
[box type=”bio”] Learning Point of the Article: [/box]
Although rare, concurrent terrible triad injury of the elbow and perilunate wrist dislocation should not be misdiagnosed as a careful examination of polytrauma patients and a promptsurgical treatment may guarantee good functional results.
Case Report | Volume 8 | Issue 6 | JOCR November – December 2018 | Page 38-41 | Ahmed Elloumi, Maamoun Mihoubi, Mohamed Abdelkafi, Mohamed Ali Kedous, Sabri Mahjoub. DOI: 10.13107/jocr.2250-0685.1248
Authors: Ahmed Elloumi[1], Maamoun Mihoubi[1], Mohamed Abdelkafi[1], Mohamed Ali Kedous[1], Sabri Mahjoub[1]
[1]Department of Orthopedic Surgery, Trauma Center, Ben Arous, Tunisia.
Address of Correspondence:
Dr. Ahmed Elloumi,
Department of Orthopedic Surgery, Trauma Center, Ben Arous, Tunisia.
E-mail: docloum@hotmail.com
Abstract
Introduction: Floating forearm is rare. Simultaneous terrible triad injury of the elbow is even rarer.
Case Report: A 47-year-old male patient presented with concurrent dorsal perilunate dislocation of the left wrist combined with a terrible triad injury of the left elbow after a fall from the second floor. The patient had an immediate reduction of the dislocated elbow. Then, a fixation of the radial head by screws, anterior capsule suture, and lateral collateral ligament repair was performed. The wrist dislocation was reduced and fixed with K-wires through a dorsal approach. At 12 months, the patient only complained of moderate pain on heavy lifting and had resumed his work.
Conclusions: A perilunate dislocation of the wrist may occur simultaneously to a terrible triad injury of the elbow at the same side, especially in polytrauma patients. These patients should be examined carefully. An urgent surgical treatment has been successful, while severe damage to the function of the superior limb may result if the diagnosis is missed.
Keywords: Multiple trauma, elbow dislocation, radial head, wrist injuries, ulna fractures.
Introduction
A perilunate dislocation may be misdiagnosed by a medical professional in up to 22% of cases, which would lead to a delay in treatment. In addition to the lack of experience of the physician, concomitant upper-extremity injuries have been found to be a risk factor for missing the initial diagnosis [1]. The term “floating forearm” refers to a rare condition in which concurrent elbow and wrist dislocations occur [2]. When elbow dislocation is associated with radial head and coronoid apophysis fractures, the diagnosis of “terrible triad injury” is made. This association is even rarer, and we found only one case reported in the literature [3]. We describe an unusual case of simultaneous terrible triad injury of the elbow and perilunate wrist dislocation treated immediately with good post-operative results.
Case Report
A 47-year-old male patient fell from the second floor while he was working on a construction site, which led to his left upper limb trauma. The first doctor on the scene diagnosed a dislocation of the left elbow. He practiced a closed reduction as the injury was very painful. The patient was then directed in a medical ambulance to our trauma center. On his arrival at the emergency room, the patient was conscious and had no respiratory distress. His vital signs were stable. He was unable to move his left upper limb due to intense pain. The left elbow was swollen. The forearm seemed shortened. Distal pulses, fingers motility, and sensitivity were normal. Radiographs showed a reduced elbow with a displaced fracture of the radial head (Fig. 1) and a dorsal perilunate dislocation of the wrist (Fig. 2). Computed tomography scan showed Mason type 2 radial head fracture associated with Regan and Morrey type 1 coronoid apophysis fracture (Fig. 3).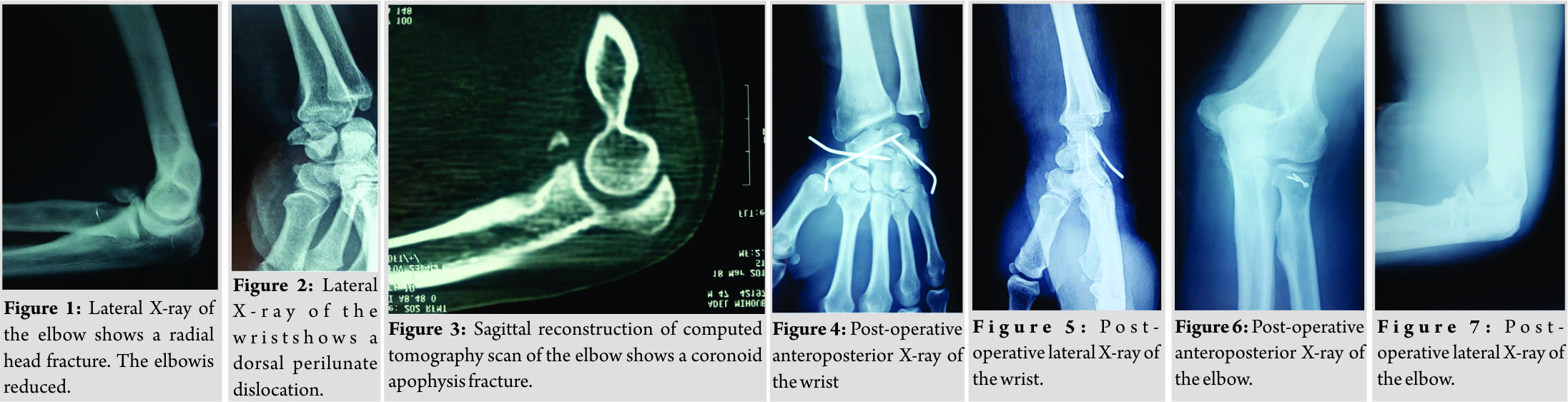 There were no carpal bone fractures. The diagnosis of floating forearm with terrible triad injury of the elbow was assessed. Then, the patient underwent primary surgical treatment on the same day. As closed manipulation did not succeed, an open reduction of the wrist was performed through a dorsal approach. Then, the reduction was fixed by the mean of three K-wires. The first K-wire passed from the scaphoid into the lunatum, the second from the scaphoid into the capitatum, and the third from the triquetrum into the lunatum (Fig. 4 and 5). The scapholunate and triquetrolunate ligaments were ruptured. They were primarily repaired. Then, a lateral approach to the elbow was performed, the radial head was reduced and fixed with screws, the capsule was tied through drill holes, and the lateral collateral ligament was repaired with transosseous sutures (Fig. 6 and 7). The elbow was stable when testing. An elbow immobilization using a cast at a joint angle of 90° was maintained for 3weeks. It was followed by a below-elbow cast for 3 other weeks. Elbow rehabilitation started in the 3rdpost-operative week. Shoulder mobilization and active-assisted flexion/extension of the elbow were performed 2times a week to reestablish non-painful range of motion and to prevent muscular atrophy. In the 6thweek, casting and K-wires were completely removed and rehabilitation of the patient’s wrist began. Resisting active exercises and handgrip training were introduced gradually, which helped to reduce pain and edema. Then, range of motion activities was performed for all planes of the elbow and the wrist. The patient was motivated to accomplish further home exercises. He was followed up regularly. There has been no septic complication or wound dehiscence. At 12-month follow-up, the patient only complained of moderate pain on heavy lifting and had resumed his job as a construction worker. At 18 months, the extension of the left elbow was limited at 10° while flexion was limited at 110°. The palmar and dorsal flexion of the wrist was each 70° (Fig. 8, 9, 10, and 11). The grip strength was 75% of the contralateral side. It was measured using a hand dynamometer. The disability of the arm, shoulder, and hand score was 20, which assessed mild impairment and good functional outcome.
There were no carpal bone fractures. The diagnosis of floating forearm with terrible triad injury of the elbow was assessed. Then, the patient underwent primary surgical treatment on the same day. As closed manipulation did not succeed, an open reduction of the wrist was performed through a dorsal approach. Then, the reduction was fixed by the mean of three K-wires. The first K-wire passed from the scaphoid into the lunatum, the second from the scaphoid into the capitatum, and the third from the triquetrum into the lunatum (Fig. 4 and 5). The scapholunate and triquetrolunate ligaments were ruptured. They were primarily repaired. Then, a lateral approach to the elbow was performed, the radial head was reduced and fixed with screws, the capsule was tied through drill holes, and the lateral collateral ligament was repaired with transosseous sutures (Fig. 6 and 7). The elbow was stable when testing. An elbow immobilization using a cast at a joint angle of 90° was maintained for 3weeks. It was followed by a below-elbow cast for 3 other weeks. Elbow rehabilitation started in the 3rdpost-operative week. Shoulder mobilization and active-assisted flexion/extension of the elbow were performed 2times a week to reestablish non-painful range of motion and to prevent muscular atrophy. In the 6thweek, casting and K-wires were completely removed and rehabilitation of the patient’s wrist began. Resisting active exercises and handgrip training were introduced gradually, which helped to reduce pain and edema. Then, range of motion activities was performed for all planes of the elbow and the wrist. The patient was motivated to accomplish further home exercises. He was followed up regularly. There has been no septic complication or wound dehiscence. At 12-month follow-up, the patient only complained of moderate pain on heavy lifting and had resumed his job as a construction worker. At 18 months, the extension of the left elbow was limited at 10° while flexion was limited at 110°. The palmar and dorsal flexion of the wrist was each 70° (Fig. 8, 9, 10, and 11). The grip strength was 75% of the contralateral side. It was measured using a hand dynamometer. The disability of the arm, shoulder, and hand score was 20, which assessed mild impairment and good functional outcome.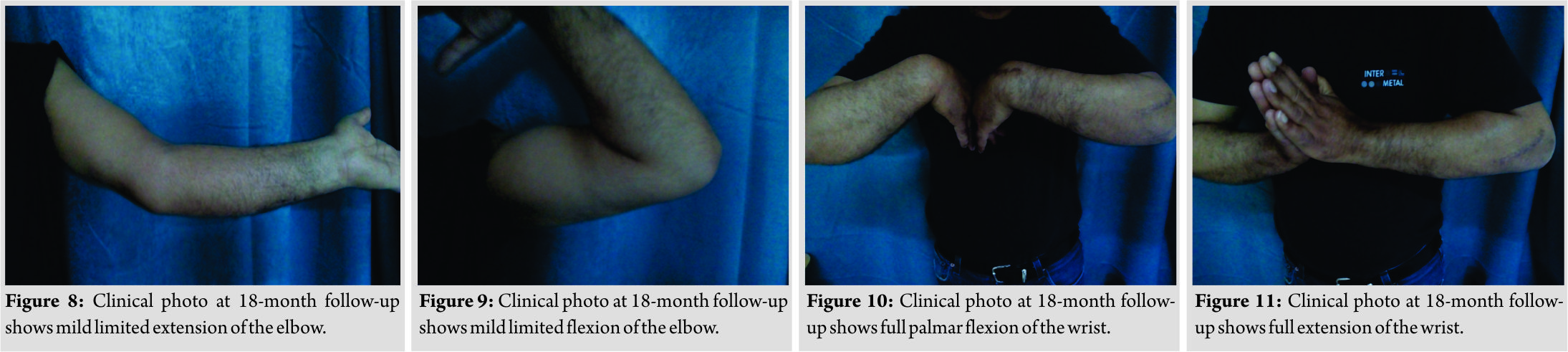
Discussion
There is only one case of concurrent terrible triad injury of the elbow and perilunate dislocation of the wrist reported by Reddy, in 2016 [3]. Otherwise, there are few reports of simultaneous elbow and wrist dislocations. We found only 12 cases of floating forearm in the literature. The term “floating forearm” was used by Prasad, in 2007, to describe a concomitant ipsilateral elbow and perilunate dislocation in a 30-year-old man who fell from a tree after alcoholic intoxication [2]. Three similar cases were reported previously by Chen, in 1994. They all fell from motorcycle [4]. Data from the other reports are shown in Table 1. All patients were male. Their age ranged from 22 to 56 years old. High-energy trauma was described in all reports: Fall from a considerable height in seven cases or motor vehicle accident in five cases (Table 1) [5, 6, 7, 8, 9, 10]. The rate of missed diagnosis of perilunate dislocations can be as high as 25% [5]. In one of the three cases reported by Chen, delay in diagnosis of perilunate dislocation necessitated proximal row carpectomy at 6weeks [4]. There is no recommended treatment algorithm for floating forearm. Closed reduction maneuvers of the wrist may be successful after 10 min of manual traction [11]. External fixation may facilitate indirect reduction of the wrist by means of ligamentotaxis. However, poor functional results have been reported with this technique. Thus, the main indication of ligamentotaxis is polytrauma patients with associated ipsilateral extremity fractures, when swelling causes concern about placing the wrist in a cast, or old neglected unreduced perilunate dislocations [12]. In all other cases, early surgical treatment and open reduction seem to be the most appropriate option for the wrist. Actually, a good functional outcome depends on the proper alignment of carpal bones and the timing of surgery [5,11]. The dorsal approach has been used in seven cases of floating forearm and in our case (Table 1). This approach is sufficient for accurate reduction of bony displacement and removal of soft tissue interposition [5,11]. Acute ligamentous injuries should be repaired if there are no degenerative changes. If there is sufficient ligamentous tissue, as in our case, primary repair may be achieved by suturing at least the dorsal scapholunate ligament. Otherwise, suture anchors may be used [5, 11]. Conservative treatment has been often preferred for the elbow [4, 5, 13]. However, open reduction was needed in a case of floating forearm with divergent dislocation of the elbow [7]. Coronoid apophysis and humeroradial wiring were performed in other cases [9, 10]. In the case reported by Reddy, a posterior approach was performed, the radial head was replaced, the capsule-osseous complex was sutured and the medial collateral ligament was repaired [3]. In our case, the radial head was fixed with screws. The elbow was stable after tying the capsule and repairing the lateral collateral ligament. Post-operative rehabilitation should begin as soon as possible. There are no sufficient data describing its modalities in the literature. In our case, it started at 3weeks for the elbow and at 6weeks for the wrist. Early and appropriate surgical treatment of both terrible triad injury of the elbow and perilunate dislocation of the wrist leads to good functional outcomes [11,14]. However, several complications have been reported such as superficial infection and ulnar nerve neuropraxia. The decrease in range of motion of the elbow may be well tolerated by the patients as it does not impede their daily activities [14]. In our case, no post-operative complication has been detected. Functional outcomes were good at 18-month follow-up.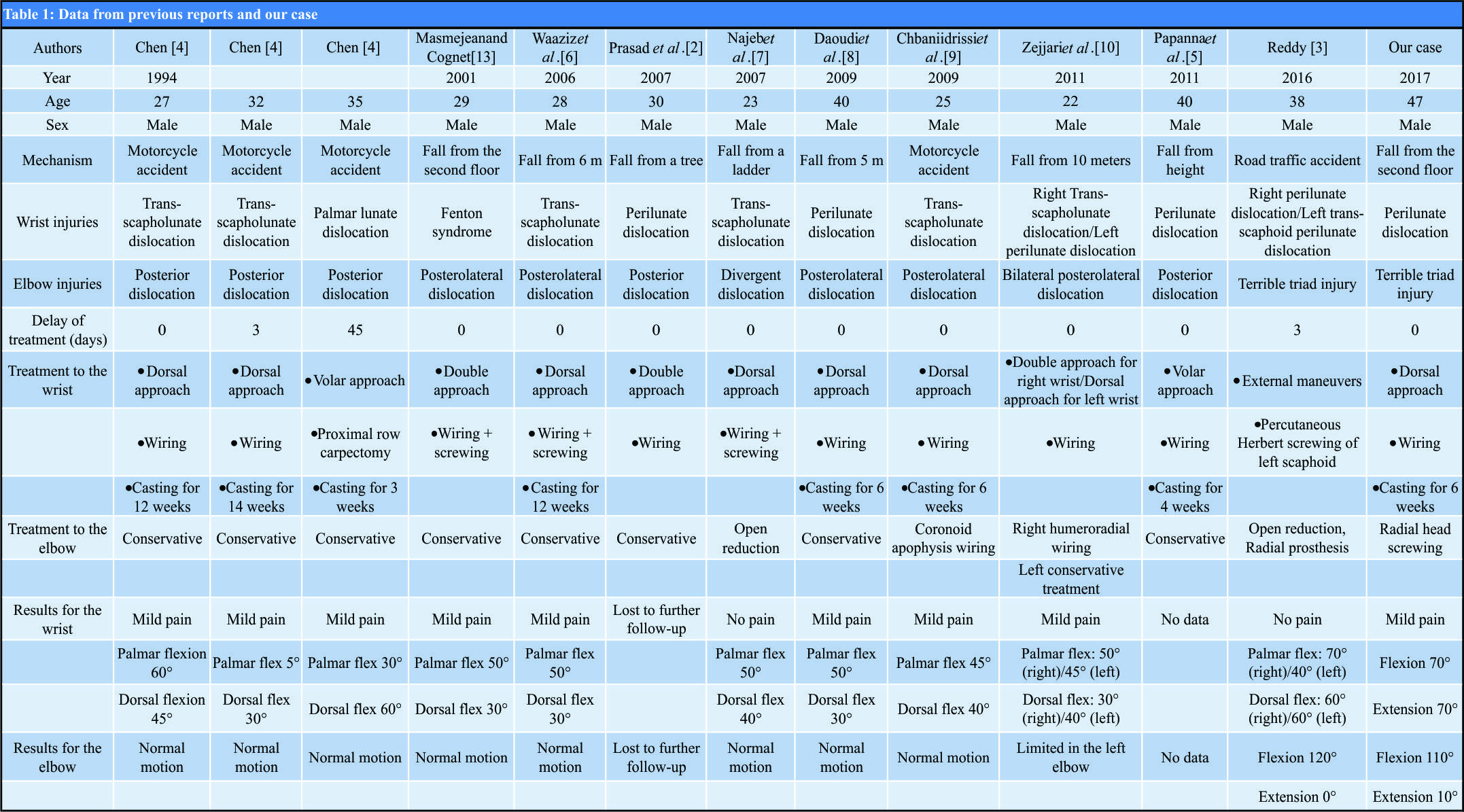
Conclusion
In case of high-energy trauma, missing a diagnosis of perilunate dislocation or terrible triad injury of the elbow may lead to a disastrous functional outcome. A thorough examination is mandatory. Only urgent surgical treatment of both elbow and wrist may achieve good results. In our case, the patient recovered a nearly normal function of his left upper limb.
Clinical Message
A careful examination of multi-injured patients is imperative. Detecting a single lesion may lead to missing the diagnosis of others and result in serious functional damage.
References
1. Çolak I, Bekler HI, Bulut G, Eceviz E, Gülabi D, Çeçen GS. Lack of experience is a significant factor in the missed diagnosis of perilunate fracture dislocation or isolated dislocation. Acta OrthopTraumatol Turcica 2018;52:32-6.
2. Prasad K, Dayanandam B, Gakhar H, Attarwala U, Karras K. Concomitant elbow and perilunate dislocation: Floating forearm. Internet J Orthop Surg 2008;8:1-4.
3. Reddy JM. Traumatic bilateral terrible triad of elbow with left trans-scaphoid perilunate dislocation and right lunate dislocation. Int J Curr Res 2016;8:35255-8.
4. Chen WS. Concurrent perilunate dislocation in patients with elbow dislocation: Three case reports. J Trauma 1994;37:504-7.
5. Papanna MC, Al-Hadithy N, Sarkar JS. Concurrent palmar lunate dislocation and posterior elbow dislocation: A case report. J Orthop Surg 2011;19:367-9.
6. Waaziz A, Moujtahid M, Bendriss A. The floating forearm: elbow and perilunate dislocation. Chirg Main 2006;25:54-7.
7. Najeb Y, Essadki B, Latifi M, Fikry T. Bipolar dislocation of the forearm. Chir Main 2007;26:62-4.
8. Daoudi A, Elibrahimi A, Loudiyi WD, Elmrini A, Chakour K, Batayeb F. Floating forearm: Elbow and wrist dislocation. Chir Main 2009;28:53-6.
9. Chbaniidrissi B, Amar MF, Loudyi D, Marzouki D, Boutayeb F. Avant bras flottant (à propos d’un cas). J Traumatol Sport 2009;26:240-2.
10. Zejjari H, Louaste J, Chkoura M, Rachid K. Avant-bras flottant bilatéral: A propos d’un cas. Chir Main 2011;30:155-8.
11. Firth GB, Aden A. Treatment of lunate and perilunate dislocations with a combined approach and anchor repair of the dorsal scapholunate interosseous ligament. SA Orthop J 2008;7:32-8.
12. Savvidou OD, Beltsios M, Sakellariou VI, Papagelopoulos PJ. Perilunate dislocations treated with external fixation and percutaneous pinning. J Wrist Surg 2015;4:76-80.
13. Masmejean E, Cognet JM. Bipolar dislocation of the forearm: Elbow and perilunate dislocation. Rev ChirOrthopReparatrice 2001;87(5):499-5O2.
14. Brigato RM, Mouraria GG, Kikuta FK, Coelho SP, Cruz MA, Filho AZ. Functional Evaluation of patients with surgically treated terrible triad of the elbow. Acta Ortop Bras 2015;23:138-41.
 |
 |
 |
 |
 |
| Dr. Ahmed Elloumi | Dr. Maamoun Mihoubi | Dr. Mohamed Abdelkafi | Dr. Mohamed Ali Kedous | Dr. Sabri Mahjoub |
| How to Cite This Article: Elloumi A, Mihoubi M, Abdelkafi M, Kedous MA, Mahjoub S. Floating Forearm with Terrible Triad Injury of the Elbow: A Case Report. Journal of Orthopaedic Case Reports 2018 Nov-Dec; 8(6): 38-41. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


