
[box type=”bio”] Learning Point for the Article: [/box]
Coxa vara in polyostotic fibrous dysplasia can be easily managed by appropriately timed valgus osteotomy to prevent pathological fracture.
Case Report | Volume 8 | Issue 3 | JOCR May – June 2018 | Page33-37 | J K Giriraj Harshavardhan, Bharghava Ram Uppalapati, P Gopinath Menon. DOI: 10.13107/jocr.2250-0685.1096
Authors: J K Giriraj Harshavardhan[1], Bharghava Ram Uppalapati[1], P Gopinath Menon[1]
[1]Department of Orthopaedics, Sri Ramachandra Medical University, Chennai, Tamil Nadu, India.
Address of Correspondence:
Dr. Bharghava Ram Uppalapati,
Department of Orthopaedics, Sri Ramachandra Medical University, Chennai, Tamil Nadu, India.
E-mail: ubrtittu@yahoo.com
Abstract
Introduction: Fibrous dysplasia is a rare benign disorder of the skeletal system characterized by fibro-osseous proliferation with intervening areas of normal or immature bone in the intramedullary region. It can either be a monostotic (involves one bone) or a polyostotic (involves more than one bone) presentation and usually occurs equally in males and females. Deformities such as scoliosis and shepherd’s crook deformity are frequently encountered in the polyostotic form. We report the management of a rare managed case of bilateral shepherd’s crook deformity of the proximal femur with impending neck of femur fracture.
Case Report: A 22-year-old male known case of polyostotic fibrous dysplasia presented with bilateral shepherd’s crook deformity of the proximal femur. Preoperatively, neck-shaft angle was 15° on the right side and 55° on the left side. The patient had severe pain on the right side due to an impending neck of femur fracture. On the right side, we first did a valgus osteotomy in the subtrochanteric region and fixed with dynamic hip screw, and after 3 months, the left proximal femur valgus osteotomy with dynamic hip screw fixation was done. Postoperatively, we achieved a neck-shaft angle of 140° on the right side and 135° on the left side. 1-year follow-up imaging showed union at both the osteotomy sites. At present, at 12-month post-operative, the patient is walking full weight-bearing without support, no apparent shortening.
Conclusion: Valgus osteotomy is an easy and effective method to correct the shepherd’s crook deformity and achieve correct mechanical alignment. Valgization of the shepherd crook deformity will prevent the development of a pathological neck of femur fracture.
Keywords: Fibrous dysplasia, dynamic hip screw, valgus osteotomy, coxa vara.
Introduction
The term “Fibrous Dysplasia” was given by Lichtenstein in 1938 [1]. Fibrous dysplasia is a rarebenign disorder of the skeletal system. Fibrous dysplasia is a developmental anomaly of bone formation that may exist in a monostotic or polyostotic form. The hallmark is replacement of normal bone and marrow by fibrous tissue and small, woven spicules of bone [6]. Fibrous dysplasia can occur in the epiphysis, metaphysis, or diaphysis. Almost any bone in the body can be involved, but polyostotic form tends to involve the craniofacial bones, ribs, and metaphysis or diaphysis of femur and tibia more commonly. Lesions tend to be present on one side of the body. Deformities such as scoliosis and shepherd’s crook deformity are frequently encountered in the polyostotic form. The latter deformity is thought to be characteristic of the polyostotic form. It involves curvature in the proximal femur neck and proximal shaft resulting in coxa vara deformity. Associated abnormalities, such as sexual precocity, abnormal skin pigmentation, intramuscular myxoma, and thyroid disease, may be present. McCune-Albright syndrome refers to polyostotic fibrous dysplasia, cutaneous pigmentation, and endocrine abnormalities [2]. Mazabraud syndrome is polyostotic fibrous dysplasia with intramuscular myxomas. Malignant change has been reported occasionally with and without prior radiotherapy. The radiographic appearance is characteristic, with the lucent area having a granular, ground-glass appearance with a well-defined sclerotic rim [3]. Occasionally, biopsy is necessary to establish the diagnosis. The histopathological appearance is that of irregular woven bone spicules with a fibrous stroma [6]. Small areas of cartilaginous metaplasia and cystic changes may be present. Surgical treatment is indicated when significant deformity or pathological fracture occurs or when significant pain exists. Actual and impending pathological fractures are best treated with intramedullary fixation when possible [4]. Deformities are corrected by osteotomy with internal fixation. The lesions persist either partially or completely in spite of the vigorous treatment and tend to recur. However, the associated pathological fractures or the osteotomies done for the correction of the deformity have excellent union rates [8]. Shepherd’s crook deformity, which is mainly a metaphyseal deformity, the goal of treatment is to prevent the recurrence by achieving mechanical alignment of the proximal femur and then internally splinting it. Recurrence is common in the managed cases and is more commonly seen with simple curettage and bone grafting. The cases reported in the literature are mostly the unilateral cases with either a single stage or two-stage correction. We report a rare managed case of bilateral shepherd’s crook deformity of the proximal femur with impending fracture neck of femur in a case of polyostotic fibrous dysplasia.
Case Report
A 21-year-old male presented to us with bilateral hip pain right more than left for 2 years and difficulty to walk for the past 6 months. 2 years back, the patient experienced pain in both hips insidious in onset gradually progressive aggravated while walking relived on rest. Then, the patient was walking with support, and for the past 6 months, the patient was not able to bear weight and pain was severe on the right side. The patient is a known case of polyostotic fibrous dysplasia was diagnosed around 10 years of age. The patient was initially able to walk with the help of walker, unable to do activities of daily living, unable to sit cross-legged, and unable to squat. There is no history of trauma or any constitutional symptoms. Clinical findings were consistent with coxa vara deformity of bilateral hips. There was no evidence of any endocrine disturbance or altered pigmentation or precocious puberty. On imaging, it was concluded that the patient suffered from polyostotic fibrous dysplasia with bilateral severe shepherd’s crook deformity of the proximal femur with measured neck-shaft angle of 15° on the right side and 55° on the left side (Fig. 1). Whole body bone scan showed multiple areas of increased tracer uptake (Fig. 2).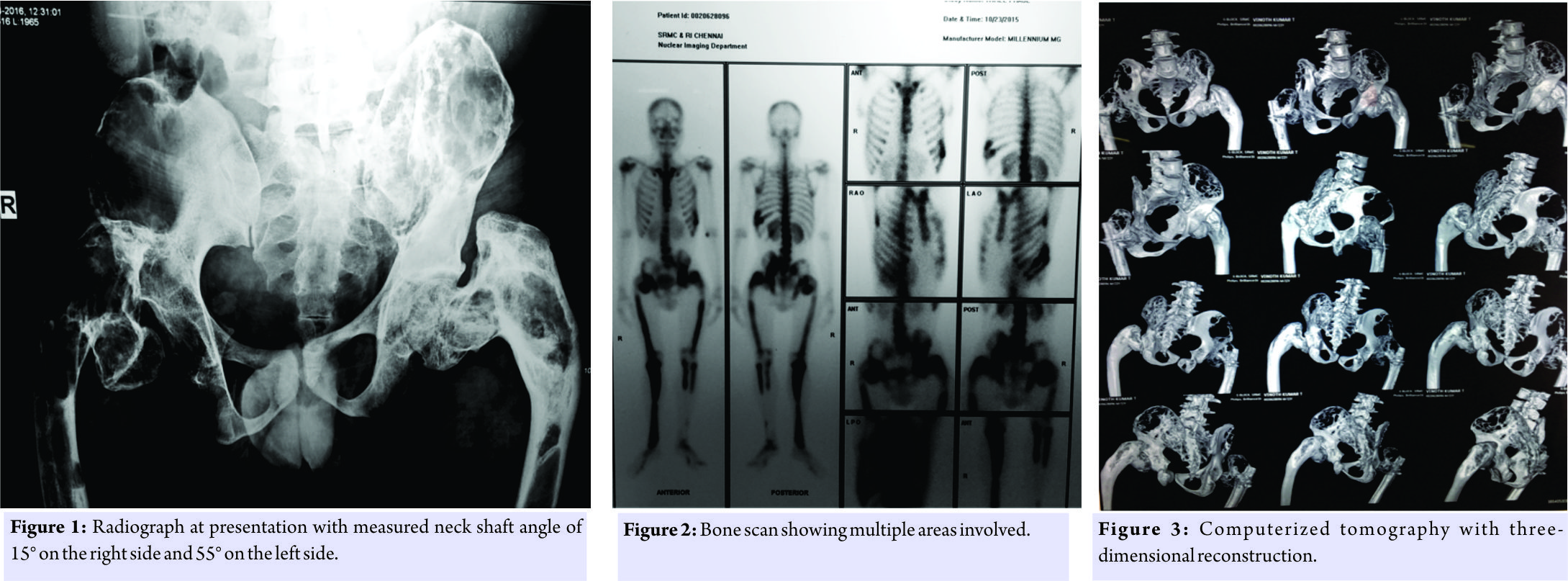 Computerized tomography of the pelvis showed features consistent with fibrous dysplasia of the proximal femur with bilateral shepherd’s crook deformity, also bilateral iliac wing, sacral ala, L3,4,5,S1, and 2 are also involved (Fig. 3).
Computerized tomography of the pelvis showed features consistent with fibrous dysplasia of the proximal femur with bilateral shepherd’s crook deformity, also bilateral iliac wing, sacral ala, L3,4,5,S1, and 2 are also involved (Fig. 3). All the blood and serum biochemical investigations of the patient such as the hemoglobin, total and differential white cell counts, erythrocyte sedimentation rate, C-reactive protein, calcium, phosphorus, and alkaline phosphatase levels, and all the hormonal studies were within normal limits. It was decided to do correction of the deformity to realign the head, neck, and shaft and to achieve valgus at the neck shaft region, in one stage, each side at a time. On the right side, lateral closing wedge osteotomy was done at the subtrochanteric level to achieve alignment of the shaft with the proximal femur and fixed with a 135° dynamic Richard’s screw with a six-holed long side plate. 3 months later on the left side, lateral closing wedge osteotomy was performed at the subtrochanteric level to align the distal shaft with the proximal femur. Fixation was done using a 135° dynamic Richard’s screw with a six-holed long side plate to span osteotomy site. Postoperatively, we achieved a neck-shaft angle of 140° on the right side and 135° on the left side (Fig. 4 and 5). The patient was started on active and passive quadriceps strengthening exercises, and after 6 weeks of immobilization, toe touch weight-bearing was started followed gradually by partial and complete weight-bearing mobilization. Follow-up imaging showed union at both the osteotomy sites bilaterally. At present, at 12-month postoperatively (Fig. 6), the patient is walking full weight-bearing without support and there are no signs of recurrence of lesions of fibrous dysplasia or the deformity (Fig. 7 and 8).
All the blood and serum biochemical investigations of the patient such as the hemoglobin, total and differential white cell counts, erythrocyte sedimentation rate, C-reactive protein, calcium, phosphorus, and alkaline phosphatase levels, and all the hormonal studies were within normal limits. It was decided to do correction of the deformity to realign the head, neck, and shaft and to achieve valgus at the neck shaft region, in one stage, each side at a time. On the right side, lateral closing wedge osteotomy was done at the subtrochanteric level to achieve alignment of the shaft with the proximal femur and fixed with a 135° dynamic Richard’s screw with a six-holed long side plate. 3 months later on the left side, lateral closing wedge osteotomy was performed at the subtrochanteric level to align the distal shaft with the proximal femur. Fixation was done using a 135° dynamic Richard’s screw with a six-holed long side plate to span osteotomy site. Postoperatively, we achieved a neck-shaft angle of 140° on the right side and 135° on the left side (Fig. 4 and 5). The patient was started on active and passive quadriceps strengthening exercises, and after 6 weeks of immobilization, toe touch weight-bearing was started followed gradually by partial and complete weight-bearing mobilization. Follow-up imaging showed union at both the osteotomy sites bilaterally. At present, at 12-month postoperatively (Fig. 6), the patient is walking full weight-bearing without support and there are no signs of recurrence of lesions of fibrous dysplasia or the deformity (Fig. 7 and 8).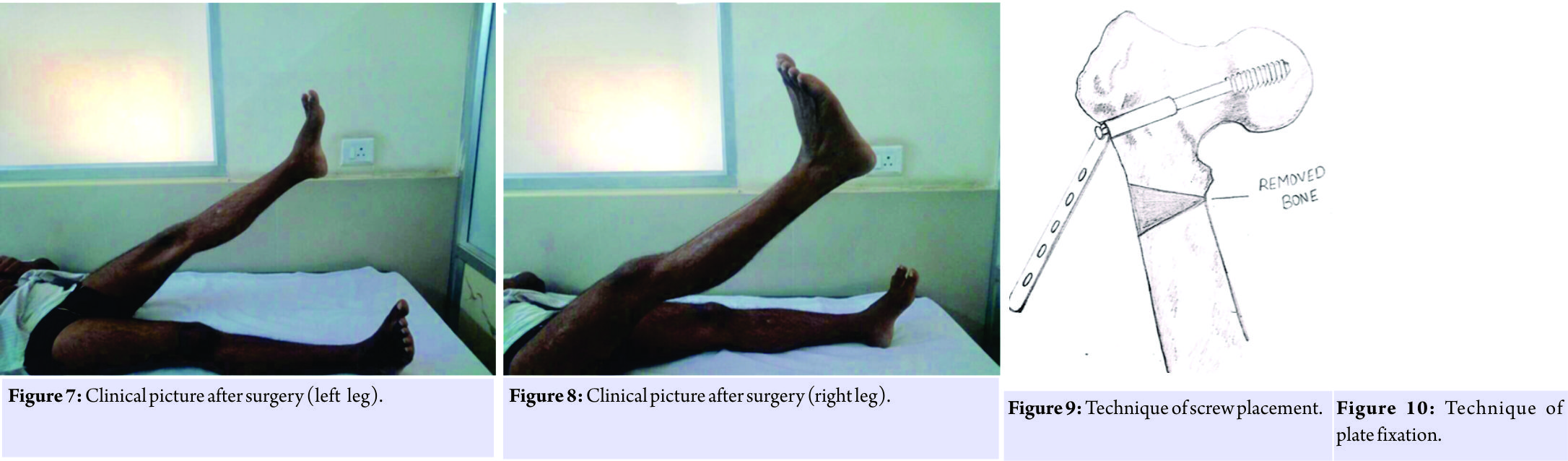
Discussion
Although pathologically fibrous dysplasia is described as a benign condition, clinically, it is associated with a significant morbidity and decreased quality of life, especially with lesions of the lower limb, like in our patient [5]. Our patient presented to us in his second decade of life with shepherd’s crook deformity of bilateral proximal femur and decreased quality of life. Every time shepherd’s crook deformity manifests in a different way and at a different stage; thus, a tailored approach should be adopted for treating them [4]. This is the reason of having varied ways described for approaching this particular deformity [3, 4]. Irrespective of the customized approach chosen for the management of this deformity, it is of utmost importance to achieve the correct alignment and union. In our experience, dynamic hip screw fixation provides a more versatile method of fixing the shepherd’s crook deformity of proximal femur, the 135° plate with barrel will act as a template to correct the neck-shaft angle once the Richard’s screw is exactly in center of the neck and head of femur both in anterioposterior and lateral views (Fig. 9 and 10). Furthermore, a desired length of the side plate depending on the extent of lesion helps to span the lesion completely and prevent recurrence. Only the placement of the osteotomy will vary depending on the extent of the disease and the amount of deformity. Union of the osteotomy is usually not an issue, as once the mechanical alignment is achieved, union is usually achieved [7, 8]. Correction of the shepherd’s crook deformity in single stage maximizes rehabilitation and also decreases the operative morbidity experienced by patient [9]. It is difficult to achieve single stage correction using an intramedullary implant as the femur is excessively bowed, and in such cases, dynamic hip screw fixation should be preferred [4, 9]. Thus, valgus osteotomy with dynamic hip screw fixation is a versatile, effective, easier, and a practical approach to correct the morbid shepherd’s crook deformity of proximal femur.
Conclusion
Valgus osteotomy is an easy and effective method to correct the shepherd’s crook deformity and achieve correct mechanical alignment of the proximal femur in patients with fibrous dysplasia. Dynamic hip screw is a versatile and preferred implant to tackle the proximal femur deformity in cases of fibrous dysplasia. Using a long side plate with the dynamic hip screw helps to span the lesion and prevent the recurrence of the deformity. Customized approach should be adopted to tackle the proximal femur shepherd’s crook deformity in cases of fibrous dysplasia. Correcting the shepherd crook deformity will prevent a pathological neck of femur fracture.
Clinical Message
Identification and early correction of coxa vara due to fibrous dysplasia will prevent progression of deformity, shortening, and pathological fracture neck of femur. In a shepherd crook deformity, even though correction is technically difficult, satisfactory results can be achieved with a well-planned corrective valgus osteotomy.
References
1. LichtensteinL.Polyostoticfibrousdysplasia.(1938)ArchSurg36:874.
2. Leet AI, Chebli C, Kushner H, Chen CC, Kelly MH, Brillante BA, et al. Fracture incidence in polyostotic fibrous dysplasia and the mcCune-albright syndrome. J Bone Miner Res 2004;19:571-7.
3. Ippolito E, Farsetti P, Boyce AM, Corsi A, De Maio F, Collins MT, et al. Radiographic classification of coronal plane femoral deformities in polyostotic fibrous dysplasia. Clin Orthop Relat Res 2014;472:1558-67.
4. Stephenson RB, London MD, Hankin FM, Kaufer H. Fibrous dysplasia. An analysis of options for treatment. J Bone Joint Surg Am 1987;69:400-9.
5. Stewart MJ, Gilmer WS, Edmonson AS. Fibrous dysplasia of bone. J Bone Joint Surg Br 1962;44-B:302-18.
6. Harris WH, Dudley HR Jr. Barry RJ. The natural history of fibrous dysplasia. An orthopaedic, pathological, and roentgenographic study. J Bone Joint Surg Am 1962;44-A:207-33.
7. Sofield HA, Page MA, Mead NC. Multiple osteotomies and metal-rod fixation for osteogenesis imperfecta. J Bone Joint Surg 1952;34A:500-2.
8. Guille JT, Kumar SJ, MacEwen GD. Fibrous dysplasia of the proximal part of the femur. J Bone Joint Surg 1998;80-A:648-58.
9. Kandhari VK, Bava SS, Desai MM, Wade RN. Single Stage Treatment of Non – Union of Transcervical Neck Femur Fracture with Shepherd Crook Deformity of Proximal Femur in A Case of Fibrous Dysplasia using Dynamic Hip Screw Fixation. Journal of Orthopaedic Case Reports 2015 July – Sep;5(3): 41-44
 |
 |
 |
| Dr. J K Giriraj Harshavardhan | Dr. Bharghava Ram Uppalapati | Dr. Gopinath Menon |
| How to Cite This Article: Harshavardhan J K G, Uppalapati B R, Menon P G. A Case of Fibrous Dysplasia with Bilateral Shepherd Crook Deformity Treated with Dynamic Hip Screw Fixation. Journal of Orthopaedic Case Reports 2018. May-June; 8(3): 33-37. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


