
[box type=”bio”] Learning Point for the Article: [/box]
Osteochondroma of the scapula is an unusual site of presentation. Congenital Osteochondroma of the scapula is extremely rare and has not been reported before to the best of our knowledge
Case Report | Volume 8 | Issue 3 | JOCR May – June 2018 | Page 38-41| . DOI: 10.13107/jocr.2250-0685.1098
Authors: Supreeth Nekkanti[1], Alok Moogali[1], Archana Meka[1], Malavika Nair[1]
[1]Department of Orthopaedics, JSS Medical College and Hospital, Mysore, Karnataka, India.
Address of Correspondence:
Dr. Supreeth Nekkanti,
Department of Orthopaedics, JSS Medical College and Hospital, Mysore – 570008, Karnataka, India.
E-mail: drsupreethn@gmail.com
Abstract
Introduction: Osteochondroma of the scapula is a rare tumour of the thorax. It constitutes 14.4% of all tumours of the scapula with the ventral surface being the most common site of presentation [1]. The dorsal surface of the scapula is rarely seen as a potential site for the origin of osteochondroma from our review of the literature, which was the case in our patient. Most of the patients presenting with osteochondroma on the dorsal aspect of scapula have been reported to be of the sessile variant.
Case Report: We report two rare cases of a pedunculated variety of osteochondroma at an unusual site-dorsal surface of the scapula in a 19-year-old male and a 5-year-old male child. The tumours were excised and the diagnosis was confirmed by histopathological studies.
Conclusion: This case series is reported for its rarity and its unusual site of presentation. A solitary congenital variant of osteochondroma of the scapula has never been reported to the best of our knowledge.
Keywords: Scapula, osteochondroma, dorsal surface.
Introduction
Osteochondroma of the scapula is a rare tumour of the thorax. It constitutes 14.4% of all tumours of the scapula with the ventral surface being the most common site of presentation[1]. The dorsal surface of the scapula is rarely seen as a potential site for the origin of osteochondroma from our review of the literature, which was the case in our patient. Most of the patients presenting with osteochondroma on the dorsal aspect of scapula have been reported to be of the sessile variant. We report two rare cases of a pedunculated variety of osteochondroma at an unusual site-dorsal surface of the scapula in a 19-year-old male and a 5-year-old male child. The tumours were excised and the diagnosis was confirmed by histopathological studies. This case series reported for its rarity and its unusual site of presentation.
Case Report
Case 1
A 19-year-old male presented to us with complaints of swelling over the left upper back for 2 years. He complained of discomfort while sleeping on his back and while moving left shoulder for1 year. It was spontaneous in onset and gradually progressive. It was not associated with any history of trauma, fever, difficulty in breathing, weight loss, or history of similar complaints in the past. On examination, a hard, oval bony swelling of size 3 cm× 3 cm was palpable on the dorsum of left scapula along the medial border, non-tender, and fixed to the scapula and with normal pinchable overlying skin(Fig. 1). There was no sensory or motor deficit in the left upper limb with a full range of motion of the left shoulder. There was no evidence of any other swelling in the body. X-ray of the left shoulder was taken in anteroposterior and scapular Y view, which revealed a bony swelling arising from the dorsal surface of the left scapula(Fig. 2). Computed tomography (CT) scan showed a pedunculated mushroom-like mass arising from the dorsal aspect of the medial border of the scapula. There was no evidence of any pathological fracture or ventral extension or chest wall abnormality (Fig. 3). A provisional diagnosis of pedunculated osteochondroma of the left scapula was made. An excision biopsy was planned for the patient.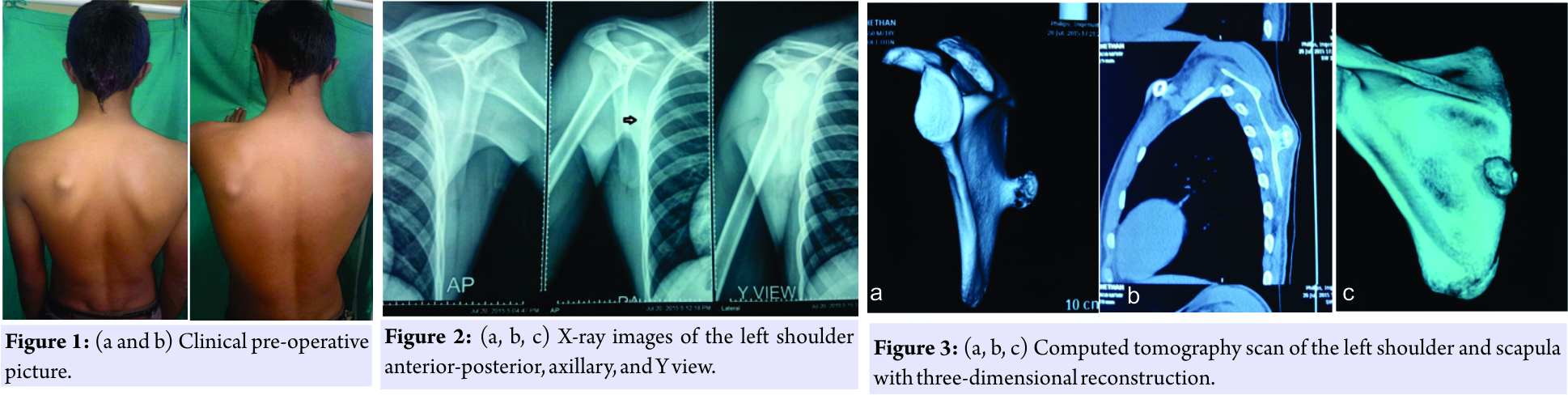
Case 2
A 5-year-old male child presented to us with complaints of a swelling over the dorsal aspect of the left shoulder for birth. It was spontaneous in onset and gradually progressed to the present size. On examination, a hard, oval bony swelling of size 1.5 cm× 1cm was palpable on the dorsum of the left scapula along the medial border, non-tender, and fixed to the scapula and with normal pinchable overlying skin. There was no sensory or motor deficit in the left upper limb with a full range of motion of the left shoulder. There was no evidence of any other swelling in the body. Plain radiographs were inconclusive. CT scan of the left shoulder revealed a pedunculated osteochondroma arising from the dorsal aspect of the scapula.
Surgical technique
Under general anaesthesia, the patient was made to lie the prone position. After preparing the left shoulder, a sterile drape was applied. A 3 cm incision was made parallel to the medial border of the scapula over the swelling. The trapezius was dissected and the borders of the mass were delineated(Fig. 4).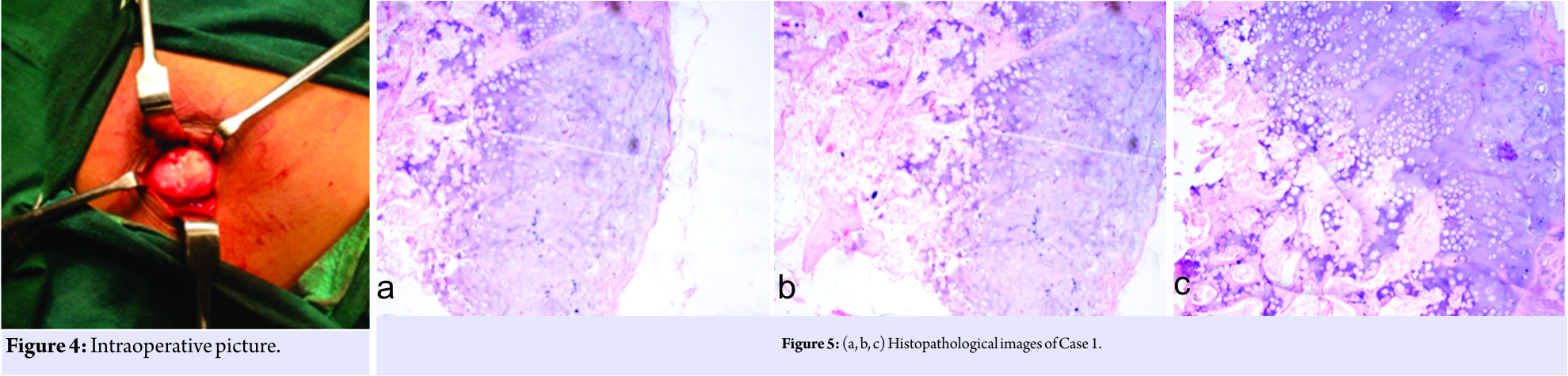 The stalk was identified and the mass was excised in toto. The remnant stump was nibbled and dorsal surface of the scapula was smoothened using a file. The excised mass was sent for histopathological studies. A similar approach was used for both the patients. Histopathological studies both the patients confirmed the diagnosis of osteochondroma (Fig. 5, 6, 7, 8, 9).
The stalk was identified and the mass was excised in toto. The remnant stump was nibbled and dorsal surface of the scapula was smoothened using a file. The excised mass was sent for histopathological studies. A similar approach was used for both the patients. Histopathological studies both the patients confirmed the diagnosis of osteochondroma (Fig. 5, 6, 7, 8, 9).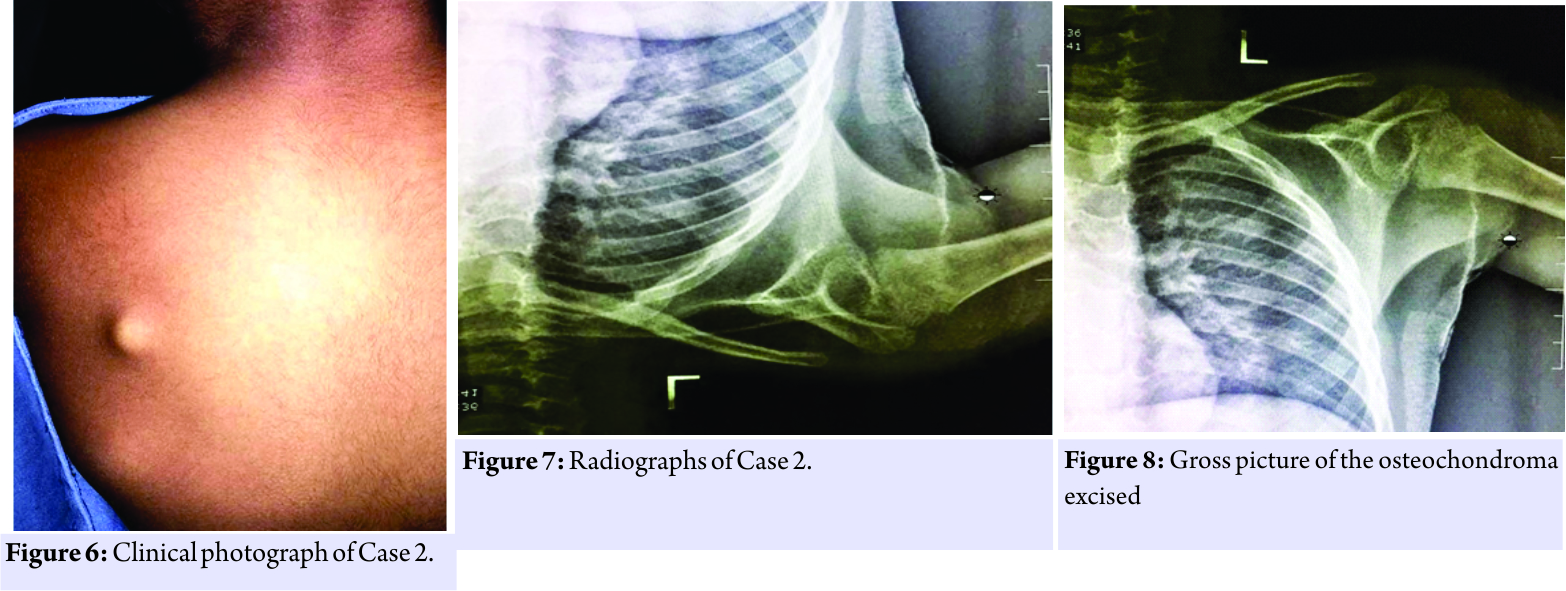 Macroscopy showed bony fragment with soft tissue attachments of size 5 cm × 4 cm × 1 cm. Microscopy revealed multiple sections of bone fragments were seen with a cartilaginous cap with trabecular bone and fatty tissue. The cartilaginous cap was 3mm in thickness. The macroscopy of the second patient revealed single bony tissue fragment of size 1.5 cm× 1cm and microscopy showed bony trabeculae enclosing marrow spaces being capped by hyaline cartilage which was consistent with osteochondroma The patient was immobilized using an arm pouch. On the 3rd post-operative day, the patient developed a fever with multiple episodes of vomiting. His platelet count had dropped to 20,000/cumm and tested positive for dengue serology. His liver function tests were normal. The patient was transfused two units of platelet concentrate. He was kept nil oral with continuous fluid and electrolytes infusion. On the 6th post-operative day, the patient was symptomatically better. His operative wound was healthy. Platelets picked up to 52,000/cumm. Sutures were removed on the 10th post-operative day for both the patients. Pendulum exercises and shoulder strengthening exercises were initiated after suture removal. The patients were otherwise asymptomatic. The second patient post-operative period was uneventful. Sutures were removed on the 10th post-operative day.
Macroscopy showed bony fragment with soft tissue attachments of size 5 cm × 4 cm × 1 cm. Microscopy revealed multiple sections of bone fragments were seen with a cartilaginous cap with trabecular bone and fatty tissue. The cartilaginous cap was 3mm in thickness. The macroscopy of the second patient revealed single bony tissue fragment of size 1.5 cm× 1cm and microscopy showed bony trabeculae enclosing marrow spaces being capped by hyaline cartilage which was consistent with osteochondroma The patient was immobilized using an arm pouch. On the 3rd post-operative day, the patient developed a fever with multiple episodes of vomiting. His platelet count had dropped to 20,000/cumm and tested positive for dengue serology. His liver function tests were normal. The patient was transfused two units of platelet concentrate. He was kept nil oral with continuous fluid and electrolytes infusion. On the 6th post-operative day, the patient was symptomatically better. His operative wound was healthy. Platelets picked up to 52,000/cumm. Sutures were removed on the 10th post-operative day for both the patients. Pendulum exercises and shoulder strengthening exercises were initiated after suture removal. The patients were otherwise asymptomatic. The second patient post-operative period was uneventful. Sutures were removed on the 10th post-operative day.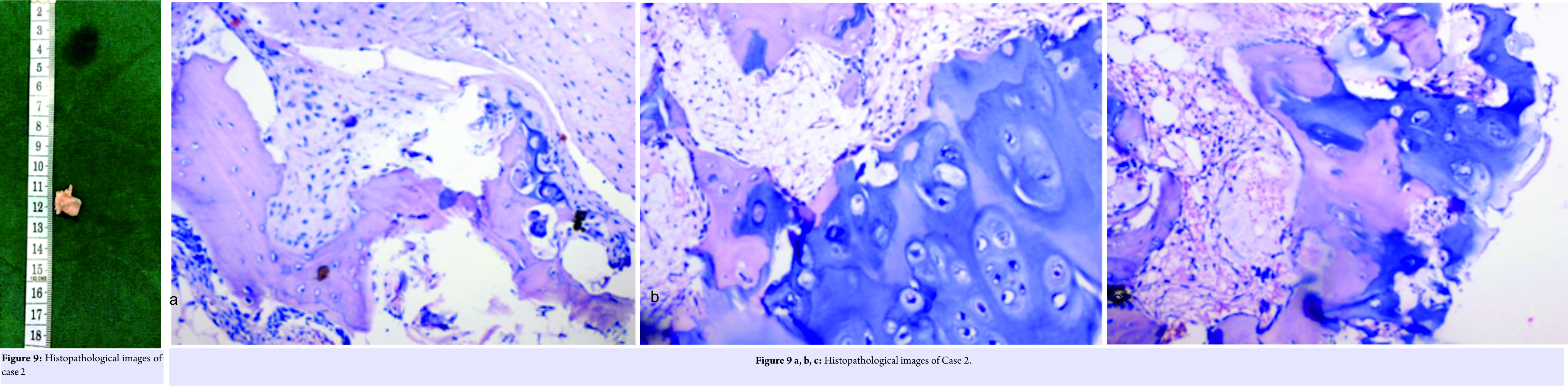
Discussion
Osteochondroma of the scapula is a rare tumour of the thorax. It constitutes 14.4% of all tumours of the scapula with the ventral surface being the most common site of presentation[1]. The dorsal surface of the scapula is rarely seen as a potential site for the origin of osteochondroma from our review of the literature, which was the case in our patient. Most of the patients presenting with solitary osteochondroma of the scapula have been reported to be of the sessile variant. Despite its unknown aetiology, a peripheral portion of the physis is thought to herniate from the growth plate [2, 3]. This metaplastic cartilage grows to form the exostosis, which is connected to the bone by a thin stalk. Osteochondroma commonly occurs at the age of<30 years, with a male-to-female ratio of >1.5:1 [4]. Our patient was a male of 19 years of age. He presented with a painless bony mass which is the most commonly reported symptom [3]. Pain, if present, is mostly due to the mass effect of tumour on the surrounding tissue. A wide range of other presentations includes a decreased range of motion, nerve impingement, underlying bursitis, fracture of the stalk of the tumour, and “pseudo-winging” of the scapula [2, 4]. Snapping scapula syndrome, which is a syndrome of painful, audible, and/or palpable abnormal scapula thoracic motion, can develop when the osteochondroma is presented on the anterior surface of the scapula, especially in adolescence or early adulthood [5]. Osteochondromas of the ventral surface of the scapula lead to potential problems such as bursa formation, pseudo-winging of the scapula, snapping syndrome, and restricted movements of the shoulder, most of which are relieved by excision of the tumour [6, 7, 8, 9]. Solitary osteochondromas have a 3% chance of converting into an osteosarcoma. This was one of the reasons why she was operated and the tumour excised. This risk increases to 10% for patients with hereditary multipleexostosis [5]. Malignant transformation is characterized by a sudden increase in the size of the tumour accompanied by pain. Osteochondromas are usually not difficult to diagnose clinically, but confirmation is a must by histopathological studies of the biopsy taken. Radiographic studies such as X-ray and CT scan are essential for isolating the location of the mass and planning surgical approach [3]. In our patient, a CT scan with three-dimensional reconstruction of the shoulder was done and it revealed the mass was a pedunculated mushroom-like swelling arising from the dorsal aspect of the scapula along the medial border of the scapula. Magnetic resonance imaging is usually reserved for cases in which malignancy is suspected. Histopathology of osteochondroma showed endochondral bone connected to normal bone by a thin stalk in continuity with the medullary canal of the native bone. The thickness of the cartilaginous cap seen in the biopsy specimen also is one of the predicting factors for malignant transformation [3]. A cartilaginous cap thickness of <1 cm indicates a benign condition, whereas a cap thicker than 2 cm should raise concern for malignant transformation [1, 3]. The biopsy of our patient revealed the thickness of the cartilaginous cap to be of 3cm, which indicated a possibly significant malignant potential. Osteochondromas usually stop growing at the time of closure of the physis and growth into adulthood should also raise suspicion for possible malignancy [1]. The only definitive treatment of osteochondroma is enbloc excision of the tumour [3, 4]. After narrowing down the location of the mass with the aid of CT scan, we planned a surgical approach parallel to the medial border of the scapula. Endoscopic resection is gaining popularity due to claims of earlier functional recovery, better results in terms of pain relief, post-operative performance, and cosmetic outcome due to a smaller incision [4, 8]. In our patient, the incision made was only a 4 cm one and we wanted to give importance to resecting the tumour completely. The overall prognosis is good with relapse being very rare, usually occurring when tumour margins are not cleared completely and residual fragments of cartilage cap or periosteum remain following excision [1,10]. Incomplete excisions lead to a 2% recurrence risk[10]. The decision for surgery was taken because of the increasing size and discomfort for the patient for 1 year.
Conclusion
Solitary osteochondromas of the scapula are rare and most of the time present on the ventral surface of scapula causing snapping shoulder syndrome. Unusual site of presentation such as the dorsal surface of scapula must also be thought of while clinically examining the patient. Surgeons must strive to completely resect the tumour to negate the risk of recurrence. Surgical excision should be done at the earliest for symptomatic cases to reduce the risk of malignant transformation.
Clinical Message
The purpose of this study is to report two patients with a rare presentation of a solitary osteochondroma on the dorsal surface of the scapula. One of them presented with a tumour since birth. This unusual, rare form of presentation of a solitary osteochondroma has not been reported before in the literature and hence poses a diagnostic challenge while managing such patients.
References
1. Frank RM, Ramirez J, Chalmers PN, McCormick FM, Romeo AA. Delayed presentation of osteochondroma on the ventral surface of scapula. Int J Shoulder Surg 2012;6:61-3.
2. Essadki B, Moujtahid M, Lamine A, Fikry T, Essadki O, Zryouil B. Solitary osteochondroma of the ribs: Clinical review of 76 cases. Acta Orthop Belgica 2000;66:146-53.
3. Mahajan S, Mahajan N, Singh P, Shikari AB, Sharma RC. Scapula, a rare localization of osteochondroma: A case report. Internet J Orthop Surg 2008;14. Available from: http://www.ispub.com/IJOS/14/1/13570. [Last cited on 2014 Feb 03].
4. Chillemic C, Franceschini V, Ippolito G, Roberto P, Franceschini V. Osteochondroma as a cause of winging scapula in an adolescent. J Med Case Rep 2013;7:220.
5. Fukunaga S, Hiroyuki Futani H, Yoshiya S. Endoscopic assisted resection of a scapular osteochondroma causing snapping scapula syndrome. World J Surg Oncol 2007;5:37.
6. Danielson LG, el-Haddad I. Winged scapula due to osteochondroma: Report of 3 children. Acta Orthop Scand 1989;60:728-29.
7. Okada K, Terada K, Sashi R, Hoshi N. Large bursa formation associated with osteochondroma of the scapula: A case report and review of the literature. Jpn J Clin Oncol 1999;29:356-60.
8. Mohsen MS, Moosa NK, Kumar P. Osteochondroma of the scapula associated with winging and large bursa formation. Med Princ Pract Surg Am 1950;32:561-56.
9. Reit RP, Glabbeek FV. Arthroscopic resection of a symptomatic snapping subscapular osteochondroma. Acta Orthop Belg 2007;73:252-54.
10. Ceberut K, Korkmaz M, Ergin I, Müslehiddinoglu A. Bursa formation with scapular osteochondroma in hereditary multiple exostoses. J Coll Physicians Surg Pak 2013;23:512-4.
 |
 |
 |
 |
| Dr. Supreeth Nekkanti | Dr. Alok Moogali | Dr. Archana Meka | Dr. Malavika Nair |
| How to Cite This Article: Nekkanti S, Moogali A, Meka A, Nair M. An Unusual Presentation of Osteochondroma on the Dorsal Surface of the Scapula: A Review of Two Patients. Journal of Orthopaedic Case Reports 2018. May- June; 8(3): 38-41. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


