
[box type=”bio”] Learning Point of the Article: [/box]
Diagnosis of atypical presentations of Poland Syndrome requires a keen eye and a good understanding of both classical and varying presentations of such rare syndromes.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 3-5 | Abhinav D Jogani, Prakash K George, Nandan A Marathe, Swapneel S Shah, Jigar R Desai. DOI: 10.13107/jocr.2019.v09i04.1452
Authors: Abhinav D Jogani[1], Prakash K George[1], Nandan A Marathe[1], Swapneel S Shah[1], Jigar R Desai[1]
[1]Department of Orthopaedics, Seth G.S. Medical College and KEM Hospital, Parel, Mumbai, India.
Address of Correspondence:
Dr. Prakash K George,
Department of Orthopaedics, Seth G.S. Medical College and KEM Hospital, Parel, Mumbai, India.
E-mail: drprakashkgeorge@gmail.com
Abstract
Introduction: Poland Syndrome(PS) is a rare congenital condition associated with the absence of unilateral chest wall muscles and sometimes ipsilateral symbrachydactyly (abnormally short and webbed fingers). The condition typically presents with unilateral absence of the sternal portion of the pectoralis major muscle which may or may not be associated with a hypoplasia of the breast, an ipsilateral webbing of the fingers (cutaneous syndactyly) and agenesis of 2, 3, 4, and 5 ipsilateral costal cartilages, and athelia.
Case report: We report a 13-year-old patient with an atypical variant of PS without any limb anomalies. In view of the good function of the upper limb, no surgical treatment was offered, and the patient and his family were counseled regarding the condition. A follow-up of the patient at 2 years revealed that the patient is still asymptomatic with good functional status of the upper limb.
Conclusion: It is hoped that this paper will further improve our understanding of this rare syndrome and its atypical presentations.
Keywords: Poland syndrome, atypical Poland, congenital.
Introduction
In 1841, Sir Alfred Poland first described the Poland Syndrome(PS). In 1962, a British plastic surgeon, Patrick Clarkson, coined the term Poland syndactyly. PS is a term that is more accurate because the group of anomalies includes more than just syndactyly and was given by Baudinne et al. (1967) [1]. PS cases present with absence or underdevelopment of pectoralis major muscle, associated sometimes with or without a hypoplasia of the breast, an agenesis of 2, 3, 4, and 5 ipsilateral costal cartilages, an athelia, and an ipsilateral webbing of the fingers (cutaneous syndactyly) [2, 3]. Therefore, PS may occur with varied presentation. At present, it is assumed that PS is characterized by a missing sternocostal bundle of the pectoralis major muscle [4]. The incidence ranges between 1:7,000and 1:100,000 births, with higher frequency among males (ratio: 2:1–3:1). In 75% of the cases, it is located on the right hemithorax in the unilateral form [2, 4]. Affected individuals may have variable associated features, such as underdevelopment or absence of one nipple including the areola and/or patchy absence of hair in the axilla [2, 5]. In females, there may be underdevelopment or aplasia of one breast and underlying (subcutaneous) tissues [8]. In some cases, associated skeletal abnormalities may also be present, such as underdevelopment or absence of upper ribs; elevation of the shoulder blade (Sprengel deformity); and/or shortening of the arm, with underdevelopment of the forearm bones (i.e., ulna and radius) [2, 5]. Rare association includes dextrocardia, renal hypoplasia, leukemia, and Moebius syndrome [3].
Case Report
A 13-year-old male student presented to a tertiary care center with a flattening of the right anterior chest wall since birth. He was asymptomatic with only cosmetic concerns. He was the second child, and there were no similar presentations in the family or any other associated familial disorder.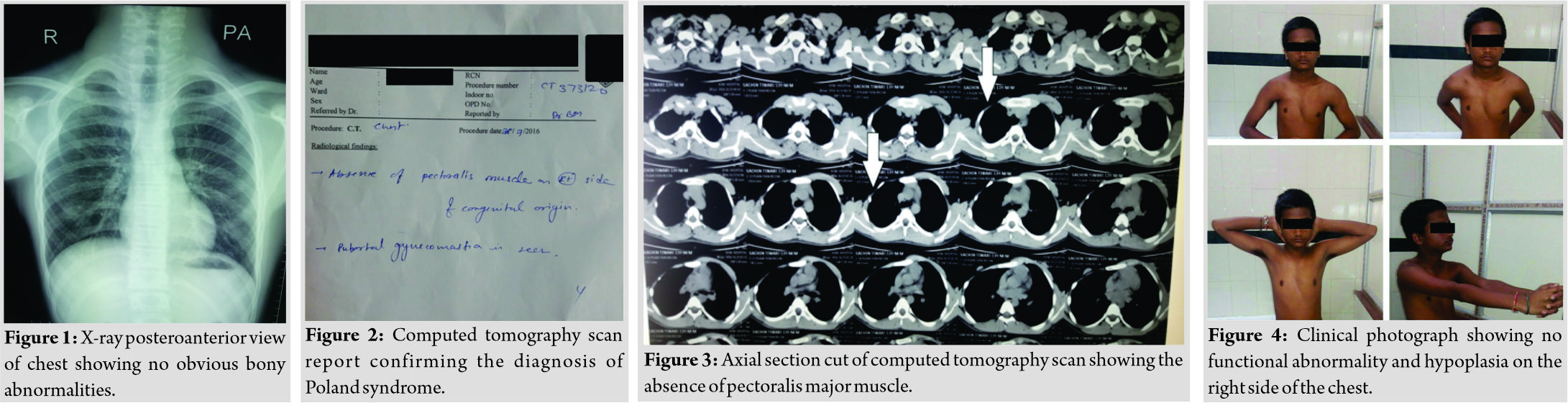
Examination revealed normal growth parameters and IQ. There was no abnormal craniofacial finding. His chest wall was asymmetric with hypoplasia of the right side (Fig. 4). The patient had a normal power in ipsilateral upper limb with full range of motion of the shoulder joint (Fig. 4)His limbs were bilaterally symmetric with no finger anomalies. Auscultation of the chest revealed normal heart sounds, breath sounds, and respiration pattern. Computed tomography scan (Fig. 2) revealed that the pectoralis major muscle was underdeveloped, but the pectoralis minor muscle and the anterior serratus muscle were present. Radiological examination of the chest showed no abnormalities of the ribs or heart (Fig. 1). Based on physical findings and the radiological picture, we diagnosed it as a case of PS. In view of the good function of the upper limb, no surgical treatment was offered and the patient and his family were counseled regarding the condition. A follow-up of the patient at 2 years revealed that the patient is still asymptomatic with good functional status of the upper limb.
Discussion
The case presented here was one of the few cases with isolated pectoralis muscle involvement and had peculiar presentation as it involved only the unilateral aplasia of the pectoralis major muscle in the right hemithorax without any other associated defects [2, 4]. The pectoralis major has many actions primarily responsible for movement of the shoulder joint. These are flexion, adduction, and medial rotation of the humerus. It is also responsible for keeping the arm attached to the trunk. Aplasia of the pectoralis muscles and associated chest defects are consequences of an interruption of early embryonic blood supply of subclavicular artery branches [6, 7]. A combination of the blockage of various branches could lead to different manifestations of PS. The interruption of the blood supply may be caused by a thrombus or embolus or due to maldevelopment of vessels. However, there have been case reports of PS associated with unusual defects, which cannot be explained on the basis of compromised blood supply alone. Hence, the true pathogenesis of PS is still a matter of debate. Most cases of PS are sporadic and occur in people with no history in their families. Rarely, this condition is passed through generations in families in an autosomal dominant pattern although no associated genes have been found. There are rare instances where more than one individual has been identified with PS either in the immediate [7,10] or extended family [10]. Therefore, some authors believe that the central underlying mechanism for this condition may be an inherited abnormal vasculature formation. Several reconstructive procedures are available to correct the deformities such as customized silicone prosthesis and transposition of the latissimus dorsi which have given satisfactory esthetic and functional results [9].
Conclusion
It is hoped that this paper will further improve our understanding of this rare syndrome and its atypical presentations.
Clinical Message
Poland Syndrome is a rare syndrome of unknown cause with a classical presentation of underdeveloped chest muscle and upper limb anomalies typically on the right side. It may be associated with varying anomalies. It is hoped that this paper will further improve our understanding of this rare syndrome and its atypical presentations.
References
1. Baudinne P, Bovy GI, Wasterlain A. Us las de syndrome de. Pland Acta Paediat Belgica 1967;32:407-10.
2. Gashegu J, Byiringiro JC, Nyundo M, Uwineza A, Mutesa L. Poland’s syndrome: A case report. East Cent Afr J 2009;14:112-4.
3. Fokin AA, Robicsek F. Poland syndrome revisited. Ann Thorac Surg 2002;74:903-18.
4. Ferraro GA, Perrotta A, Rossano F, D’Andrea F. Poland syndrome: Description of an atypical variant. Aesthetic Plast Surg 2005;29:32-3.
5. Hamidu AU, Musa A, Tahir MC. Poland’s syndrome: An incidental finding at routine medical examination. Niger J Surg Res 2006;8:97-8.
6. Czeizel A, Vitéz M, Lenz W. Birth prevalence of Poland sequence and proportion of its familial cases. Am J Med Genet 1990;36:524.
7. Hoyme HE, Der Kaloustian VM, Hogg H, Entin MA, Guttmacher AE. Possible common pathogenetic mechanisms for Poland sequence and Adams-Oliver syndrome: An additional clinical observation. Am J Med Genet 1992;42:398-9.
8. David TJ. Familial Poland anomaly. J Med Genet 1982;19:293-6.
9. Rda SF, Tolazzi AR, Martins VD, Knop BA, Graf RM, Cruz GA, et al. Poland’s syndrome: Different clinical presentations and surgical reconstructions in 18 cases. Aesthetic Plast Surg 2007;31:140-6.
10. Gocmen H, Akkas Y, Doganay S. Poland syndrome: Rare presentation in two cases. N Z Med J 2010;123:71-7.
 |
 |
 |
 |
 |
| Dr. Abhinav D Jogani | Dr. Prakash K George | Dr. Nandan A Marathe | Dr. Swapneel S Shah | Dr. Jigar R Desai |
| How to Cite This Article: Jogani A D, George P K, Marathe N A, Shah S S, Desai J R. A case report of Poland Syndrome with Absent Limb Anomalies. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 3-5. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


