
[box type=”bio”] Learning Point of the Article: [/box]
Medical practitioners must consider the possibility of soft tissue sarcoma in patients that present with a benign looking mass.
Case Report | Volume 8 | Issue 6 | JOCR November – December 2018 | Page 13-15| Konstantinos Papageorgiou, Peter Goodwin, John Travlos, Asterios Dramis. DOI: 10.13107/jocr.2250-0685.1236
Authors: Konstantinos Papageorgiou[1], Peter Goodwin[2], John Travlos[1], Asterios Dramis[3]
[1]Department of Trauma and Orthopaedics, The Royal Wolverhampton Hospitals NHS Trust, New Cross Hospital, Wolverhampton, WV10 0QP, UK,
[2]Medical Student, Warwick Medical School, University of Warwick, Coventry CV4 7AL, UK,
[3]Department of Trauma and Orthopaedics, George Eliot Hospital NHS Trust, Nuneaton, CV10 7DJ, UK.
Address of Correspondence:
Dr. Asterios Dramis,
38 Pakenham Road, Birmingham, B15 2NE, UK.
E-mail: ad199@doctors.org.uk
Abstract
Introduction: Soft tissue sarcomas are rare tumors that often present with pain, increasing size and a location deep to the fascia. If they do not present with the aforementioned symptoms and signs, delayed diagnosis can occur.
Case Report: We present an unusual case of a 51-year-old patient who presented with clinical features of a benign mass of the lower limb that turned out to be a soft tissue sarcoma – a leiomyosarcoma.
Conclusion: Medical practitioners must consider the possibility of soft tissue sarcoma in patients that present with a benign looking mass. Diagnostic imaging can be inconclusive on these cases and definite diagnosis is made on histological examination. Treatment includes surgery and radiotherapy.
Keywords: Leiomyosarcoma, Lower limb, Soft tissue.
Introduction
Most soft tissue sarcomas present with features of a large and painful mass, which is increasing in size and have a location which is deep to fascia. There are soft tissue sarcomas though that present with clinical features of a benign tumor such as slow growth, painless, and superficial locality. Park et al. [1] presented a series of 18 cases where patients presented with a superficial mass of a limb whose misleading clinical features led to a delayed diagnosis of a soft tissue sarcoma. We present an interesting case where a mass in a lower limb with benign clinical features was later diagnosed as a soft tissue sarcoma.
Case Report
A 51-year-old male patient presented with 5years history of a lump on the front of his left knee. The lump was about 5 cm in size around the tibial tubercle, subcutaneous, firm and mobile, not tender,and not translucent, there were no associated dilated veins, and the patient had full and pain-free range of movements of his left knee. It had the clinical features of a benign tumor. It was thought to be an infrapatellar bursa related to the knee. Hence, a “watch and wait” policy was initially adopted as the patient was asymptomatic. No medications or other treatments were provided. There was no change in the size of the lump, but a year later as the lump became itchy and, therefore, symptomatic, the patient decided to follow the surgical intervention route. Therefore, further investigations were advised. A plain radiograph of his knee showed medial joint space narrowing with small osteophytes (Fig. 1). A small effusion was present but no chondrocalcinosis. There was no periosteal involvement, no cortical irregularity, and no local osteopenia, but a soft tissue swelling was apparent on the anterior part of the knee. A magnetic resonance imaging scan showed a well-defined lump measuring 2.7 cm × 1.7 cm × 4.1cm within the subcutaneous fat just medial to the tibial tuberosity, did not involve the pes anserinus, neither the underlying bone nor the knee joint, and there was no evidence of infection (Fig. 2).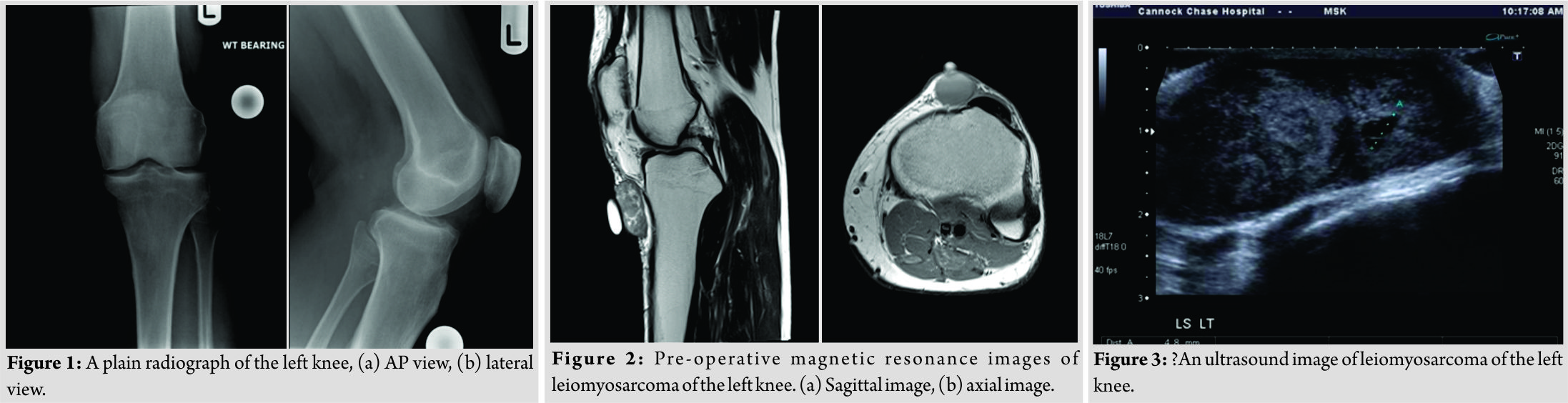 It was low signal on T1 and high signal on T2. No STIR images were performed. The features were otherwise non-specific. An ultrasound was suggested for further information regarding its nature. The ultrasound scan showed a solid/soft tissue looking hypoechoic lesion at the area of interest measuring 3 cm × 1.9 cm ×4.1cm (Fig. 3). A small 5mm cystic component was seen within it. The lesion was highly vascular on Doppler. No obvious connection to the surrounding bone or joint space or blood vessels. The patient was referred to the regional orthopedic oncology service and the differential diagnosis included a soft tissue chondroma, a giant cell tumor of tendon sheath, and a synovial sarcoma. As such, he was consented for a Tru-cut biopsy which was performed in the outpatient department by an orthopedic oncology surgeon. The histological examination showed features compatible with a high-grade leiomyosarcoma (LMS). A computerized tomography scan of his chest performed after biopsy did not show any metastases. A positron emission tomography image was not deemed essential. Furthermore, all his blood investigations were within normal limits. Following discussion at the weekly multidisciplinary meeting, he underwent a formal surgical excision of the lump with marginal margins achieved and he received post-operative radiotherapy. The patient had an uneventful recovery and 18 months postoperatively he remains disease free.
It was low signal on T1 and high signal on T2. No STIR images were performed. The features were otherwise non-specific. An ultrasound was suggested for further information regarding its nature. The ultrasound scan showed a solid/soft tissue looking hypoechoic lesion at the area of interest measuring 3 cm × 1.9 cm ×4.1cm (Fig. 3). A small 5mm cystic component was seen within it. The lesion was highly vascular on Doppler. No obvious connection to the surrounding bone or joint space or blood vessels. The patient was referred to the regional orthopedic oncology service and the differential diagnosis included a soft tissue chondroma, a giant cell tumor of tendon sheath, and a synovial sarcoma. As such, he was consented for a Tru-cut biopsy which was performed in the outpatient department by an orthopedic oncology surgeon. The histological examination showed features compatible with a high-grade leiomyosarcoma (LMS). A computerized tomography scan of his chest performed after biopsy did not show any metastases. A positron emission tomography image was not deemed essential. Furthermore, all his blood investigations were within normal limits. Following discussion at the weekly multidisciplinary meeting, he underwent a formal surgical excision of the lump with marginal margins achieved and he received post-operative radiotherapy. The patient had an uneventful recovery and 18 months postoperatively he remains disease free.
Discussion
LMS is a rare malignant tumor of smooth muscle that often presents in the lower limb. While there are several cases of dermal LMS infiltrating the subcutaneous fat, cases of LMS arising in the subcutaneous fat are rare [2,3]. They originate in the smooth muscle of vessel walls [4, 5]. Superficial LMS (SLMS) can affect any age group although it is exceedingly rare in children. It is slightly more likely to occur in the male population [5]. The general characteristics of most soft tissue sarcomas are that they are painful; they increase in size, are located deep to the superficial fascia, and are relatively large. SLMS-i.e., those that arise in the dermis or subcutaneous tissue -accounts for only 2–3% of all soft tissue sarcomas, with an overall incidence of 0.04% [5]. These tumors, contrary to the general characteristics of most soft tissue sarcomas, are painless and movable by palpation in many cases, and therefore, they are often misdiagnosed as benign tumors such as lipoma, soft tissue chondroma, leiomyoma, fibroma, or a giant cell tumor. Hence, care should be taken to avoid a delay in diagnosis and treatment. However, some patients have reported pain or tenderness on palpationand recent accelerated growth [5]. Diagnosisis normally made following histological investigation, using immunohistochemical stains to prove smooth muscle differentiation [2,5,6]. Prognosis for an SLMS with subcutaneous involvement is poor, as the tumors tend to be high-grade malignancies [5, 7]. Local recurrence occurs in as many as 50–70% of cases, metastases occur in 40–60% of cases, and mortality is as high as 30–40% [5]. Prognostic features with a higher mortality rate include increased size of tumor, a high malignancy grade, extended tumor necrosis, and the American Joint Committee on Cancer staging [6]. Treatment of LMS commonly involves local excision of the tumor with significant clear margins [5, 8, 9]. They do not respond well to either radiation or chemotherapy [10].In our case, post-operative radiotherapy was given as recommended by the multidisciplinary team members because of the marginal resection margins. Long-term clinical follow-up is recommended due to the high potential of local recurrence and metastasis [5].
Conclusion
LMS is a rare smooth muscle malignant tumor. It occasionally presents with features of a benign tumor and can be diagnosed as a lipoma, soft tissue chondroma, leiomyoma, fibroma, or a giant cell tumor. Diagnostic imaging can be inconclusive and definite diagnosis can be made on histological examination. Treatment includes surgical excision and radiotherapy.
Clinical Message
Patients can present to a medical practitioner with a lump having the clinical features of a benign tumor. We advise that after eliminating benign possibilities, medical practitioners must consider the possibility of a soft tissue sarcoma and have a high level of suspicion and a low threshold of conducting further clinical and radiological examinations with subsequent referral to the regional oncology specialist center.
References
1. Park J, Kang C, Kim C, Chae I, Park J. Highly malignant soft tissue sarcoma of the extremity with a delayed diagnosis. World J Surg Oncol 2010;8:84.
2. Jensen M, Jensen O, Michalski W, Nielsen O, Keller J. Intradermal and subcutaneous leiomyosarcoma: A clinic pathological and immune histochemical study of 41 cases. J CutanPathol1996;23:458-63.
3. Massi D, Franchi A, Alos L, Cook M, Di Palma S, Enguita A, et al. Primary cutaneous leiomyosarcoma: Clinicopathological analysis of 36 cases. Histopathology 2010;56:251-62.
4. Altinok G, Dogan AI, Aydin SO, Gedikoglu G. Primary leiomyosarcomas of the skin. Scand J PlastReconstr Surg Hand Surg 2002;36:56.
5. Fauth C, Bruecks A, Temple W, Arlette J, Di Francesco L. Superficial leiomyosarcoma: A clinic pathologic review and update. J CutanPathol2010;37:269-76.
6. Miyajima K, Oda Y, Oshiro Y, Tamiya S, Kinukawa N, Masuda K, et al. Clinicopathological prognostic factors in soft tissue leiomyosarcoma: A multivariate analysis. Histopathology 2002;40:353-9.
7. Spencer JM, Amonette RA. Tumors with smooth muscle differentiation. Dermatol Surg 1996;22:761.
8. Schadendorf D, Haas N, Ostmeier H, Czarnetzki BM. Primary leiomyosarcoma of the skin: A histological and immune histochemical analysis. Acta DermVenereol1993;73:143.
9. Tsutsumida A, Yoshida T, Yamamoto Y, Itoh T, Minakawa H, Sugihara T. Management of superficial leiomyosarcoma: A retrospective study of 10 cases. PlastReconstr Surg 2005;116:8.
10. John T, Portenier D, Auster B, Mehregan D, Drelichman A, Telmos A. Leiomyosarcoma of the scrotum: Case report and review of literature. Urology 2006;67:424.e13.
 |
 |
 |
 |
| Dr. Konstantinos Papageorgiou | Dr. Peter Goodwin | Dr. John Travlos | Dr. Asterios Dramis |
| How to Cite This Article: Papageorgiou K, Goodwin P, Travlos J, Dramis A. Leiomyosarcoma of the Lower Limb Presenting as a Benign Mass: A Case Report. Journal of Orthopaedic Case Reports 2018 Nov-Dec; 8(6): 13-15. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


