontal capsulotomy parallel with the border lunate facet of the radius was carried out to approach the intra-articular rotated fragment. The radial styloid fragment was reduced with the aid of finger pressure in a dorsal-to-volar direction. The entrapped and rotated volar medial fragment was reduced by a maneuver in the opposite direction and the fragment was gripped using Kelly hemostatic forceps, gently pivoted on its own axis (with the aid of soft tissue attachments) and reduced. These reduced fragments were stabilized using two K-wires. Following this, the joint spanning external fixator was utilized to keep the reduced fragment together with initial reduction position (the wrist was positioned in palmar flexion with slide ulnar deviation). At the end of procedure, the final confirmation reduction was performed with C-arm and before discharging the patient postoperative radiography was taken (Fig. 3).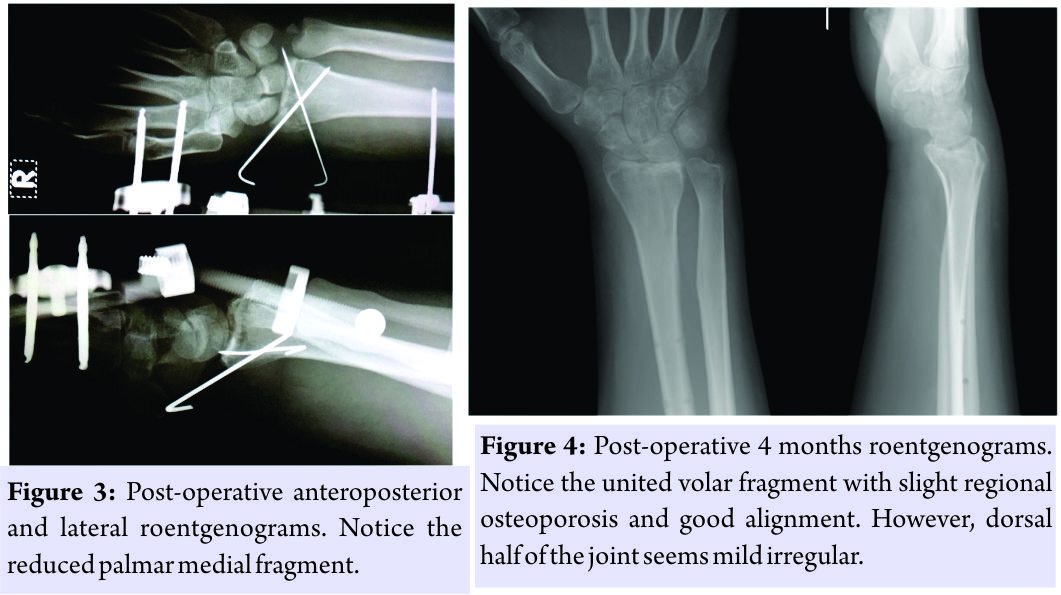
Follow-up
After 5 weeks postoperatively, the external fixator removed, physical treatment started. The post-operative 4-month X-rays revealed that the volar fragment united with good alignment. However, dorsal half of the joint healed a little irregular (Fig. 4). The patient achieved 60–70° of palmar flexion and 60–65° of dorsiflexion (Fig. 5) and returned to daily activities without any discomfort and pain after 1 year from the surgery. In last telephone call (after 18 months from the surgery), he stated that he was satisfied with clinical results.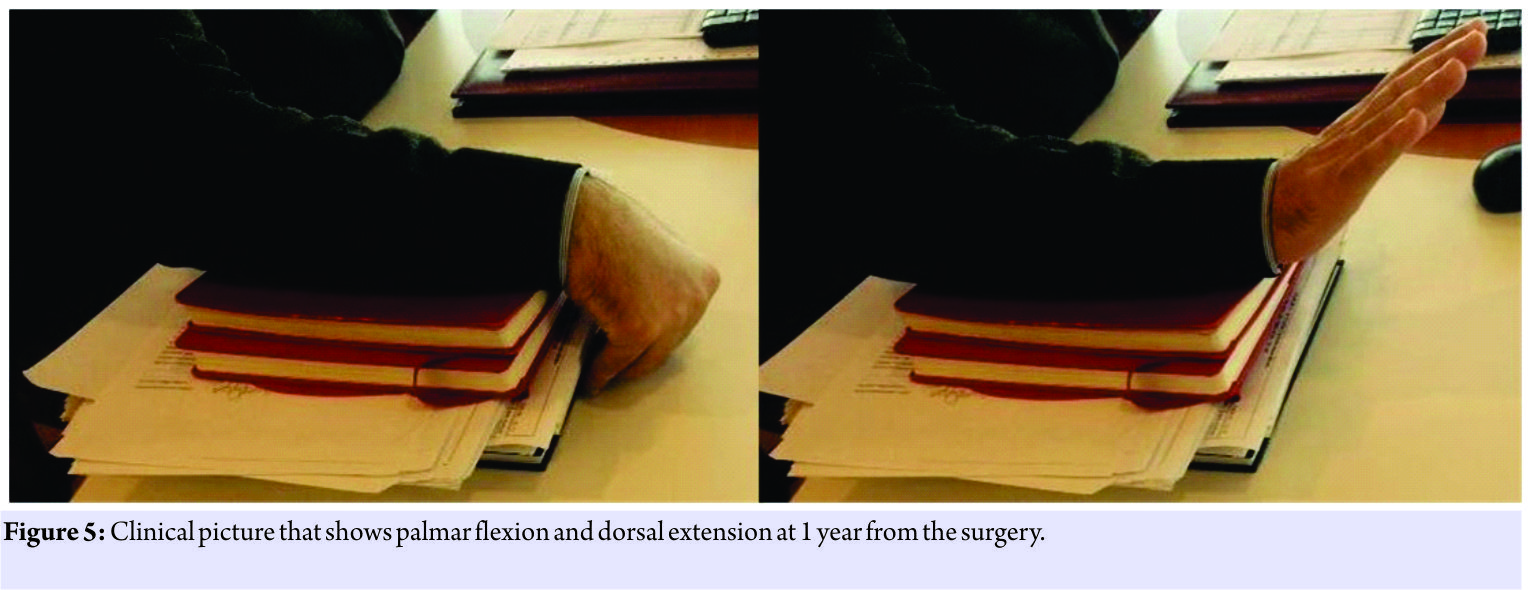
Discussion
In this article, we would like to emphasize the significance of the rotated volar medial (lunate facet) fragment. The explanation of these kinds of fractures (one large volar osteochondral fragment that rotated and entrapped in the joint with comminuted distal radius fracture) will only possible with Melone [2, 3] classification. He designated the articular fractures into four basic components: Radial shaft, radial styloid, dorsal medial fragment, and palmar medial fragment. The key medial fragments, which possess strong ligamentous attachments to both carpus and the ulnar styloid, have been designated as a medical complex, which profoundly affects both the radiocarpal and radioulnar joints are the basis on which distal radial articular fractures are classified into four categories (Type 1–4) [2, 3]. Our case could be classified as “Type IV” in Melone classification system. Melone commented in his original paper that those first three types could be treated with closed manipulation-percutaneous pin fixation. Type IV fractures necessitate the open reduction to correct the displacement of rotated medial palmar fragment rather than the other types (Type I, II, and III) [2, 3]. He reported largest cohort of this type of fracture (15 cases) with good and satisfactory results [3]. Plenty of studies had been performed regarding to assess the interobserver reliability and intraobserver reproducibility of classification systems that were interested with distal radius fractures. Given the low degree of interobserver and intraobserver agreement for each of the distal radius fracture classifications in those studies, their use as the sole means for determining the direction of treatment or for the direct comparison of results among different studies is not warranted [14, 15, 16, 17, 18, 19]. Yet among all other classification systems, Melone classification system is unique for defining rotated volar medial fragment, and it helps with decision-making for the surgical approach. Halbrecht and Stuchin [4] reported one case that possesses palmar medial fragment 180° rotation into the joint such that the articular cartilage was facing the radial shaft. They used dorsoradial approach to reduce the fragment and fixation was achieved with multiple K-wires. In this case, a non-displaced scaphoid fracture coexisted with distal radius comminuted intra-articular fracture. They immobilized the wrist with cast for 8 weeks. They emphasized the importance of CT to understand the fracture pattern and underlined necessity of the open reduction and internal fixation. Takami et al. [5] reported two cases. One of them is very similar to our case in which they used to palmar approach to reduce rotated fragment. They stabilized this reduction with multiple K-wires and immobilized wrist in cast for 4 weeks. In contrast with these cases, we secured reduction with two K-wires with external fixator for 5 weeks. In both cases, they reported, the surgery was not performed within the same day (in the first case, it was 3 weeks, and in the second case, 7 weeks after the injury). Furthermore, both cases required carpal tunnel decompression. They achieved good clinical-functional results. They emphasized the need for open reduction with palmar approach and agreed with Melone’s findings regarding the insufficiency of closed reduction. Chin and Jupiter [6] reported four cases with (Melone Type 4) displaced volar lunate facet osteochondral fractures (without any rotation). They recommend wire loop fixation to those fractures and reported good-to-excellent results. In contrast to our case, their cases had not include rotated palmar medial fragment in the joint. Panagopoulos et al. [7] reported a case very similar to us, but they reduced the rotated palmar medial fragment through the dorsoradial approach and stabilized with external fixator for 6-week immobilization. They did not detail the reduction maneuver of the fragment through the dorsoradial approach. However, their case was evidenced good healing and perfect radiological alignment with late post-operative X-rays. They emphasized the Melone deduction regarding to need for open reduction in those type fractures involving rotated palmar medial fragment. Uzel et al. [20] proposed the volar medial approach to access the medal side of the distal radius (lunate facet) and the distal radioulnar joint. They performed a mixed study that includes dissections of five cadavers with 10 wrist and four cases with Melone Type IV distal radius fractures (with rotated palmar medial fragment). They commented that the Henry approach is not adequate to access medial side of the volar distal radius unless it is extended proximally. In addition, they underlined that the median nerve might be stretched due to excessive retraction with nearby tendons. (According to their comment, to access palmar medial fragment necessitates excessive retraction of the tendon groups toward to ulnar side in Henry approach). They also proposed that detachment of the pronator quadratus from its distal attachment would be beneficial for further healing as ulnar and radial insertions are left intact. After this study Uzel et al. [8] reported four cases with the particularity of having a 90° or 180° rotated lunate fossa. They used volar medial approach between the flexors tendons and the ulnar bundle to pin the fragment of lunate fossa. They commented that using volar medial approach facilitates visualization of rotated fragment compared to the Henry’s approach and avoids the excessive traction of the median nerve. In our case, we used classic modified volar Henry approach and we were not encountered median nerve symptoms due to excessive traction of median nerve. In two cases, they used external fixator for maintaining reduction. Apergis et al. [9] and Tan and Chew [10] reported cases with fractures with volar ulnar fragment. They emphasized the importance of the ulnar palmar fragment for the stability of radiocarpal joints. In contrast of our case, in those cases, the fragments were not rotated and entrapped in the joint. These types of fractures necessitate complex strategy plan before the surgery. Because an additional intervention will be mandatory to reduce volar dislocated osseocartilaginous fragment. It would be impossible to fix this fragment with screw through the volar plate due to its’ small size. Thus, sole volar plate option for fixation would not be feasible. A sole external fixator would be also inappropriate because closed reduction could not be achieved in those fractures. The surgeon should be familiar with modified Henry approach or volar medial approach and should know the difficulty of reduction of rotated fragment. Volar medial approach is also another option and preferable depending on the surgeon’s choice as Uzel et al. proposed. This paper has a value of regarding to review of published articles in this topic, detailing the approach with discussions and highlighting the Melone classification system guidance for the management.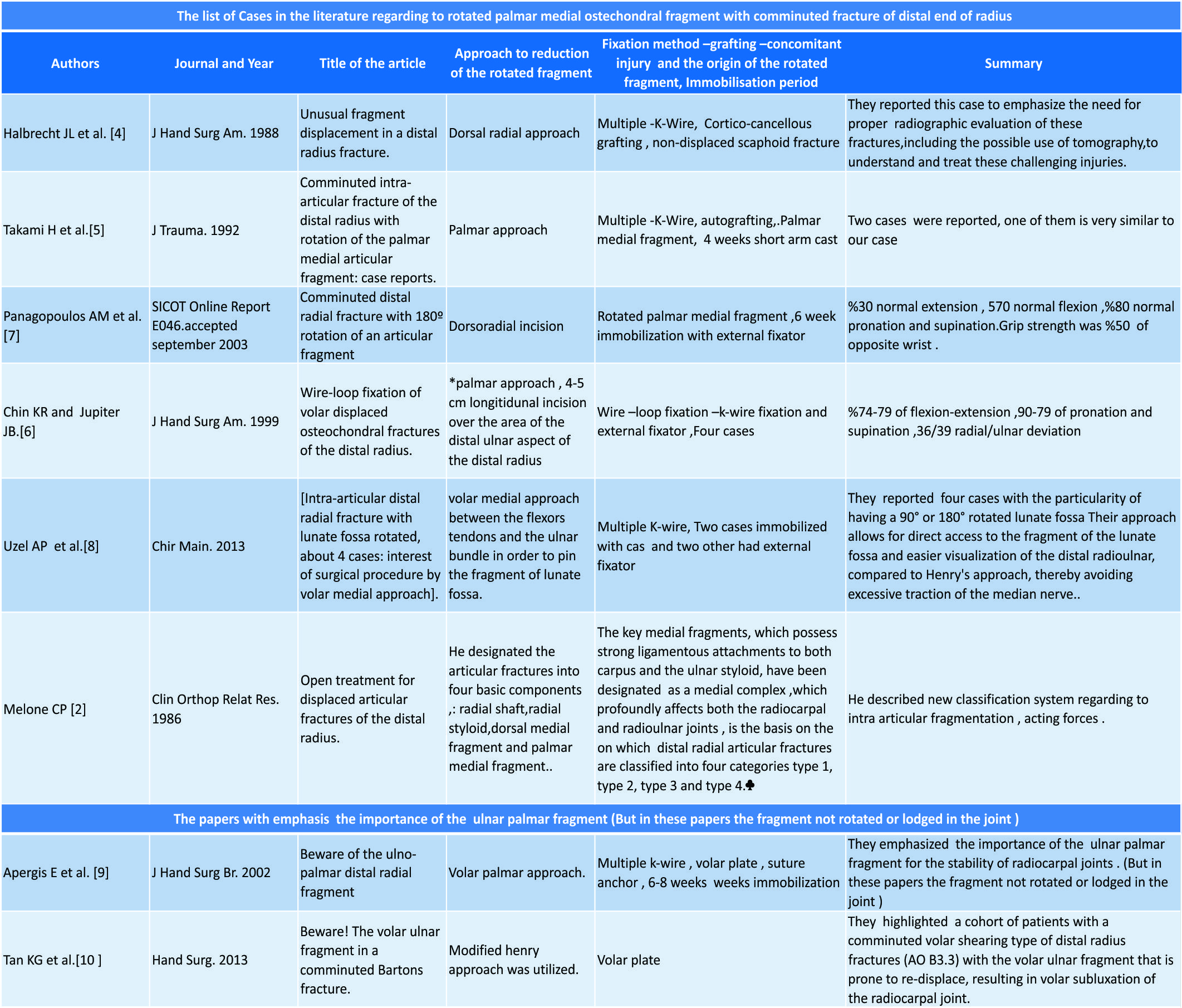
Conclusion
Literature highlighted the importance of this rare type fracture. In such cases, overlooking the possible volar rotated osteochondral fragments can cause a weakness in planning the pre-operative measures for fragment reduction. An incomplete reduction might damage the articular surface, increasing the possibility of early osteoarthritis of the wrist significantly. The reduction and fixation of these kinds of volar rotated intra-articular fragments necessitate volar extra exposure with capsulotomy in addition to classic reduction techniques (closed reduction with longitudinal traction or open reduction with classic volar approach) of the wrist fractures. The surgeon should detect this fragment clearly and should be familiar with volar approaches to the wrist. For a successful reduction, the surgeon should have the proper surgical skills and experience with such relatively complex surgeries.
Clinical Message
Comminuted distal radial fractures that possess rotated palmar medial fragment in the joint deserve more attention than the ordinary distal radius articular fractures. To detect palmar medial fragment and build a pre-operative strategy regarding to the reduction of the fragment would positively affect stability of the wrist and clinical results.
References
1. Ring D. Intra-articular fractures of the distal radius. J Am Soc Surg Hand 2002;2:60-77.
2. Melone CP Jr. Articular fractures of the distal radius. Orthop Clin North Am 1984;15:217-36.
3. Melone CP Jr. Open treatment for displaced articular fractures of the distal radius. Clin Orthop Relat Res 1986;202:103-11.
4. Halbrecht JL, Stuchin SA. Unusual fragment displacement in a distal radius fracture. J Hand Surg Am 1988;13:746-9.
5. Takami H, Takahashi S, Ando M. Comminuted intra-articular fracture of the distal radius with rotation of the palmar medial articular fragment: Case reports. J Trauma 1992;32:404-7.
6. Chin KR, Jupiter JB. Wire-loop fixation of volar displaced osteochondral fractures of the distal radius. J Hand Surg Am 1999;24:525-33.
7. Panagopoulos AM, Tyllianakis ME, Papadopoulos AX, Giannikas DA. Communited Distal Radial Fracture With 180° Rotation of an Articular Fragment. SICOT Online Report E046; 2003.
8. Uzel AP, Bulla A, Tchéro H, Tsiaviry P, Bourges C, Daculsi G, et al. Intra-articular distal radial fracture with lunate fossa rotated, about 4 cases: Interest of surgical procedure by volar medial approach. Chir Main 2013;32:37-43.
9. Apergis E, Darmanis S, Theodoratos G, Maris J. Beware of the ulno-palmar distal radial fragment. J Hand Surg Br 2002;27:139-45.
10. Tan KG, Chew WY. Beware! The volar ulnar fragment in a comminuted bartons fracture. Hand Surg 2013;18:331-6.
11. Gallagher E, Howard P, Ruiter T. Distal radius fracture in a surgeon’s dominant wrist. Eplasty 2016;16:ic35.
12. Wolfe SW. Distal radius fractures. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, editors. Green’s Operative Hand Surgery. 6th ed. Philadelphia, PA: Elsevier; 2011. p. 561-638.
13. Catalano LW 3rd, Zlotolow DA, Hitchcock PB, Shah SN, Barron OA. Surgical exposures of the radius and ulna. J Am Acad Orthop Surg 2011;19:430-8.
14. Andersen DJ, Blair WF, Steyers CM Jr. Adams BD, el-Khouri GY, Brandser EA, et al. Classification of distal radius fractures: An analysis of interobserver reliability and intraobserver reproducibility. J Hand Surg Am 1996;21:574-82.
15. Shehovych A, Salar O, Meyer C, Ford DJ. Adult distal radius fractures classification systems: Essential clinical knowledge or abstract memory testing? Ann R Coll Surg Engl 2016;98:525-31.
16. Küçük L, Kumbaracı M, Günay H, Karapınar L, Ozdemir O. Reliability and reproducibility of classifications for distal radius fractures. Acta Orthop Traumatol Turc 2013;47:153-7.
17. Belloti JC, Tamaoki MJ, Franciozi CE, Santos JB, Balbachevsky D, Chap Chap E, et al. Are distal radius fracture classifications reproducible? Intra and interobserver agreement. Sao Paulo Med J 2008;126:180-5.
18. Kural C, Sungur I, Kaya I, Ugras A, Ertürk A, Cetinus E, et al. Evaluation of the reliability of classification systems used for distal radius fractures. Orthopedics 2010;33:801.
19. Flikkilä T, Nikkola-Sihto A, Kaarela O, Pääkkö E, Raatikainen T. Poor interobserver reliability of AO classification of fractures of the distal radius. Additional computed tomography is of minor value. J Bone Joint Surg Br 1998;80:670-2.
20. Uzel AP, Bulla A, Laurent-Joye M, Caix P. Antero-medial approach to the wrist: Anatomic basis and new application in cases of fracture of the lunate facet. Folia Morphol (Warsz) 2011;70:204-10.
 |
 |
 |
 |
| Dr. Kemal Gökkus | Dr. Ergin Sagtas | Dr. Engin Kesgin | Dr. Ahmet Turan Aydin |
| How to Cite This Article: Gökkus K, Sagtas E, Kesgin E, Aydin A. T. Comminuted Distal Radial Fracture with Large Rotated Palmar Medial Osteochondral Fragment in the Joint. Journal of Orthopaedic Case Reports 2018 Jan-Feb; 8(1): 27-31. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


