
[box type=”bio”] Learning Point for this Article: [/box]
The technique for synovial osteochondromatosis of the hip joint could achieve the goals of extensive synovectomy, complete loose body removal, and avoid dislocation of the femoral head, therefore reducing the recurrence rate and surgical complications.
Case Report | Volume 8 | Issue 2 | JOCR Mar – Apr 2018 | Page 38-41| Ching-Wei Lin, Chung-Da Wu. DOI: 10.13107/jocr.2250-0685.1040
Authors: Ching-Wei Lin[1],[2], Chung-Da Wu[1]
[1]Department of Orthopedics, Chi Mei Medical Center, Tainan, Taiwan,
[2]Department of Orthopedics, Hualien Hospital, Ministry of Health and Welfare, Hualien, Taiwan.
Address of Correspondence:
Dr. Chung-Da Wu,
Department of Orthopedics, Chi Mei Medical Center, No. 901, ZhonghuRoad, Tainan City, 710, Taiwan.
E-mail: wcd225.sports@msa.hinet.net
Abstract
Introduction: Primary synovial osteochondromatosis of the hip joint is a rare condition. It is characterized by the presence of multiple intra-articular loose bodies and can result in mechanical symptoms, even causing degenerative change. Surgical treatment is indicated for synovial osteochondromatosis of the hip joint. However, the optimal approaches for successful surgical management are still controversial.
Case Report: We report two cases with primary synovial osteochondromatosis of the hip joint where arthroscopic-assisted mini-open surgical treatment was performed. The posterior approach was used, and a minimal arthrotomy was performed with preservation of bloody supplement of the femoral head. With the assistance of an arthroscope, synovectomy, debridement, and loose body removal were completed without dislocating the femoral head. The follow-up duration was 5 years and 2.5 years,respectively. There were no perioperative or post-operative complications. At the latest follow-up, the patients remain symptom free with no radiographic evidence of recurrence.
Conclusions: Our arthroscopic-assisted mini-open method could achieve the goals of extensive synovectomy, debridement, and loose body removal, thus reducing the recurrence rate. This method avoids dislocation of the femoral head, thus reducing the occurrence of surgical complications.
Keywords: Synovial osteochondromatosis, hip joint, arthrotomy, arthroscopy.
Introduction
Primary synovial osteochondromatosis is a rare benign disorder of the synovium, and metaplastic transformation leads to the formation of osteochondral bodies in the joint cavity. The diseased synovia and the intra-articular loose bodies may progressively cause joint articular cartilage damage over years before the disease is diagnosed. Treatment of this condition is essentially adequate debridement, removal of loose bodies, and near total synovectomy. The knee is the most commonly affected joint, and involvement of the hip joint is relatively rare [1].Knee joint synovial osteochondromatosis can be adequately treated with arthroscopic surgery. However, surgical management of hip joint synovial osteochondromatosis is much more difficult due to its specific anatomy. Open arthrotomy with femoral head dislocation to expose the whole hip joint or an arthroscopic approach to the hip joint and perform surgery has been reported. However, the optimal approach for successfully managing this condition is still controversial. The risk of avascular necrosis caused by femoral head dislocation during the surgery always exists. Inadequate debridement and a relatively high recurrence rate are the main concerns of hip arthroscopy [2, 3, 4, 5]. The posterior approach with preservation of the deep branch of the medial femoral circumferential artery, limited arthrotomy without dislocation of the femoral head, use of an arthroscope to carry out the synovectomy, and loose body removal is our method of treatment for this particular condition. We report two cases of primary synovial osteochondromatosis of the hip joint with a description of their disease courses, radiographic presentations, surgical management, and follow-up results.
Case Report
Case I
A 41-year-old male without any previous trauma history had suffered from disabling right hip pain for more than 3 years. Before visiting our institution, he had conservative treatments including analgesics and rehabilitation under the impression of muscle strain; however, the pain got worse. Physical examination of the right hip joint showed limited internal–external rotation, abduction, and adduction. Intra-articular calcified loose bodies filling the hip joint were seen on plain radiographs (Fig. 1). Magnetic resonance imaging revealed the expansion of the joint capsule containing multiple loose bodies around the femoral neck (Fig. 2). Synovectomy and loose body removal were done through limited hip joint arthrotomy and with the assistance of an arthroscope (Fig. 3).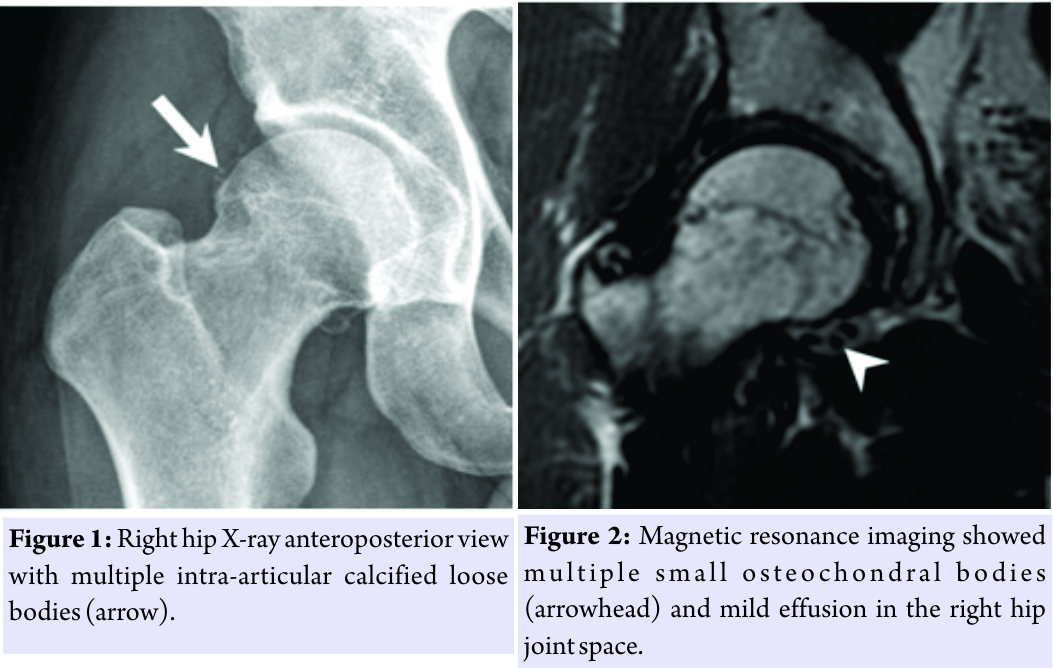 Histologic study revealed characteristic findings of Milgram Stage II synovial osteochondromatosis. The patient has been followed up for 5 years. Subjectively, he has no complaint and full motion of the operated hip joint. Harris hip score improved from pre-operative 60–94 points at the time of the latest follow-up. He plays volleyball and softball regularly without any problem. The latest follow-up X-rays showed clear a right hip joint without evidence of osteoarthritis or avascular necrosis of the femoral head (Fig. 4).
Histologic study revealed characteristic findings of Milgram Stage II synovial osteochondromatosis. The patient has been followed up for 5 years. Subjectively, he has no complaint and full motion of the operated hip joint. Harris hip score improved from pre-operative 60–94 points at the time of the latest follow-up. He plays volleyball and softball regularly without any problem. The latest follow-up X-rays showed clear a right hip joint without evidence of osteoarthritis or avascular necrosis of the femoral head (Fig. 4).
Case II
A 32-year-old professional baseball pitcher without any previous trauma history had suffered from left hip joint pain for more than 3 years. The pain was severe on rotation of the joint, and his performance was greatly reduced. Physical examination could only detect some weakness of the gluteal muscles. The plain radiograph appeared normal (Fig. 5). However, multiple loose bodies were found below the femoral head in the left hip joint by magnetic resonance imaging studies (Fig. 6). The patient received operation of the left hip joint. Milgram Stage II synovial osteochondromatosis was confirmed by pathologic examination. He resumed pitching 10 months after the operation and is back to his pre-injury level of professional pitching. It has been 2.5 years after his hip joint operation. Subjectively, his hip joint feels normal. Harris hip score was 44 points pre-operatively and has improved to 98 points at the latest follow-up. His latest follow-up X-ray did not have any evidence of degeneration or femoral head avascular necrosis (Fig. 7).
However, multiple loose bodies were found below the femoral head in the left hip joint by magnetic resonance imaging studies (Fig. 6). The patient received operation of the left hip joint. Milgram Stage II synovial osteochondromatosis was confirmed by pathologic examination. He resumed pitching 10 months after the operation and is back to his pre-injury level of professional pitching. It has been 2.5 years after his hip joint operation. Subjectively, his hip joint feels normal. Harris hip score was 44 points pre-operatively and has improved to 98 points at the latest follow-up. His latest follow-up X-ray did not have any evidence of degeneration or femoral head avascular necrosis (Fig. 7).
Operative technique
The patient was put in the lateral decubitus position. A Kocher-Langenbeck incision was made. The quadratus femoris tendon was first identified and protected, then the gemelli, obturator internus, and piriformis tendons were divided about 2cm from their bony insertion sites to gain access to the hip joint capsule [6].The joint capsule was opened using a small T-shaped incision. All accessible loose bodies and proliferative synovium were first removed under direct vision.Manual traction was applied,and an arthroscope was first inserted through the superior aperture into the hip joint; inflow fluid was established parallel to the scope sheath. Arthroscopic shaver with suction drainage and a grasper were put into the inferior, dependent position of the hip joint. Small loose bodies were suctioned out, and the remaining larger loose bodies were taken out by an arthroscopic grasper. A synovectomy was done as completely as possible using an arthroscopic shaver. Special care was taken not to damage the ligamentum teres, though the most difficult loose bodies to be removed were found near it or attached to it. After the work on the inferior hip joint was finished, the scope and the instruments’ position were switched to clean the remaining portions of the hip joint. The joint capsule was closed with 1–0 Vicryl. A drain was inserted and the external rotators were then repaired with interrupted 1-0 Vicryl sutures.
Discussion
As there is no specific symptom and signs and due to its rarity, the diagnosis of hip joint synovial osteochondromatosis is often missed or delayed. Plain radiographs are the initial study tool. However, loose bodies cannot be seen on plain radiograph unless there is calcification or ossification. Magnetic resonance imaging is the most useful diagnostic tool for this disease [7, 8]. The benefit of magnetic resonance imaging is to provide early diagnosis of the disease and to evaluate extra-articular involvements. Synovectomy and loosebody removal are the recommended method of treatment. Most authors in the literature support the idea of adequate synovectomy to decrease the disease recurrence rate. Several methods are available to achieve this goal. Arthroscopic synovectomy of the hip joint is technically demanding,and it has difficulty reaching some areas with extensive synovectomy usually beingimpossible. The recurrence rate after arthroscopic surgery is high, ranging from 7.1% to 39 % [2, 3, 4, 5]. In Boyer and Dorfmann’s report, 23of the 111 patients(20.7%)required more than one arthroscopy; 42 of them(37.8%)required open surgery. If the disease was managed by arthroscopy alone, 18 (16.2%) of the 69 patients required further arthroscopies [2]. Five patients received revision arthroscopy in Marchie et al.’s series [3].Hip arthroscopy is considered most useful when the loose bodies are <10 mm [3]. Open surgery with or without femoral head dislocation is another treatment method [7, 9, 10, 11, 12]. If the femoral head is not dislocated, complete synovectomy and loose body removal could not be easily done or are almost an impossible task. If the femoral head is dislocated, there is always fear of complications such asavascular necrosis of the femoral head, osteoarthritis, trochanteric fixation failure, or ectopic ossification [11,13].In Lim et al.’s series, two symptomatic disease recurrences occurred in thirteen hips treated with arthrotomy alone. No recurrence was noted in 21 of the patients treated with femoral head dislocation, but the surgical complication rate was significantly higher in this group of patients [7]. Ganzet al. developed a surgical technique to achieve dislocation of the femoral head without the risk of avascular necrosis [13]. The deep branch of the medial femoral circumferential artery in front of the quadratus femoris tendon, the primary source for blood supply of the femoral head, is protected and the most worrisome iatrogenic complication of posterior arthrotomy, post-operative avascular necrosis of the femoral head, could be prevented [6]. In eight patients with this disease treated with this surgical method, no recurrence or avascular necrosis was found at follow-up [9]. We wanted to achieve our goal of extensive synovectomy, complete loose body removal, and prevention of disease recurrence. On the other hand, we protected the deep branch of the medial femoral circumferential artery and avoided to sacrifice the ligamentum teres. The nerve ending of this ligament has proprioception functions similar to the cruciate ligaments of the knee joint [14], by preserving the ligament, better functional recovery could be achieved. Thus, it was our final surgical design that we could try to perform the surgery with mini-arthrotomy and use the arthroscope to clean the hip joint. The follow-up results proved our arthroscopic-assisted mini-open surgery of hip joint synovial osteochondromatosis to be a feasible and effective method.
Conclusion
Surgical treatment is indicated for synovial osteochondromatosis of the hip joint. Our arthroscopic-assisted mini-open debridement technique did achieve the goals of extensive synovectomy and complete loose body removal. We also preserved the ligament teres for better functional recovery. The follow-up results were very encouraging. This is, therefore, a viable alternative for orthopedic surgeons to treat this rarely encountered disease.
Clinical Message
The arthroscopic-assisted mini-open technique for synovial osteochondromatosis of the hip joint could achieve the goals of extensive synovectomy and complete loose body removal, thus reducing the recurrence rate. This method could avoid dislocation of the femoral head, therefore reducing the occurrence of surgical complications.
References
1. Milgram JW. Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801. Available from:https://www.jbjs.org/reader.php?source=The_Journal_of_Bone_and_Joint_Surgery/59/6/792/abstract&id=13946&rsuite_id=399380#info
2. Boyer T, Dorfmann H. Arthroscopy in primary synovial chondromatosis of the hip: Description and outcome of treatment. J Bone Joint Surg Br 2008;90B:314-8. Available from: https://www.ncbi.nlm.nih.gov/ pubmed/18310752
3. Marchie A, Panuncialman I, McCarthy JC. Efficacy of hip arthroscopy in the management of synovial chondromatosis. Am J Sports Med 2011;39 Suppl:126S-31S. Available from: https://www.ncbi.nlm.nih.gov/pubmed/21709042
4. Lee JB, Kang C, Lee CH, Kim PS, Hwang DS. Arthroscopic treatment of synovial chondromatosis of the hip. Am J Sports Med 2012;40:1412-8. Available from: https://www.ncbi.nlm.nih.gov/pubmed/22539535
5. deSa D, Horner NS, MacDonald A, Simunovic N, Ghert MA, Philippon MJ, et al. Arthroscopic surgery for synovial chondromatosis of the hip: A systematic review of rates and predisposing factors for recurrence. Arthroscopy 2014;30:1499-50400. Available from: https://www.ncbi.nlm.nih.gov/pubmed/25064754
6. Gautier E, Ganz K, Krugel N, Gill T, Ganz R. Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br 2000;82:679-83. Available from: http://www.bjj.boneandjoint.org.uk/ content/82-B/5/679.
7. Lim SJ, Chung HW, Choi YL, Moon YW, Seo JG, Park YS. Operative treatment of primary synovial osteochondromatosis of the hip. J Bone Joint Surg Am 2006;88:2456-64. Available from:https://www.ncbi.nlm.nih.gov/pubmed/17079404
8. McKenzie G, Raby N, Ritchie D. A pictorial review of primary synovial osteochondromatosis. Eur Radiol 2008;18:2662-9. Available from: https://www.ncbi.nlm.nih.gov/ pubmed/18491106
9. Schoeniger R, Naudie DD, Siebenrock KA, Trousdale RT, Ganz R. Modified complete synovectomy prevents recurrence in synovial chondromatosis of the hip. Clin Orthop Relat Res 2006;451:195-200. Available from: https://www.ncbi.nlm.nih.gov/pubmed/16760824
10. Nakamura Y, Echigoya N, Toh S. Synovial osteochondromatosis of the hip treated through a surgical dislocation. J Arthrop 2009;24:1143, e15-9. Available from: https://www.ncbi.nlm.nih.gov/ pubmed/18835688
11. Zhang YM, Liu X. Surgery of a rare case of multiple synovial osteochondromatosis of the hip joint. J Orthop Case Rep 2016;6:51-4.
12. Kataoka M, Goto K, Kuroda Y, Kawai T, Murata O, Sugimoto M, et al. Complete resection of a massive synovial osteochondromatosis of the hip using an anterior approach: A Report of two cases. Case Rep Orthop 2017;2017:9806863.
13. Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip: A technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-24. Available from: http://bjj.boneandjoint.org.uk/ content/83-B/8/1119.
14. Leunig M, Beck M, Stauffer E, Hertel R, Ganz R. Free nerve endings in the ligamentum capitis femoris. Acta Orthop Scand 2000;71:452-4. Available from: http://www.tandfonline.com/doi/abs/10.1080/000164700317381117.
 |
 |
| Dr. Ching-Wei Lin | Dr. Chung-Da Wu |
| How to Cite This Article: Lin C W, Wu C D.Primary Synovial Osteochondromatosis of the Hip Joint Treated with Arthroscopic-assisted Mini-open Surgery-Two Case Reports. Journal of Orthopaedic Case Reports 2018. Mar- April; 8(2): 38-41. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


