
[box type=”bio”] Learning Point of the Article: [/box]
Central ray CMC disruptions have varied presentations and the associated carpal fractures can be overlooked without thorough radiological investigations.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 5-9 | Narendran Pushpasekaran, Srinivas Karthik Rathipelli, George Mathew Koshy, Veliyaveettil Muhamed Khaleel. DOI: 10.13107/jocr.2019.v09i04.1454
Authors: Narendran Pushpasekaran[1], Srinivas Karthik Rathipelli[1], George Mathew Koshy[1], Veliyaveettil Muhamed Khaleel[1]
[1]Department of Orthopaedics, Medical Trust Hospital, Cochin, Kerala, India.
Address of Correspondence:
Dr. Narendran Pushpasekaran,
Department of Orthopaedics, Medical Trust Hospital, Cochin – 682 016, Kerala, India.
E-mail: drnaren247ortho@gmail.com
Abstract
Introduction: An isolated second metacarpal dislocation is one of the least reported injuries of the hand. This particular injury assumes clinical significance as they occur subsequent to high energy direct trauma and are usually missed with associated carpal and metacarpal bone fractures. We describe this unique case of an isolated metacarpal-trapezoidal disruption with clinical presentation as the pseudo-pointing index finger and also describe a novel radiological sign to ascertain the rotational deformity of metacarpals on plain radiographs.
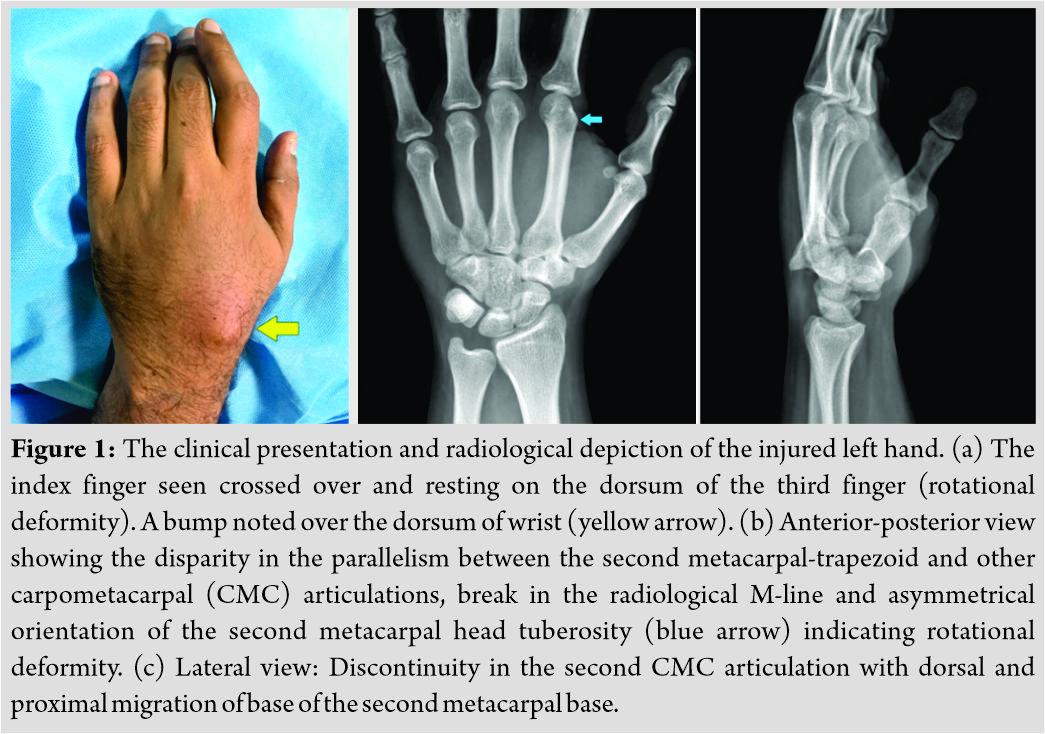
Case Report: A 32-year male information technology employee experienced a road traffic accident and developed pain, localized swelling over dorsum of the left hand. He exhibited an inability to form a complete fist with the index finger lagging behind, giving a pointing index finger like appearance. Plain radiographs showed isolated disruption of second metacarpal-trapezoid articulation. The computed tomography (CT) scans were used to confirm the absence of associated carpal injuries. The patient was managed successfully by closed reduction and Kirschner wiring. All the deformities resolved and regained normal hand functions in the follow-up period of 13 months with no recurrent episodes or evidence of arthritis.
Conclusion: Although a rare presentation, astute clinical examination and systematic radiological evaluation are the key to diagnose second through fourth carpometacarpal disruptions. The asymmetrical appearance of the metacarpal head tuberosities on anteroposterior radiographs is a strong indicator for rotational deformity of hands. These injuries must be evaluated with CT scans due to the increased potential for associated carpal injuries and poor prognosis when missed. More than often, an open reduction may be required to obtain stable concentric reduction.
Keywords: Carpometacarpal disruption, second metacarpal-trapezoid dislocation, pseudo-pointing index finger, radiology
Introduction
The carpometacarpal (CMC) dislocations are serious injuries of the hand and usually involve multiple rays [1]. However, the presentations of an isolated disruption of the anatomically stable second through fourth metacarpal articulations have been rarely reported [2]. They assume clinical significance as the literature reports these injuries to be frequently missed, have varied presentations, high degree of associated carpal bone injuries, and various obstacles to reduction [3, 4, 5]. Through our case description of an isolated second CMC dislocation with a unique clinical presentation as a pseudo-pointing index finger, we describe a novel radiological sign in addition to the systematic evaluation of CMC articulations on plain radiographs and also review the current methods to evaluate central ray CMC dislocations.
Case Report
A 32-year male information technology employee experienced a road traffic accident and sustained direct impact injury to the left hand. He presented to the emergency department with pain, localized swelling over dorsum of the left hand, rotational deformity of index finger, and inability to form a complete fist. There were no associated injuries, and the patient was hemodynamically stable. On examination of the left hand (Fig. 1a), the index finger was appeared rotated and crossed over the dorsum of the middle finger. There was tenderness at the base of the second metacarpal and localized bony prominence over the wrist.The index finger appeared to have hyperextension at the metacarpophalangeal (MCP) joint, and flexion at the interphalangeal (IP) joints with the inability to flex or extend when attempted to form a fist giving the appearance of a pointing index finger (Video 1). Plain radiographs of the left hand revealed a dislocation of metacarpal-trapezoidal joint with dorsal and proximal migration of the second metacarpal (Fig. 1b and c).
The computed tomography (CT) scan of the left wrist revealed the same, and no associated carpal injuries were observed (Fig. 2a-c).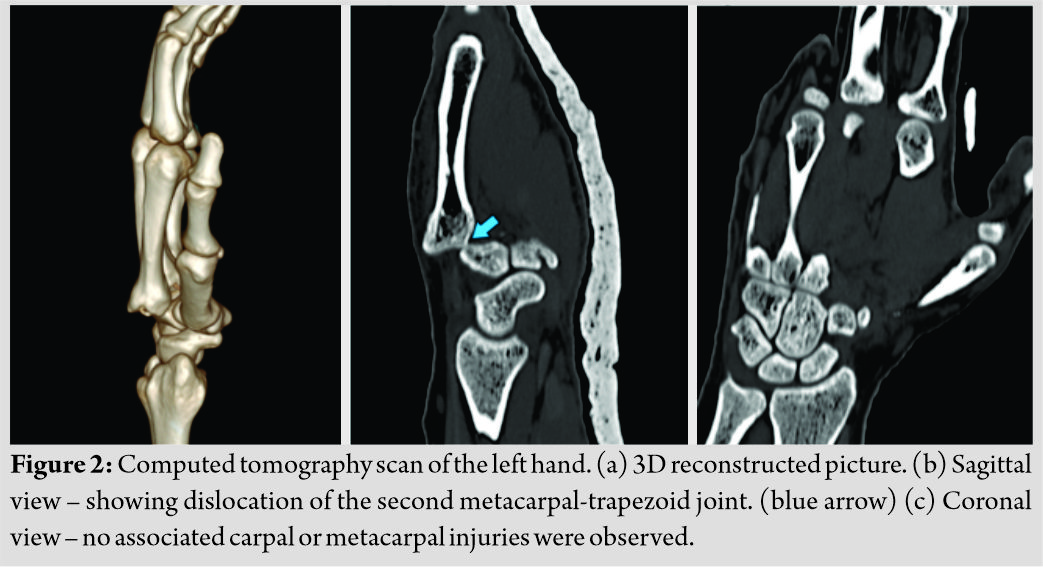 Under general anesthesia, a closed manipulation was attempted in the form of exaggerating the deformity and maneuvering a gentle distally directed force over the dislocated second metacarpal base which reduced with clunk and resolution of the deformities (Fig. 3a). The concentric reduction was attained and the articulation stabilized with a 1.5 mm Kirschner wire (K-wire) passed percutaneously under fluoroscopy guidance (Fig. 3b-d).
Under general anesthesia, a closed manipulation was attempted in the form of exaggerating the deformity and maneuvering a gentle distally directed force over the dislocated second metacarpal base which reduced with clunk and resolution of the deformities (Fig. 3a). The concentric reduction was attained and the articulation stabilized with a 1.5 mm Kirschner wire (K-wire) passed percutaneously under fluoroscopy guidance (Fig. 3b-d). 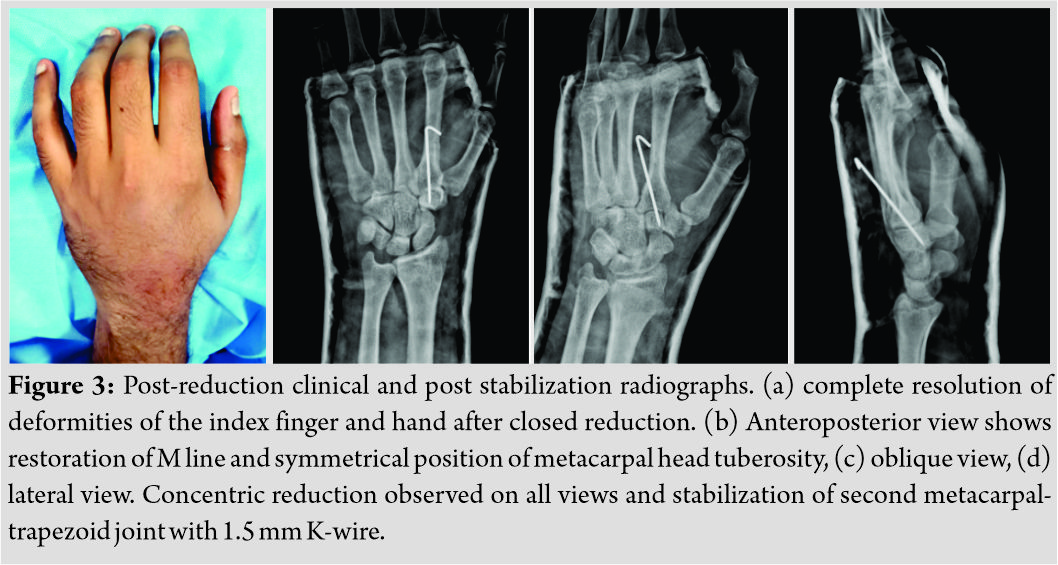 A below elbow cast with the wrist in 30° dorsiflexion was given for 3 weeks further which the K-wires were removed and rehabilitation instituted. The patient regained full range of hand functions, similar to pre-trauma status and returned to routine activities. Over the 13 months period of follow-up, no recurrent episodes or radiological evidence of arthritis were observed.
A below elbow cast with the wrist in 30° dorsiflexion was given for 3 weeks further which the K-wires were removed and rehabilitation instituted. The patient regained full range of hand functions, similar to pre-trauma status and returned to routine activities. Over the 13 months period of follow-up, no recurrent episodes or radiological evidence of arthritis were observed.
Discussion
CMC disruptions are serious injuries of the hand. They are the result of high energy direct trauma to hand and usually involve multiple rays and carpal bones [1]. Although not a common occurrence, isolated CMC dislocations have been reported in the more mobile rays of the thumb, little, and ring fingers [1, 2]. The metacarpal-trapezoid and metacarpal-capitate articulations are strongly stabilized by their bony architecture, interosseous ligaments, dorsal and volar capsular ligaments, and well anchored by tendons to form the central pillar for stable hand movements [6]. Hence, isolated dislocations of the second CMC joint are extremely rare and assume significance because they are least expected and missed, have varied presentations, have poor outcomes if inadequately treated and infrequently reported in literature [4, 5, 7]. Considering the extreme rarity of the isolated CMC dislocations, only anatomic classification prevails as dorsal, volar, or radial dislocations [2, 3]. The clinical presentations do correlate with the anatomical location as a bump, dimple, or rotated position, respectively. However, these findings could be masked due to the associated significant soft tissue swelling and missed [3, 4]. Cardozo et al. in a similar case of isolated dorsal second CMC dislocation had given the diagrammatic presentation with a bump at the base of the metacarpal and flexion at the MCP and IP joints [3]. In contrary, our patient had an attitude of extension at the MCP joint and flexion at the IP joints of the index finger and lacked any movement at these joints when attempting to form a fist giving the appearance of a pseudo-pointing index finger. Although the dorsal bump and rotational deformity of the index finger had also been noted in our patient, this attitude was the most disabling and could be explained by the fact that the metacarpal-trapezoidal disruption and proximal migration of the metacarpal had caused laxity of the long flexors and extensors to index finger and thereby deprived of the essential tension in the tendons to complete the movements. The plain radiographs are the initial way for evaluation, and often, this injury can be a distracting or be distracted by the associated injuries [4]. A systematic and sequential evaluation of the radiological anatomy of the carpal and CMC articulations is of paramount importance to avoid these injuries being missed [7]. Very often, more than two radiological views may be required and loss of the articular parallelism of CMC articulations, break in the radiological appearance of M line, variation in the cascade lines, proximal migration in the level of metacarpal head, and abnormalities in the metacarpal inclination angles can aid in suspicion of these injuries [7, 8, 9]. In addition to these subtle findings, we observed the asymmetrical orientation of the metacarpal head tubercles on an anterior-posterior view as a strong indicator for rotational malalignment. Broadbent et al. had recommended routine evaluation of CMC disruptions with CT scan emphasizing on the diagnosis of associated injuries and obstacles to reduction [10]. However, the evaluation of our patient showed an isolated ligamentous metacarpal-trapezoidal dislocation with dorsal displacement and proximal migration of the metacarpal. From the sparse literature available on this condition limited to a few case reports, more than 80% underwent open reduction. The usual structures reported to impede reduction were extensor carpi radialis brevis or longus (ECR), flexor carpi radialis, in situ rotation of trapezoid and rotated bony fragment of the second metacarpal base [3, 5, 8, 10]. van der Lei and Klasen et al. through a series of three dorsal CMC dislocations and review of similar cases observed delayed displacement in cases without stabilization [5]. ECRL, through its attachment, exerts the distracting force and recommended initial stabilization to neutralize. We had obtained a stable concentric reduction by closed means through the maneuver described in our report with complete resolution of deformities. Additional stabilization with K-wire was done to prevent displacement due to the deforming forces. Eventually, the patient had pain free hand functions and returned to pre-trauma activities. The patient had consented to share of data for academic purposes, and the same was approved by the Institutional Ethical Committee.
Conclusion
There are varied presentations of an isolated second CMC dislocation, and a pseudo-pointing index finger is one rare variant. A systematic radiological observation, including CT scans, is required in the evaluation of CMC disruptions. Isolated metacarpal-trapezoidal dislocations are complex and usually require open reductions for a congruent stable reduction.
Clinical Message
CMC dislocations imply serious injuries to the hand. Astute radiological observation, including CT scans, is required to avoid misdiagnosis and screen for associated carpal injuries. Although they are stable articulations, temporary internal fixation is required until capsuloligamentous healing to prevent late displacement by the long and powerful flexor/ extensor tendons.
References
1. Pundkare GT, Patil AM. Carpometacarpal Joint Fracture Dislocation of Second to Fifth Finger. 2015;7(4):430–435.
2. Han K-J, Lee J, Seo H. Isolated volar fracture-dislocation of the base of the second metacarpal bone by indirect injury. 2015;6(1):42-45.
3. Cardozo DFR, Plata GV, Casas JAC, Rodríguez NS. Acute Dislocation of the Metacarpal-Trapezoid Joint. Clin Orthop Surg 2016;8(2):223–227.
4. Carneiro RS, Rancatore E. Dorsal dislocation of the index carpo- metacarpal joint. J Emerg Med 2000;18(1):21–26.
5. Van Der Lei B, Klasen HJ. Dorsal carpometacarpal dislocation of the index finger: a report of three cases and a review of the English-language literature. J Trauma 1992;32:789–793.
6. Nakamura K, Patterson RM, Viegas SF. The ligament and skeletal anatomy of the second through fifth carpometacarpal joints and adjacent structures. J Hand Surg Am 2001;26(6):1016-1029.
7. Köse O, Islam C. Re: irreducible dorsal dislocation of the index carpometacarpal joint. J Hand Surg Eur. 2008;33(2):217-218.
8. Wright AC, Muir L. A Review of Published Radiographic Indicators of Carpometacarpal Dislocation Including Their Application to Volar Dislocations Through a Case Study. J Emerg Med 2015;49(3):e69-e71.
9. M, B, P, C, A. Rare carpometacarpal dislocations. Orthop Traumatol Surg Res 2016:813-816.
10. Broadbent MR, Bach OS, Johnstone AJ. In situ rotational dislocation of the trapezoid associated with carpal-metacarpal dislocations. Hand Surg 2009;14(1):31-33.
 |
 |
 |
 |
| Dr. Cedric Ngbilo | Dr. Srinivas Karthik Rathipelli | Dr. George Mathew Koshy | Dr. Veliyaveettil Muhamed Khaleel |
| How to Cite This Article: Pushpasekaran N P, Rathipelli S K, Koshy G M, Khaleel V M. Acute Traumatic Pseudo-pointing Index Finger Due to an Isolated Second Metacarpal-Trapezoid Dislocation: A Case Report. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 6-9. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


