
[box type=”bio”] Learning Point for this Article: [/box]
Varus deformity of the second toe of hallux valgus foot may be secondary to the metatarsus primus varus deformity.
Case Report | Volume 8 | Issue 2 | JOCR Mar – Apr 2018 | Page 42-46| Wu Daniel. DOI: 10.13107/jocr.2250-0685.1042
Authors: Wu Daniel[1]
[1]Department of Orthopaedics, Fellow of Hong Kong College of Orthopaedic Surgeons, Hong Kong, China.
Address of Correspondence:
Dr. Daniel Wu,
Hong Kong Adventist Hospital, 40 Stubbs Rd., Hong Kong, China.
E-mail: info@bunioncenter.com
Abstract
Introduction: Crossover deformity of the first and second toes is not uncommon of a severe hallux valgus (HV) deformity. It can be corrected by adequate realignment of the hallux. However, the crossover deformity may be complicated by also aconcomitant varus deformity of the second toe. Although the pathoanatomy of second toe varus deformity has been well described, its pathogenesis is still unclear. Consequently, its treatment has been mostly symptomatic and not specific to its pathogenesis. This is a 1-year follow-up report of spontaneous correction of the second toe varus deformity after a soft tissue procedure for HV and metatarsus primus varus (MPV) deformities correction.
Case Report: A patient had bilateral HV and crossover deformities of her feet. She opted fora bilateral surgical treatment when conservation management failed to be helpful anymore. A soft tissue non-osteotomy technique called syndesmosis procedure was chosen for her deformities correction. Her crossover deformity was caused mainly by varus deformity of the second toe. Intraoperatively, the second toe varus deformity was found to correct itself spontaneously once the first metatarsal was realigned by a non-osteotomy intermetatarsal cerclage suture technique to correct the MPV deformity. Only the more severe second toe deformity of right foot required additional soft tissue release to help correct its mild residual varus deformity.The patient enjoyed excellent cosmetic and functional results. The possible pathogenesis of second toe varus deformity and its unexpected spontaneous correction is discussed.
Conclusion: The pathogenic deforming force of second toe varus deformity may originate from the first ray HV deformity complex. Consequently,the satisfactory anatomical correction of her HV deformity and also function restoration of the first ray by the syndesmosis procedure might have beenthe mechanismof spontaneouscorrection of thesecond toe varus deformity and its recurrence prevention.
Keywords: Hallux valgus deformity, metatarsus primus varus deformity, second toe varus deformity, syndesmosis procedure.
Introduction
Hallux valgus (HV) deformity is practically a deformity complex of the first ray that is made up of HV, and also bunion,metatarsus primus varus (MPV), and sesamoid displacement [1, 2]. HV deformity is a progressive condition under the stress of daily weight-bearing activities and shoes in general.Secondary problems such as claw deformity of the lesser toes, metatarsal callus, metatarsalgia, and crossover deformity of the first and second toe scan develop in time [3]. The crossover deformity is usually formed by a severeval gusdeviation of the hallux, while the second toe remains mostly straight [4, 5]. This simple form of crossover deformity can be readily corrected through adequate realignment of the hallux. However, the crossover deformity can also comprise varus deformity of the second toe, and then, straightening of the hallux alone would not be sufficient without realigning the second toe also.The management of such complicated crossover deformity is still regarded one of the most challenging conditions of lesser toes [6]. This is because its pathogenesis is not well understood yet and its surgical treatment has been limited to correction of secondary anatomical changes of the plantar plate [7] and collateral ligaments. Tendon transfer may be recommended to correct more severe varus deformity,but stiffness can become an issue [8, 9]. This case report is about a bilateral moderate HV deformity with crossover toes that were mostly contributed by varus deformity of the second toes. The purpose of this presentation was to report the unexpected spontaneous realignment of second toes and its metatarsophalangeal joint (MPJ) once the underlying severe MPV deformities were corrected intraoperatively with a non-osteotomy intermetatarsal cerclage-suture technique. This spontaneous correction effect has not been reported after osteotomy or other HV surgical techniques in the past.
Case Report
A 60-year-old female had progressive HV and bunion deformities for many years. Despite increasing pain in the bunion area initially and then the crossover deformity between first and second toes,she could still manage for several years by wearing increasingly more accommodating shoes with wider forefoot region and roomy toe box made of soft materials. Due to her daily required walking activities, she developed thick and painful metatarsal calluses despite wearing mostly thick-soled shoes only. She could hardly tolerate the metatarsalgia of her feet in walking due to the constant feeling of walking on a pebble in her shoes. She found that walking was becoming an exhausting chore to avoid. She felt losing balance easily on uneven ground and walking down stairs.She had fallen several times already. Her mother had also HV deformity but not as severe and she got by without surgery. Physical examination revealed bilateral HV deformity (Fig. 1) that could only be partially corrected.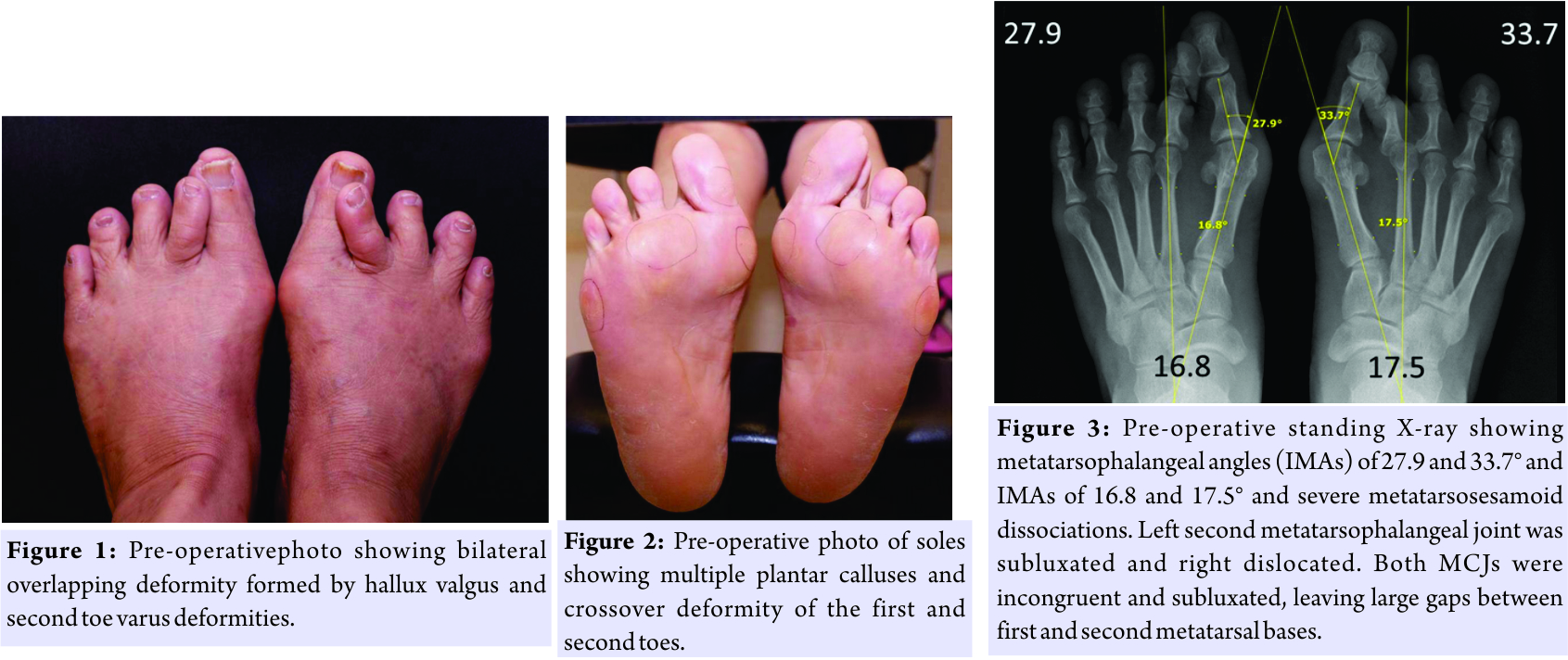 The passive range of motion of her right foot first MPJ was 45° in both extension and flexion and 60° and 45°,respectively,of her left foot first MPJ. Her right second toe had severe varus deformity that was crossing over the hallux but without any remarkable clawing deformity. Her left second toe varus deformity was not as severe. The second toe varus deformity of her left foot could be manually realigned completely but not her right foot second toe. Both second MPJs were moderately tender and had reduced passive flexion movement due to pain. First metatarsals were hypermobile in both sagittal and frontal planes.There were large and thick calluses under the forefoot region of both feet (Fig. 2). Dorsoplantar standing x-rays of her feet (Fig. 3) revealed a right foot first intermetatarsal angle (IMA) of 17.5° and metatarsophalangeal angle (MPA) of 33.7° and 16.8° and 27.9°,respectively,of her left foot. IMA and MPA are usually considered normal within their upper limits of 9° and 15°, respectively. All first and second MPJs were in congruent and the right second MPJ subluxated in dorsomedial direction. Both tibial and fibula sesamoids were dissociated from their first metatarsals. Pre-operative walking plantar pressure study by F-Scan (Tekscan, USA) (Fig.4) revealed poor weight bearing and reactive force under the first ray and obvious lateral shift of functional area of her forefeet to the second and third metatarsal heads where she had large and thick metatarsal calluses. This patient agreed to undergo a simultaneous bilateral syndesmosis procedure [10, 11], a non-osteotomy soft tissue technique, for her HV deformity correction and possible additional surgery and pinning if necessary for the varus deformity correction of her second toes.
The passive range of motion of her right foot first MPJ was 45° in both extension and flexion and 60° and 45°,respectively,of her left foot first MPJ. Her right second toe had severe varus deformity that was crossing over the hallux but without any remarkable clawing deformity. Her left second toe varus deformity was not as severe. The second toe varus deformity of her left foot could be manually realigned completely but not her right foot second toe. Both second MPJs were moderately tender and had reduced passive flexion movement due to pain. First metatarsals were hypermobile in both sagittal and frontal planes.There were large and thick calluses under the forefoot region of both feet (Fig. 2). Dorsoplantar standing x-rays of her feet (Fig. 3) revealed a right foot first intermetatarsal angle (IMA) of 17.5° and metatarsophalangeal angle (MPA) of 33.7° and 16.8° and 27.9°,respectively,of her left foot. IMA and MPA are usually considered normal within their upper limits of 9° and 15°, respectively. All first and second MPJs were in congruent and the right second MPJ subluxated in dorsomedial direction. Both tibial and fibula sesamoids were dissociated from their first metatarsals. Pre-operative walking plantar pressure study by F-Scan (Tekscan, USA) (Fig.4) revealed poor weight bearing and reactive force under the first ray and obvious lateral shift of functional area of her forefeet to the second and third metatarsal heads where she had large and thick metatarsal calluses. This patient agreed to undergo a simultaneous bilateral syndesmosis procedure [10, 11], a non-osteotomy soft tissue technique, for her HV deformity correction and possible additional surgery and pinning if necessary for the varus deformity correction of her second toes.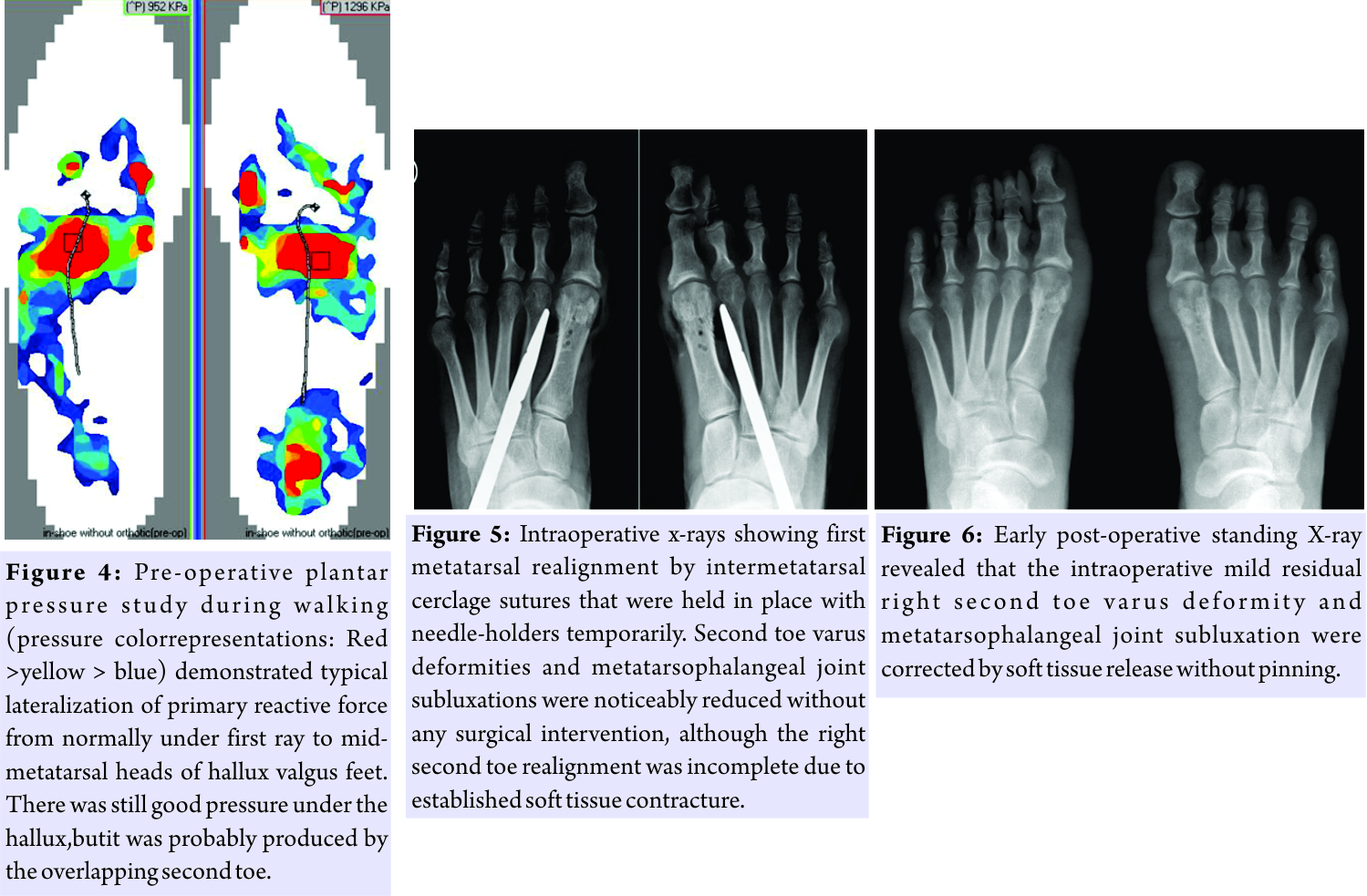
Operative technique
An initial one-inch incision was made along the distal dorsal medial border of the second metatarsal. After blunt dissection, the interosseous muscle was retracted laterally and partially resected to help expose the lateral soft tissue structures for the release of the lateral collateral and metatarsosesamoid ligaments. The adductor hallucis tendon was preserved and the fibular sesamoid was not resected. The distal third of the first and second metatarsals was then exposed subperiosteally and roughened in a fish-scale fashion with an osteotome. Three drill holes of 2 mm diameter were made in dorsoplantar direction in the distal half of first metatarsal shaft about 5 mm apart. Double-strand number-onepolydioxanone dissolvable sutures (ETHICON, Johnson & Johnson, USA) were then passed through the drill holes and around the second metatarsal, binding the two together. Intraoperative anteroposterior (AP) view X-ray was then taken to assess the MPV deformity correction and first metatarsal alignment with a needle holder temporarily locking the intermetatarsal cerclage suture (Fig. 5) before it was tied later. However, to our surprise that,not only the HV and MPV deformities were corrected but also the severe right second toe varus deformity was also mostly corrected spontaneously without any surgical intervention to it yet. The same phenomenon also was happened to her left second toe but with complete spontaneous correction.The residual varus deformity of right foot second toe was then further corrected by capsulorrhaphy and collateral ligaments release of its MPJ. A medial horizontal elliptical incision was then made to remove redundant skin, bursa, capsular tissues, and exostoses. The combined single ligament tendon capsular layer was then approximated with interrupted 2-0 Vicryl sutures (Ethicon, Johnson & Johnson, USA) without plication.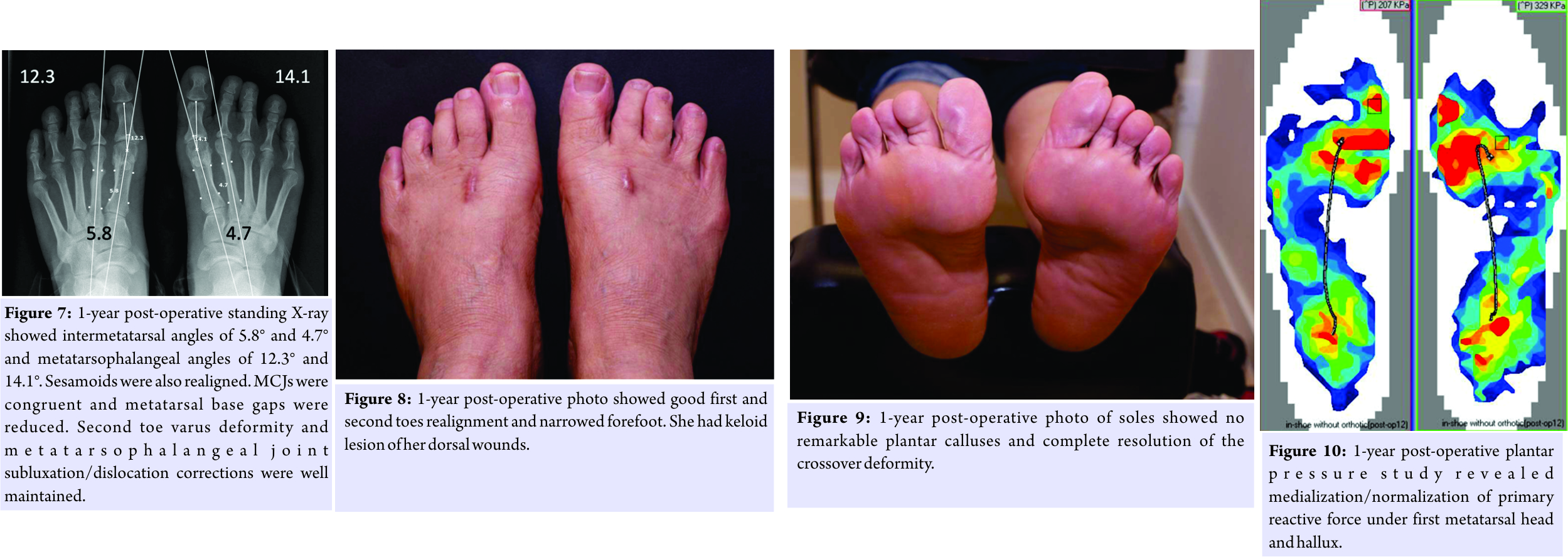
Post-operative care
The patient worea forefoot cast for protected walking for 3 months. She was allowed only to return to unrestricted activities and shoes about 6 months after surgery.
Result
Her early post-operative standing AP view x-ray revealed excellent MPV, HV, sesamoid dissociation, and second toe varus deformity correction without using pin fixation (Fig. 6). Her 1-year standing X-ray revealed excellent maintenance of all corrections without signs of impending recurrences. The right and left IMA and MPA were 4.7° and 14.1° and 5.8° and 12.3°, respectively (Fig. 7). The patient was extremely satisfied with her cosmetic result (Fig. 8) and also being able to return to regular shoes without any pre-operative pain. She had no more episodes of losing balance in walking or falling. Her plantar call uses have mostly disappeared (Fig. 9), and she had no more metatarsalgia. Both first metatarsals were much more stable and less mobile in all planes than before.She felt her feet much firmer and less effort and tiring in walking. She did not participate in any sports or exercises by choice. She could wear heels about two-inch high comfortably and no desire for anything higher. Function study of the plantar pressure distribution of her feet again by F-scan revealed medialization of forefoot function area under the first ray in walking (Fig. 10).
Discussion
First ray, medial column of the foot, is the most important mechanical region of the forefoot for exerting the necessary force to push body forward in walking. HV is a progressive condition,and as its hallux, first metatarsal, and sesamoids move increasing out of their normal positions due to the stress of daily activities [1], the mechanical function of the first ray for walking can become also increasingly compromised. Consequently, lesser toes need to compensate for the loss in hallux function, and they can be overworked and develop secondary problems such as clawing deformity and MPJ dorsal dislocation, metatarsal plantar calluses, and metatarsalgia [2]. The pathogenesis of most of these secondary conditions has been well described, but not of the second toe varus deformity despite its pathoanatomy of lateral attenuation of MPJ collateral ligament and plantar plate and medial soft tissues contracture [12,13]are well recognized already. Without knowing the exact underlying cause of the second toe varus deformity, its definitive correction and recurrence prevention are still not satisfactorily resolved yet.Although flexor-to-extensor tendon transfer has been recommended, stiffness has often been a problem [14]. Since, according to this patient, her crossover deformity developed only subsequent to her HV deformity, it is then reasonable to surmise that it could be secondary to her HV deformity. It might have certain deforming effect on the second toe statically and dynamically. Its intraoperative spontaneous correction after MPV correction by a non-osteotomy technique strongly suggested that there was probably a static causal effect relationship between the varus deformity of first metatarsal and second toe, but more study is needed to understand this possible anatomical connection. There would also likely be a dynamic causal effect due to the loss of hallux function of HV deformity and consequential over use deforming effect on the second toe. This dynamic relationship can also probably be drawn from the function restoration of hallux [10] as demonstrated by her plantar pressure study and the absence of second toe varus deformity recurrence without the usual Weil osteotomy of the second metatarsal [15]. This possible deforming force was likely related to the dysfunction of the all-important first ray of the foot due to its HV, MPV, and sesamoids dissociation. Since these deformities were satisfactorily corrected by evidence of her X-rays and the function of first ray was restored by evidence of her F-Scan studies, they are possible circumstantial reasons for the deforming force being removed from the second toe [10] and to have prevented recurrence of the varus deformity despite her return to unrestricted activities after surgery.
Conclusion
This case presentation demonstrated that MPV and HV deformities could be the underlying cause of the varus deformity of the second toe,statically and dynamically. This probably was the reason for its spontaneous resolution and also its recurrence prevented after the proper anatomical correction and function restoration of first ray.
Clinical Message
Within a deformity complex, there may just be one principal deformity/pathology and it may be responsible for other accompanied problems. These secondary problems may be resolved spontaneously if their underlying primary cause can be effectively removed.
References
1. Haines RW, McDougall A. The anatomy of hallux valgus. J Bone Joint Surg Br 1954;36-B:272-93.
2. Coughlin MJ. Lesser toe deformities. In: Coughlin MJ, Anderson RB, editors. Mann’s Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier; 2014. p. 322-424.
3. Shirzad K, Kiesau CD, DeOrio JK, Parekh SG. Lesser toe deformities. J Am Acad Orthop Surg 2011;1:9505-14.
4. Coughlin MJ. Subluxation and dislocation of the second metatarsophalangeal joint. Orthop Clin North Am 1989;20:535-51.
5. Bhatia D, Myerson MS, Curtis MJ, Cunningham BW, Jinnah RH. Anatomical restraints to dislocation of the second metatarsophalangeal joint and assessment of a repair technique. J Bone Joint Surg [Am] 1994;76-A:1371-5.
6. Malhotra K, Davda K, Singh D. The pathology and management of lesser toe deformities. EFORT Open Rev 2017;1:409-19.
7. Stainsby GD. Pathological anatomy and dynamic effect of the displaced plantar plate and the importance of the integrity of the plantar plate-deep transverse metatarsal ligament tie-bar. Ann R Coll Surg Engl 1997;79:58-68.
8. Veljkovic A, Lansang E, Lau J. Forefoot tendon transfers. Foot Ankle Clin 2014;19:123-37.
9. Barca F, Acciaro AL. Surgical correction of crossover deformity of the second toe: A technique for tenodesis. Foot Ankle Int 2004;25:620-4.
10. Leung AK, Man HS, Wong DW, Wu DY. Syndesmosis procedure for the treatment of hallux valgus. Good clinical and radiological results two years post-operatively. Bone Joint J 2014;96-B:502-7.
11. Wu DY, Lam KF. Osteodesis for hallux valgus correction: Is it effective? Clin Orthop Relat Res 2015;473:328-36.
12. Coughlin MJ. Subluxation and dislocation of the second metatarsophalangeal joint. Orthop Clin North Am 1989;20:535-51.
13. Deland JT, Sung IH. The medial crossover toe: A cadaveric dissection. Foot Ankle Int 2000;21:375-8.
14. Haddad SL, Sabbagh RC, Resch S, Myerson B, Myerson MS. Results of flexor-to-extensor and extensor brevis tendon transfer for correction of the crossover second toe deformity. Foot Ankle Int 1999;20:781-8.
15. Vandeputte G, Dereymaeker G, Steenwerckx A, Peeraer L. The Weil osteotomy of the lesser metatarsals: A clinical and pedobarographic follow-up study. Foot Ankle Int 2000;21:370-4.
 |
| Dr. Wu Daniel |
| How to Cite This Article: Daniel W. A Case Report of Spontaneous Second Toe Varus Deformity Correction after Hallux Valgus Deformity Correction by a Non-osteotomy Technique: Syndesmosis Procedure. Journal of Orthopaedic Case Reports 2018. Mar- Apr; 8(2): 42-46. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


