
[box type=”bio”] Learning Point for the Article: [/box]
Diffuse-type tenosynovial giant cell tumor is a benign lesion, but the osteolytic lesion in the spine may mimic an aggressive bone tumor, making the diagnosis potentially challenging.
Case Report | Volume 8 | Issue 3 | JOCR May – June 2018 | Page 14-17| Akio Sakamoto, Atsuji Matsuyama, Masanori Hisaoka, Shuichi Matsuda. DOI: 10.13107/jocr.2250-0685.1088
Authors: Akio Sakamoto[1], Atsuji Matsuyama[2], Masanori Hisaoka[2], Shuichi Matsuda[1]
[1]Department of Orthopaedic Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan,
[2]Departments of Pathology and Oncology, School of Medicine, University of Occupational and Environmental Health, Kitakyushu, Japan.
Address of Correspondence:
Dr. Akio Sakamoto,
Department of Orthopaedic Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
E-mail: akiosaka@kuhp.kyoto-u.ac.jp
Abstract
Introduction: Diffuse-type tenosynovial giant cell tumor (D-TGCT), or pigmented villonodular synovitis, is a benign, but aggressive lesion, primarily involving large joints. The spine is rarely affected, with the involvement of the thoracic spine being particularly rare. Massive bone involvement associated with facet joints is a characteristic of spinal D-TGCT.
Case Report: We report the case of a 26-year-old woman with D-TGCT in her first thoracic vertebral lamina. Computed tomography (CT) showed an osteolytic expansive lesion without the involvement of the facet joint. Magnetic resonance imaging (MRI)revealed a lesion with intermediate signal intensity on T1- and T2-weighted images. After computed tomographically guided biopsy, curettage was performed, and D-TGCTwas diagnosed.
Conclusions: Features of CT and MRI suggested an aggressive bone lesion, and it was challenging to assume D-TGCT, particularly without the involvement of the facet joint.
Keywords: Tenosynovial giant cell tumor, pigmented villonodular synovitis, thoracic, lamina, computed tomography, magnetic resonance imaging.
Introduction
Tenosynovial giant cell tumor (TGCT) is characterized by variable proportions of synovial-like mononuclear cells, multinucleated giant cells, and foamy histiocytes. TGCTs are classified based on whether they have a “nodular” or “diffuse” growth pattern. Diffuse-type TGCT (D-TGCT) is often referred to as pigmented villonodular synovitis (PVNS), and it predominantly affects large joints such as the knees. D-TGCTs tend to be locally aggressive and to recur[1]. D-TGCT arising in the spine is rare. The first case of D-TGCT involving the spine was reported in 1980 [2]. The distribution of spinal D-TGCT has been reported as 44% in the cervical spine, 19% in the thoracic spine, and 33% in the lumbar spine[3]. Spinal D-TGCT is typically located in a posterior element, involving the facet joints [4]. In the present article, we present a case of D-TGCT in the thoracic vertebral lamina without the involvement of the facet joint.
Case Report
A 26-year-old woman noticed nuchal pain without any obvious cause. Plain radiographs showed no obvious findings. Computed tomography (CT) showed an osteolytic expansive lesion in the first thoracic vertebral lamina with a thinned cortex. A pathological fracture of discontinuous cortical bone was observed at the spinal process (Fig. 1).Magnetic resonance imaging (MRI) revealed a lesion with intermediate signal intensity on both T1- and T2-weighted images (Fig. 2).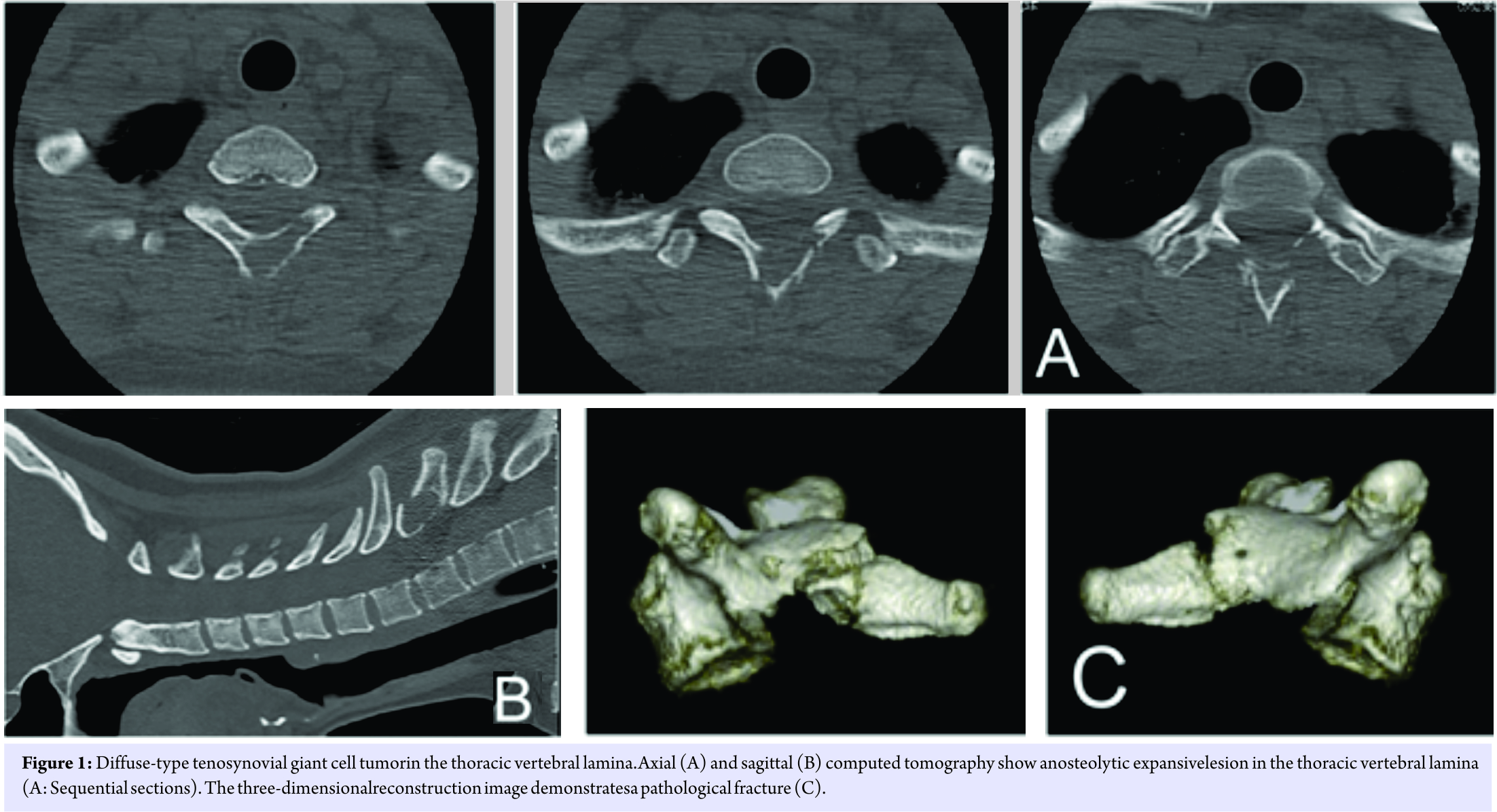 CT-guided biopsy of the lesion was performed. The specimen showed proliferation of mononuclear cells admixed with osteoclast-like multinucleated giant cells. These features suggested benign or borderline giant cell lesions including osteoblastoma or giant cell tumor of bone. The lesion was curetted along with the resection of the thinned outer cortex, leaving the cortical bone intact. The lesion showed no involvement of the facet joint. The curetted specimen revealed proliferating mononuclear cells that were histiocytic. The tumor cells were arranged in a sheet-like fashion embedded in a fibrosclerotic stroma, with osteoclast-like multinucleated giant cells (Fig. 3). Immunohistochemically, osteoclast-like multinucleated giant cells and some mononuclear cells were positive for CD68, a histiocytic marker. Consequently, D-TGCT was finally diagnosed. MRI examination was performed every 6 months after the operation to detect any possible recurrence. No recurrence was seen on MRI examination 1 year and 7 months after the operation.
CT-guided biopsy of the lesion was performed. The specimen showed proliferation of mononuclear cells admixed with osteoclast-like multinucleated giant cells. These features suggested benign or borderline giant cell lesions including osteoblastoma or giant cell tumor of bone. The lesion was curetted along with the resection of the thinned outer cortex, leaving the cortical bone intact. The lesion showed no involvement of the facet joint. The curetted specimen revealed proliferating mononuclear cells that were histiocytic. The tumor cells were arranged in a sheet-like fashion embedded in a fibrosclerotic stroma, with osteoclast-like multinucleated giant cells (Fig. 3). Immunohistochemically, osteoclast-like multinucleated giant cells and some mononuclear cells were positive for CD68, a histiocytic marker. Consequently, D-TGCT was finally diagnosed. MRI examination was performed every 6 months after the operation to detect any possible recurrence. No recurrence was seen on MRI examination 1 year and 7 months after the operation.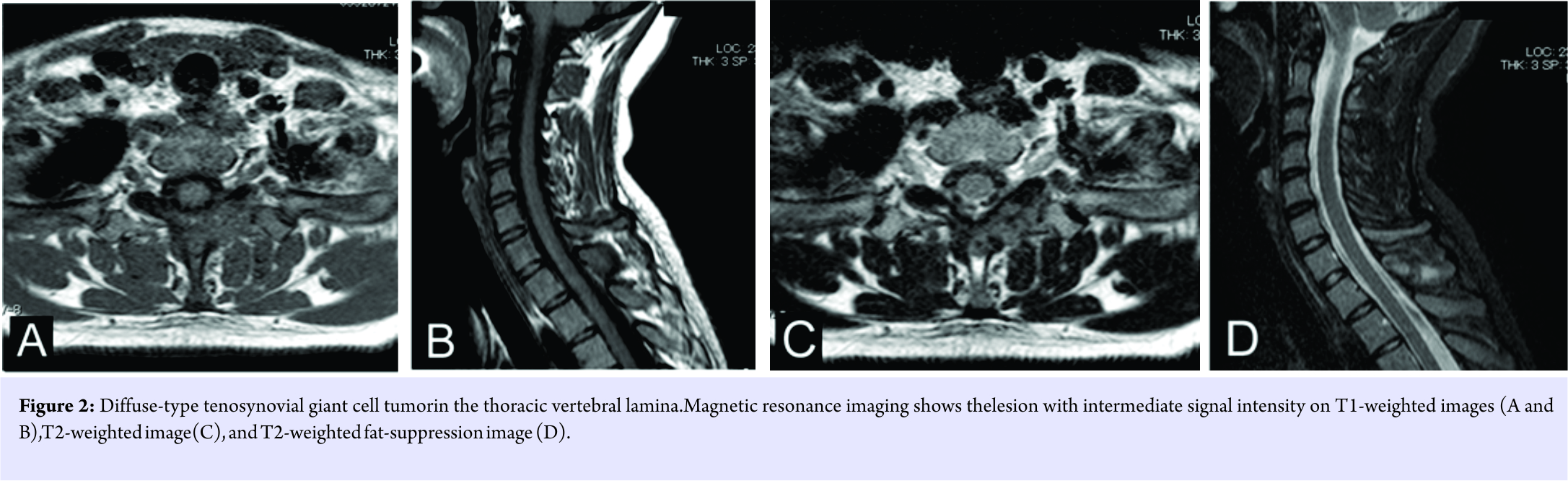
Discussion
D-TGCT in the spine is typically characterized by osteolytic and expansive findings, which are clearly demonstrated by CT [5]. Therefore, differential diagnosis of D-TGCT in the spine includes benign or borderline lesions, such as osteoblastoma and giant cell tumor of bone. Osteolytic lesions centered on the facet joint have been reported to be characteristic of D-TGCT [5]. However, the current case failed to support this finding. Spinal D-TGCT could arise from the atlantoaxial or atlanto-occipital joints, which are a tendon sheath or synovial membrane containing joints, and not a facet joint [4, 6]. D-TGCTs are reported to show low to intermediate signal intensity on both T1- and T2-weighted images on MRI [5, 7]. The signal intensity, particularly on T2-weighted images, is reported to be due to the presence of hemosiderin [5]. However, low to intermediate signal intensity can be observed in giant cell tumor of bone. Therefore, the low to intermediate signal intensity is suggestive of D-TGCT but is not sufficient to distinguish between D-TGCT and giant cell tumor of bone. In the present case, a small CT-guided biopsy sample suggested giant cell lesions, which are common features of the both D-TGCT and giant cell tumor of bone. Because D-TGCT is rare in the spine, D-TGCT may not be considered as a diagnosis at MRI examination, even with histological information from a small sample. Consideration of D-TGCT is important when making a diagnosis of spinal osteolytic lesions. Gross total excision, including curettage, with functional preservation is recommended for D-TGCT in the spine[4]. However, resection of the lesion is sometimes challenging because of the anatomical complexity of the spine. The local recurrence rate of spinal D-TGCT has been reported to be 18–25% [8]. By contrast, the recurrence rate of overall D-TGCT has been reported to be 40–50% [9]. In giant cell tumor of the bone, adjuvant therapy, such as soaking with ethanol, is known to reduce the recurrence rate; however, adjuvant therapy has not been established for D-TGCT. The extent of resection is reported to reduce the recurrence rate [4, 10].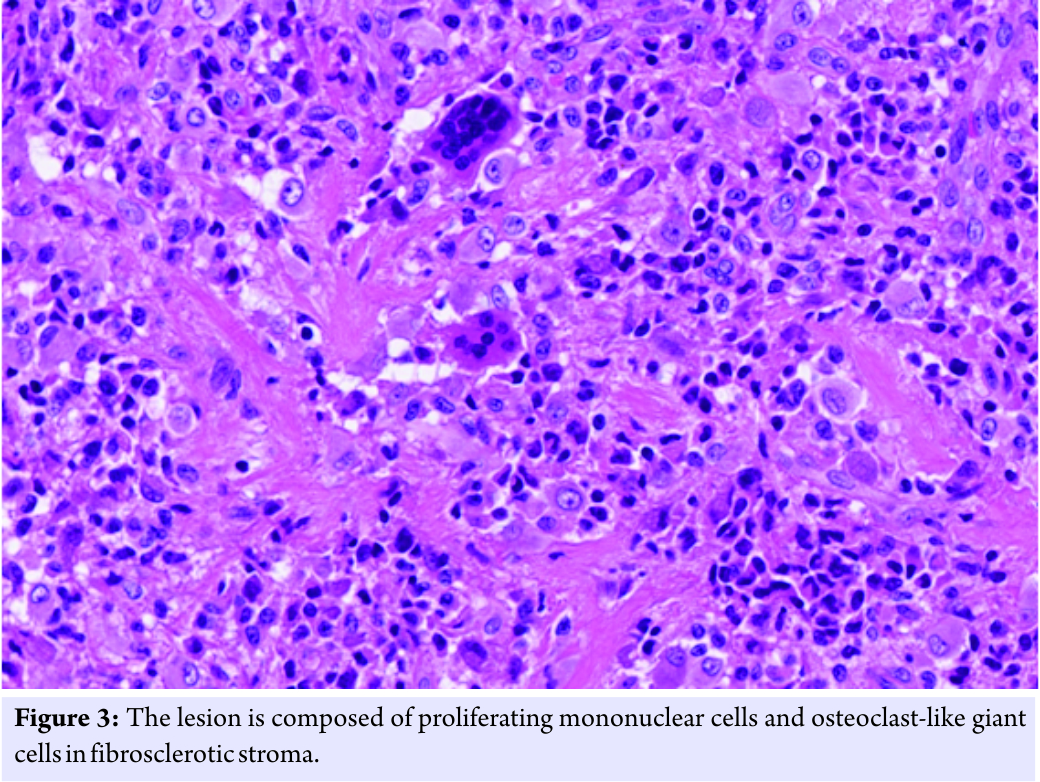
Conclusion
In the present article, a case of D-TGCT in the thoracic vertebral lamina that failed to associate with the facet joint is reported. For diagnosis of D-TGCT, a combination of CT and MRI is useful, but osteolytic lesions may mimic aggressive bone tumors, making the diagnosis potentially challenging. The treatment goal for patients with PVNS is gross total excision of the mass with functional preservation and lowering of recurrence rate [4].
Clinical Message
D-TGCT is a benign, but aggressive lesion, primarily involving large joints. D-TGCT arising in the spine is rare, with the involvement of the thoracic spine being particularly rare. Massive bone involvement associated with facet joints is characteristic of spinal D-TGCT. In the present article, a case of D-TGCT in the thoracic vertebral lamina that failed to associate with the facet joint is reported. For diagnosis of D-TGCT, a combination of CT and MRI is useful, but osteolytic lesions may mimic aggressive bone tumors, making the diagnosis potentially challenging.
References
1. Dorfman HD, Czerniak B. Soft Tissue Tumors. St Louis: CV Mosby; 1995.
2. Kleinman GM, Dagi TF, Poletti CE. Villonodular synovitis in the spinal canal: Case report. J Neurosurg 1980;52:846-8.
3. Oh SW, Lee MH, Eoh W. Pigmented villonodular synovitis on lumbar spine: A case report and literature review. J Korean Neurosurg Soc 2014;56:272-7.
4. Furlong MA, Motamedi K, Laskin WB, Vinh TN, Murphey M, Sweet DE, et al. Synovial-type giant cell tumors of the vertebral column: A clinicopathologic study of 15 cases, with a review of the literature and discussion of the differential diagnosis. Hum Pathol 2003;34:670-9.
5. Lang N, Yuan HS. Computed tomography and magnetic resonance manifestations of spinal pigmented villonodular synovitis. J Comput Assist Tomogr 2015;39:601-6.
6. Blankenbaker DG, Tuite MJ, Koplin SA, Salamat MS, Hafez R. Tenosynovial giant cell tumor of the posterior arch of C1. Skeletal Radiol 2008;37:667-71.
7. Roguski M, Safain MG, Zerris VA, Kryzanski JT, Thomas CB, Magge SN, et al. Pigmented villonodular synovitis of the thoracic spine. J Clin Neurosci 2014;21:1679-85.
8. Clark LJ, McCormick PW, Domenico DR, Savory L. Pigmented villonodular synovitis of the spine. Case report. J Neurosurg 1993;79:456-9.
9. Enzinger FM, Weiss WS. Benign tumors and tumor-like lesions of synovial tissue. Soft Tissue Tumors. 3rd ed. St Louis, MO: CV Mosby; 1995. p. 735-55.
10. Giannini C, Scheithauer BW, Wenger DE, Unni KK. Pigmented villonodular synovitis of the spine: A clinical, radiological, and morphological study of 12 cases. J Neurosurg 1996;84:592-7.
 |
 |
 |
 |
| Dr. Akio Sakamoto | Dr. Atsuji Matsuyama | Dr. Masanori Hisaoka | Dr. Shuichi Matsuda |
| How to Cite This Article: Sakamoto A, Matsuyama A, Hisaoka M, Matsuda S. Bone Involvement Mimicking an Aggressive Bone Lesion in a Diffuse-type Tenosynovial Giant Cell Tumor in the Thoracic Vertebral Lamina: A Case Report. Journal of Orthopaedic Case Reports 2018. May- June; 8(3): 14-17. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


