
[box type=”bio”] Learning Point of the Article: [/box]
Management guidelines: Functional need is of higher priority than the anatomical correction when a case of Mirror foot with trapezoidal dysplastic tibia presents at adolescent age.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 26-29 | Pabitra Kumar Sahoo, Mamata Manjari Sahu. DOI: 10.13107/jocr.2019.v09.i04.1464
Authors: Pabitra Kumar Sahoo[1], Mamata Manjari Sahu[2]
[1]Department of Physical Medicine and Rehabilitation, Swami Vivekanand National Institute of Rehabilitation Training and Research, Cuttack, Odisha, India,
[2]Department of Physiotherapy, Swami Vivekanand National Institute of Rehabilitation Training and Research, Cuttack, Odisha, India.
Address of Correspondence:
Dr. Pabitra Kumar Sahoo,
Department of Physical Medicine and Rehabilitation, Swami Vivekanand National Institute of Rehabilitation Training and Research(SVNIRTAR),
Olatpur, Bairoi, Cuttack-754010, Odisha, India.
E-mail: pabitra2406@gmail.com
Abstract
Introduction: Pre-axial foot polydactyly has been termed as mirror foot, otherwise known as diplopodia. Association of a hypoplastic trapezoid shaped tibia makes the condition extremely uncommon. Whatever limited literature is available, most of it is focused on the preliminary reconstruction of deformity which again may not be feasible in late presentation.
Case report: We present a 17-year-old girl having mirror foot with dysplastic trapezoid shaped tibia. She had mild equinovarus deformity of the right foot with three pre-axial extra digits that represent a mirror foot. There was also a gross shortening of the right leg with 20° fixed flexion deformity of the knee, but she could walk around with limited disability. Her chief complaint was difficulty in outdoor ambulation and poor cosmesis of the foot. Limb reconstruction may not have a predictable outcome with so much of shortening and she was also reluctant for amputation. A course of therapy was given with a treatment objective of improvement of knee flexion deformity and quadriceps control. She was fitted with an extension prosthesis which accommodates the deformed foot and also corrected the limb length discrepancy.
Conclusion: Mirror foot with dysplastic tibia reported at an adolescent age may not be benefited from surgical reconstruction. Functional rehabilitation is better than an anatomic correction in case of late presentation.
Keywords: Mirror foot, polydactyly, dysplastic tibia, rehabilitation.
Introduction
Mirror foot or diplopodia is a rare congenital anomaly with pre-axial mirror polydactyly of the foot. It may occur as an isolated deformity[1] or as a part of the syndrome with multiple congenital anomalies. However, it is commonly associated with a developmental anomaly of the leg such as tibial aplasia or dysplasia and fibular dimelia. Foot deformity in these situations receives least attention and is usually overshadowed by the major long bone anomaly. Most authors prefer amputation of the affected leg on account of severe anomaly and unpredicted surgical outcomes [2]. There is no strict definition of mirror foot. For the diagnosis of mirror foot, there has to be a mirror image polydactyly on the medial side of the foot. There is no universal agreement on what constitutes a mirror foot. Some authors believe that the mirror foot is a foot with mirror-image polydactyly, whereas others considered that mirror duplication of all the skeletal elements of the foot must present on the tibial aspect [3]. There are authors who also suggest that feet with supernumerary rays situated pre-axially, but with the characteristic of post-axial toes can be considered as mirror feet [4].
Most of the cases report in the neonatal period or early childhood for treatment. We here present a case of pre-axial polydactyly with trapezoid dysplastic tibia reported at an adolescent age. We put forward this case for its rarity, unusual late presentation and rehabilitation management.
Case Report
A 17-year-old girl was presented to our rehabilitation institute, having pre-axial polydactyly of the right foot with eight toes and gross shortening of the leg (Fig.1). She was the eldest child of her family and had two younger brothers without having any anomaly. Obstetric history of the mother revealed no previous history of abortion. She was born from a full-term pregnancy with vaginal delivery at home. There was no history of consanguineous marriage in the family. She belonged to the low socioeconomic group. She was evaluated by the nearby tertiary medical center at 1 year age where amputation was suggested. Her parent denied amputation fearing social stigma. They reported to our rehab institute for any alternate management when the girl was rejected repeatedly for her marriage proposals. On examination, she was found to have normal mental and physical milestones except that she had started walking late. Of her polydactyly right foot, the pre-axial three digits were similar to her lateral three toes. The foot was broader compared to the opposite side (Fig. 2). The ankle and foot were in mild equinus and significant varus to an extent that she was walking on varus foot. The varus deformity was predominantly at the ankle joint than the subtalar joint. There was a gross shortening of the leg with 20° fixed flexion deformity of knee. Further, flexion up to 110° was possible. The fibular head was palpable proximal to the knee joint. She had mediolateral instability with varus thrust at the knee during walking with a short limb gait. The power around knee was Grade3, just manageable for walking. There was no sensory-motor deficit. The femur, pelvis, and spine were normal. On radiological evaluation, tibia was very short, trapezoidal shaped, fibula hypertrophied, bowed, and proximally extended above the knee joint (Fig. 3). There were seven metatarsals in the foot with a delta phalanx at medial most toe. Talar dome was concave shaped. There was no duplication of talus or calcaneus. The lateral column of foot appeared longer, which could be due to associated varus deformity. Parents, as well as the patient, were counseled about the plan of management. As the patient was managing indoor ambulation with a minimal disability, parents were not prepared for amputation. There was severe limb length discrepancy where lengthening or reconstruction had a limited role. Despite a gross dysplastic limb, she was able to bear weight on the affected limb. As she belonged to a low socioeconomic family, her nature of work would be limited around the home. Keeping her education, occupation in view, it was decided to fabricate a specially designed extension prosthesis (Fig. 4), which would remain under dress cover. She was fitted with an extension prosthesis. After gait training, she was comfortable with the outdoor ambulation.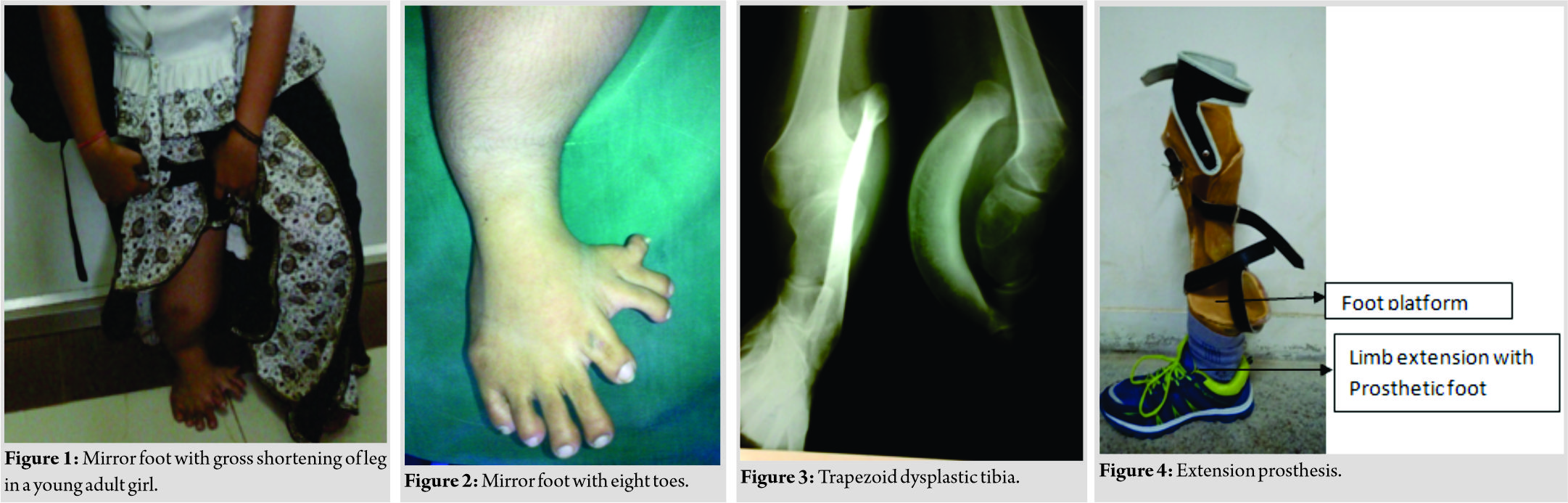
Discussion
The morphological term mirror foot or diplopodia is not sufficient enough to describe the embryological defect. The supernumerary toes in diplopodia may not be the mirror duplication as described by Hamanishi et al. [5] Hence, feet with supernumerary rays situated pre-axially, i.e., medial to the first ray, but with the characteristic of post-axial toes were considered as pre-axial mirror feet [4]. Mirror feet associated with dysplastic tibia are much rarer entity. Genetically, polydactyly is associated with 39 genetic mutations. A number of genetic loci have been identified that are responsible for human polydactyly phenotypes. Genes such as GL13 andSonic Hedgehog SHH protein have been related to polydactyly. Mutation in SHH gene is responsible for mirror image digits [6]. In our case, none of the family members including both paternal and maternal side had any history of limb anomaly. The pattern of skeletal anomalies with pre-axial polydactyly was studied in detail by Verghese et al [4]. They classified their series of mirror polydactyly into four categories; Type 1– mirror polydactyly with fibular dimelia, Type II– associated with tibial aplasia, Type III– mirror polydactyly with the trapezoidal tibia, and Type IV– association with the hypoplastic tibia. In their series, all the three cases with trapezoidal dysplastic tibia were presented with duplication of talus. A retrospective study by Bjoseph [7] on congenital anomalies of tibia had shown similar result where cases of dysplastic trapezoidal tibia were associated with duplication of talus and mirror foot anomaly. There was no duplication of talus in our case; rather, the talar dome was concaved. Fukazawa et al. [8] had reviewed literature and studied the case presented by different authors including three of their own case on mirror hand and mirror feet and tried to classify the mirror feet into six types. Our case of mirror foot with trapezoid tibia is not coming under any of the six categories. Karchinov [3] first noted a dysplastic trapezoidal tibia with pre-axial mirror foot anomaly and accessory foot bones. They treated the leg with amputation. Kadir et al. [9] had a case with a similar presentation which they treated with amputation. However, surgical reconstruction can be tried in a selective condition of this type of cases where there are no gross limb length discrepancy and fair quadriceps function, and foot and ankle deformities are not much severe as described by Deshmukh and Shyam [10]. Sahdi et al. [11] successfully reconstructed the mirror foot of a pre-walking age child to a cosmetically and functionally acceptable foot. Overall result was satisfactory as both the tibia and fibula of the affected limb were apparently normal. Jose et al. [12] suggested that when mirror foot coexists with tibial deficiency that is not amenable to reconstruction through lengthening, the next best option would be below knee or Syme’s amputation. Here,the early correction of the foot by excising the accessory toes would be an exercise in futility. In our case, although there was gross shortening, the parents were reluctant for amputation as the patient had comfortable indoor ambulation without much difficulty.
Conclusion
Treatment of mirror foot as described by various authors in literature may not be applicable to all age groups. On late presentation at an adolescent age, the functional need of the patient is of higher priority than the anatomical correction. If the patient can bear weight on the deformed limb, an extension prosthesis probably would be the best choice for community ambulation and vocational rehabilitation. Preservation of the deformed foot helps in indoor ambulation and provides proprioception for prosthetic function.
Clinical Message
Mirror feet associated with dysplastic tibia are an extremely rare entity and so its management. Most of the published literature suggest early below knee or Syme’s amputation, except for a few who choose surgical limb reconstruction as the treatment of choice. So far, literature is silent about the management of such a condition presented at adolescent or adult age where amputation becomes a social and cultural issue. Functional need of the patient is of more priority above the anatomical correction. An extension prosthesis probably would be the best choice for community ambulation and vocational rehabilitation.
References
1. Al-Qattan MM, Hashem FK, Al Malaq A. An unusual case of preaxial polydactyly of the hands and feet: A case report. J Hand Surg Am 2002;27:498-502.
2. Narang IC, Mysorekar VR, Mathur BP. Diplopodia with double fibula and agenesis of tibia. A case report. J Bone Joint Surg Br 1982;64:206-9.
3. Karchinov K. Congenital diplopodia with hypoplasia or aplasia of the tibia. A report of six cases. J Bone Joint Surg Br 1973;55:604-11.
4. Verghese R, Shah H, Rebello G, Joseph B. Pre-axial mirror polydactyly associated with tibial deficiency: A study of the patterns of skeletal anomalies of the foot and leg. J Child Orthop 2007;1:49-54.
5. Hamanishi C, Ueba Y, Iwashita Y, Yamamuro T. Diplopodia with reversed foot. Normal gait after operation at 8 years of age. Acta Orthop Scand 1985;56:439-41.
6. Shoenwolf G, Bleyl S, Brauer P, West PF. Larsen’s Human Embryology. 4th ed. Philadelphia, PA: Churchill Livingstone; 2009. p. 621-32.
7. Joseph B. The Spectrum of Congenital Tibial Dysplasia and Associated Foot Anomalies. Vol. 94B. Orthoedic Proceedings, No 23; 2018.
8. Fukazawa H, Kawabata H, Matsui Y. Mirror foot: Treatment of three cases and review of the literature. J Child Orthop 2009;3:277-82.
9. Kadir KH, Abdul Rashid AH, Das S, Ibrahim S. A rare case of diplopodia and syndactyly: Anatomical and surgical considerations. J Foot Ankle Surg 2011;50:252-6.
10. Deshmukh R, Shyam AK. Reconstruction of mirror foot with dysplastic tibia. J Orthop Case Rep 2015;5:54-6.
11. Sahdi H, Hoong CW, Rasit AH, Arianto F, Siong LK, Abdullah NA, et al. A rare case of unilateral postaxial duplicated foot in a developmentally normal child. J Orthop Surg (Hong Kong) 2017;25:1-7.
12. Jose RM, Kamath AK, Vijayaraghaban S, Verghese S, Nair SR, Nanadakumar UR. Tibial hemimelia with mirror foot. Eur J Plast Surg 2004;27:39-41.
 |
 |
| Dr. Pabitra Kumar Sahoo | Dr. Mamata Manjari Sahu |
| How to Cite This Article: Sahoo P K, Sahu M M. Mirror foot with Trapezoidal dysplastic Tibia –A Case Report. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 26-29. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


