
[box type=”bio”] Learning Point of the Article: [/box]
Beware of this unusual, novel complication when using cemented metal-backed dual mobility acetabular sockets in THA.
Case Report | Volume 8 | Issue 6 | JOCR November – December 2018 | Page 46-49 | Rakesh John, Anuj Jain, Shekhar Agarwal, Simon Thomas, Sunny Agarwal. DOI: 10.13107/jocr.2250-0685.1252
Authors: Rakesh John[1], Anuj Jain[1], Shekhar Agarwal[1], Simon Thomas[1], Sunny Agarwal[1]
[1]Department of Orthopaedics, Sant Parmanand Hospital, Civil Lines, New Delhi, India.
Address of Correspondence:
Dr. Rakesh John,
Department of Orthopaedics,Delhi Institute of Trauma and Orthopaedics, Sant Parmanand Hospital, New Delhi – 110054, India.
E-mail: rakeshjohn23@gmail.com
Abstract
Introduction: Acute complete dissociation of a cemented socket from the acetabular cavity is very rare and has been described only in relation to closed reduction maneuver of a dislocated hip arthroplasty.
Case Report: We present a case of recurrent hip dislocation in a 70-year-old female post total hip arthroplasty for which a cemented dual mobility (DM) component was used. The cemented socket dissociated from the acetabular cavity with the polyethylene liner insitu1-year post-surgery. It was not related to intraprosthetic dislocation as the acetabular liner-socket interface was not disrupted. A re-revision of the acetabular component was done with an acetabular reinforcement cage, cemented cup, and constraint acetabular liner. No such case of cup dissociation has been reported in the literature till date.
Conclusion: The use of cemented DM cups without acetabular reinforcement devices has been described recently and is still controversial. Surgeons should be aware of the possibility of such a complication when using metal-backed cemented DM cups.
Keywords: Dislocation, dissociation, dual mobility, hip arthroplasty.
Introduction
Dislocation is the most common reason for revision after total hip arthroplasty (THA) after both primary and revision surgeries [1]. Farizon et al. [2] developed the dual mobility (DM) socket in 1974 to increase the stability of the THA implant. Due to the dual articulation, larger jump distance and the greater range of motion before impingement, the rate of dislocation is significantly reduced with a DM cup [3, 4]. The use of a DM hip in a revision surgery for THA instability is an attractive option as the rate of dislocation after revision arthroplasty is higher compared to primary THA [3]. DM implants are increasingly being used in cases with high risk of post-operative instability. However, the DM cup has its own set of complications such as intraprosthetic dislocation (IPD) and accelerated wear of liner. [3, 5] Furthermore, the use of cemented DM cups is relatively new and controversial [6, 7]. In this case report, we present a case where a metal-backed, cemented DM socket was used to revise an uncemented THA with recurrent instability and the entire socket, along with the polyethylene (PE) liner insitu, dissociated from the acetabulum 1year later. Such a complication is unusual and has not been reported in the literature till date.
Case Report
A 70-year-old female, known case of rheumatoid arthritis underwent elective, uncemented THA of the left hip in 2015 for severe destructive arthropathy through the posterolateral approach (Fig. 1). She sustained three episodes of dislocation at 2, 3, and 5 weeks post-surgery secondary to acetabular component malpositioning. A revision of the acetabulum component was performed after the third episode of dislocation and a cemented DM socket (Cotyle double mobilite, Evolutis, Briennon, France) was implanted using standard operative technique (Fig. 2). Following this revision surgery, the patient was asymptomatic for the next 1year when she sustained a trivial fall in the bathroom. She was unable to bear weight at presentation. Plain radiograph revealed a completely dissociated acetabular socket lying outside the acetabulum (Fig. 3). She was taken up for re-revision surgery. The DM socket had reposed back into the acetabulum on surgical exposure and was completely loose (Fig. 4).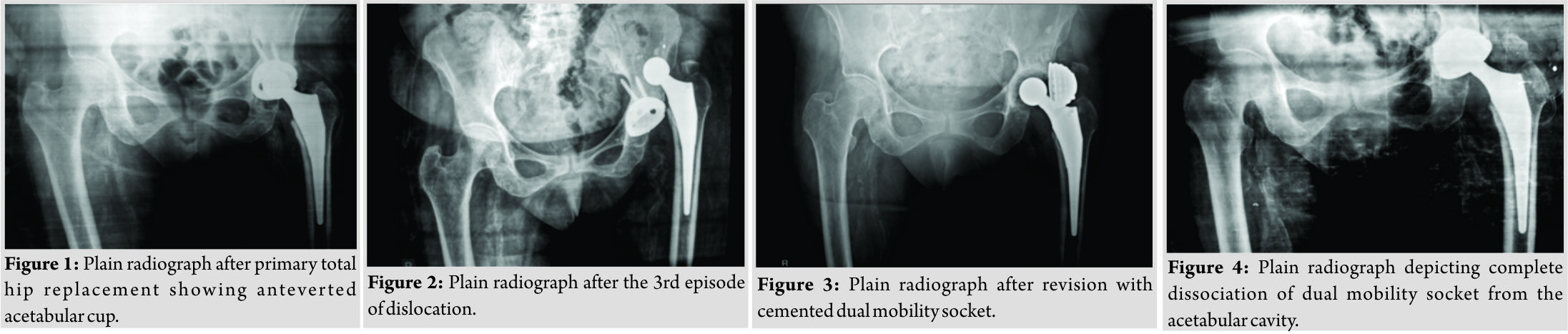 The socket was extracted with the liner insitu (Fig. 5). An acetabular reinforcement cage (Burch-Schneider™ reinforcement cage; Zimmer, Warsaw, IN) along with a cemented socket and constraint acetabular liner (ZCA®; Zimmer, Warsaw, IN) was implanted with a 28 mm head (Fig. 7). At the latest follow-up (1year), the patient was mobile, asymptomatic and had no further episodes of instability.
The socket was extracted with the liner insitu (Fig. 5). An acetabular reinforcement cage (Burch-Schneider™ reinforcement cage; Zimmer, Warsaw, IN) along with a cemented socket and constraint acetabular liner (ZCA®; Zimmer, Warsaw, IN) was implanted with a 28 mm head (Fig. 7). At the latest follow-up (1year), the patient was mobile, asymptomatic and had no further episodes of instability.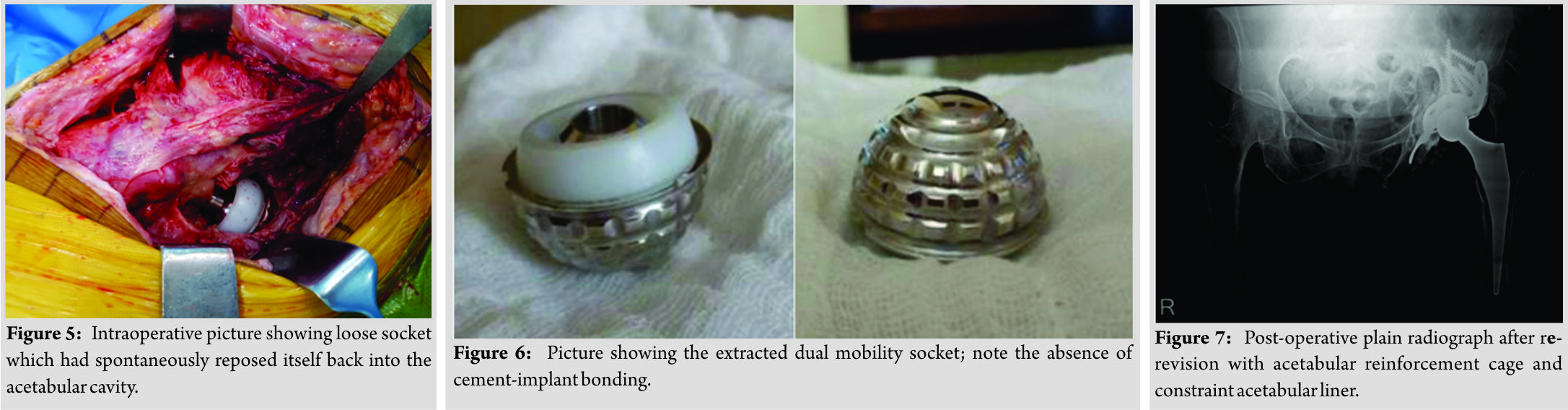
Discussion
Dissociation of the cemented socket or cemented stem after THA is an extremely rare complication and has been only reported during closed reduction maneuvers in an already dislocated total hip replacement. Dissociation of cemented femur stems from the femoral canal during closed reduction has been described multiple times in the literature [8, 9, 10, 11, 12, 13, 14]. However, dissociation of the cemented acetabular socket is very unusual. Tamura et al. [15] reported the first case of a cemented cup dissociation which occurred during the closed reduction of a dislocated THA. This dissociation of the cup was secondary to fractured ceramic screws which were used to secure bone graft which was used to fill defects superior to the acetabulum. However, the cup was not completely displaced from its position like in our case. After a careful search of the literature, we could not find any other published case report/series where a complete dissociation of the cemented acetabular cup has been described. Furthermore, no such case has been reported in any series involving follow-up of metal-backed, cemented DM cups. DM sockets have demonstrated a reduced dislocation rate in revision hip arthroplasty and also in recurrent THA instability [4, 16, 17, 18, 19]. Although the dislocation rate is reduced considerably with the use of DM sockets, it is associated with a unique and troublesome complication – IPD [4, 5, 20]. Here, the mobile PE liner dissociates from the socket and is displaced, whereas the femoral head continues to articulate with the acetabular socket. Philippot et al. [5] reported the largest series of IPD and devised a classification system for the same. Type III IPD is associated with cup loosening. In the case, we have reported, the liner was not dissociated from the acetabular socket, therefore, ruling out IPD. The most important reason for dissociation, in this case, is the weak bonding between the cement and the metal-backed socket. The use of cemented DM cups has been controversial. Cemented DM sockets were initially developed to be used in conjunction with acetabular reinforcement cages in cases with deficient acetabular bone stock [6]. The use of cemented DM cups without reinforcement devices has only been described recently. Many studies have advised against the use of cemented DM cups without reinforcement devices for the fear of increased risk of acetabular component loosening [6, 21, 22]. On the other hand, few recent midterm outcome studies have demonstrated good results where a cemented DM socket has been used without acetabular reinforcement devices in revision THA for post-THA instability [7,16,19].
Conclusion
To summarize, although DM sockets reduce the dislocation rates in recurrent THA instability, uncemented DM sockets should be preferred over cemented sockets. Surgeons should be aware of the possibility of dissociation of the acetabular component with the use of a metal-backed cemented acetabular cup without a reinforcement device.
Clinical Message
Metal-backed cemented DM acetabular components can be associated with complete cup dissociation; uncemented DM cups should be preferred over metal-backed cemented acetabular components.
References
1. Bozic KJ, Kurtz SM, Lau E, Ong K, Vail TP, Berry DJ, et al. The epidemiology of revision total hip arthroplasty in the United States. J Bone Joint Surg Am 2009;91:128-33.
2. Farizon F, de Lavison R, Azoulai JJ, Bousquet G. Results with a cementless alumina-coated cup with dual mobility. A twelve-year follow-up study. Int Orthop1998;22:219-24.
3. Plummer DR, Haughom BD, Della Valle CJ. Dual mobility in total hip arthroplasty. Orthop Clin North Am 2014;45:1-8.
4. De Martino I, D’Apolito R, Soranoglou VG, Poultsides LA, Sculco PK, Sculco TP, et al. Dislocation following total hip arthroplasty using dual mobility acetabular components: A systematic review. Bone Joint J 2017;99-B:18-24.
5. Philippot R, Boyer B, Farizon F. Intraprosthetic dislocation: A specific complication of the dual-mobility system. Clin OrthopRelat Res 2013;471:965-70.
6. Wegrzyn J, Pibarot V, Jacquel A, Carret JP, Béjui-Hugues J, Guyen O, et al. Acetabular reconstruction using a Kerboull cross-plate, structural allograft and cemented dual-mobility cup in revision THA at a minimum 5-year follow-up. J Arthroplasty 2014;29:432-7.
7. Haen TX, Lonjon G, Vandenbussche E. Can cemented dual-mobility cups be used without a reinforcement device in cases of mild acetabular bone stock alteration in total hip arthroplasty? OrthopTraumatol Surg Res 2015;101:923-7.
8. Ng Man Sun S, Gillott E, Davies N, Skinner J. Displacement of a cemented femoral implant. A complication of manipulation of a dislocated total hip replacement. BMJ Case Rep 2012;2012: pii: bcr2012006821.
9. Pai VS. Dislocation of a polished femoral stem following a cemented total hip arthroplasty: A report of 2 cases. J Orthop Surg (Hong Kong) 2005;13:73-5.
10. Holt MD. Prosthesis displacement as a complication of reduction of a dislocated total hip arthroplasty. J Arthroplasty 1996;11:979-80.
11. Haq RU, Park KS, Yang HK, Lee KB, Yoon TR. Displacement of a cemented femoral stem during attempted closed reduction of a dislocated total hip arthroplasty. J Arthroplasty 2010;25:658.e11-5.
12. Petracchi M, Della Valle AG, Buttaro M, Piccaluga F. Displacement of a cemented polished tapered stem during closed reduction of a dislocated total hip arthroplasty-a case report. Acta OrthopScand2002;73:475-7.
13. Staal HM, Heyligers IC, van der Sluijs JA. Stem displacement during reduction of a dislocated cemented total hip arthroplasty with a polished tapered stem. J Arthroplasty 2000;15:944-6.
14. Volpin G, Grimberg B, Daniel M. Complete displacement of the femoral stem during dislocation of a THR. J Bone Joint Surg Br 1997;79:616-7.
15. Tamura J, Kawanabe K, Shimizu M, Kimura G, Nakamura T. Displacement of a cemented socket after reduction of a dislocated total hip arthroplasty. J Arthroplasty 2004;19:240-3.
16. Hamadouche M, Ropars M, Rodaix C, Musset T, Gaucher F, Biau D, et al. Five to thirteen year results of a cemented dual mobility socket to treat recurrent dislocation. Int Orthop2017;41:513-9.
17. Guyen O, Pibarot V, Vaz G, Chevillotte C, Béjui-Hugues J. Use of a dual mobility socket to manage total hip arthroplasty instability. Clin OrthopRelat Res 2009;467:465-72.
18. Leclercq S, el Blidi S, Aubriot JH. Bousquet’s device in the treatment of recurrent dislocation of a total hip prosthesis. Apropos of 13 cases. Rev ChirOrthopReparatriceAppar Mot 1995;81:389-94.
19. Langlais FL, Ropars M, Gaucher F, Musset T, Chaix O. Dual mobility cemented cups have low dislocation rates in THA revisions. Clin OrthopRelat Res 2008;466:389-95.
20. Star MJ, Colwell CW Jr. Donaldson WF 3rd, Walker RH. Dissociation of modular hip arthroplasty components after dislocation. A report of three cases at differing dissociation levels. Clin OrthopRelat Res 1992;278:111-5.
21. Girard J, Herent S, Combes A, Pinoit Y, Soenen M, Laffargue P, et al. Metal-on-metal hip replacement using metasul cups cemented into muller reinforcement rings after a mean 5-year (3-8) follow-up: Improvement of acetabular fixation by comparing with direct cementation to bone. Rev ChirOrthopReparatriceAppar Mot 2008;94:346-53.
22. Ebramzadeh E, Beaulé PE, Culwell JL, Amstutz HC. Fixation strength of an all-metal acetabular component cemented into an acetabular shell: A biomechanical analysis. J Arthroplasty 2004;19:45-9.
 |
 |
 |
 |
 |
| Dr. Rakesh John | Dr. Anuj Jain | Dr. Shekhar Agarwal | Dr. Simon Thomas | Dr. Sunny Agarwal |
| How to Cite This Article: John R, Jain A, Agarwal S, Thomas S, Agarwal S. Dissociation of Cemented Dual Mobility Socket from the Acetabulum in a Case of Recurrent Total Hip Arthroplasty Instability -A Novel Complication. Journal of Orthopaedic Case Reports 2018 Nov-Dec; 8(6): 46-49. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


