
[box type=”bio”] Learning Point of the Article: [/box]
Proper management of super-obese patients requires special planning, preparation, resources and approach.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 31-33 | E M S Badghish, Hani H Alsulaimany, M Schotanus. DOI: 10.13107/jocr.2019.v09i04.1466
Authors: E M S Badghish[1], Hani H Alsulaimany[2], M Schotanus[3]
[1]Department of Medicine, Faculty of Health, Medicine and Life Science, Maastricht, Netherlands,
[2]Department of Orthopaedic, King Abdulaziz Medical City, Jeddah, Saudi Arabia,
[3]Department of Orthopedic, Zuyderland Medical Center, Geleen-Sittard, Netherlands.
Address of Correspondence:
Dr. E M S Badghish,
Department of Medicine, Faculty of Health, Medicine and Life Science,130-D Avenue Ceramique, 6221 KV, Maastricht, Netherlands.
E-mail: Emran.b11@gmail.com
Abstract
Introduction: Rate of obese patients are on the rise and fractures on these patients are difficult to treat, risk of management failure is high as they are more prone to develop wound infection, hardware failure, malunion and prolonged procedure time.
Case Report: In this report, we present a case on how we successfully managed a supracondylar femur fracture in a patient with a body mass index of 98.1 kg/m2 with surgical site infection as the main complication. No literature reported such a case with an astonishing weight of 264 kg given the case uniqueness and importance.
Conclusion: A retrograde intramedullary nailing of the femur was performed under difficult circumstances, with a variety of modification to be considered pre-peri and post-operatively. It is advised based on the literature review and expert opinion to take the recommendations into consideration for better outcome.
Keywords: super-obese, supracondylar fracture, femur, retrograde nailing, surgical site infection.
Introduction
Obesity is progressing in both developing and developed nations and it is becoming a global epidemic. Latest statistics reported that an estimate of 68% of Saudi Arabia’s population is overweight [1,10]. According to the European World Health Organization, data of 2008 showed that approximately 23% of women and 20% of men were obese, almost doubled since 1980. As we are facing an increasing number of patients who are obese or even morbidly obese, we must confront and prepare for such challenges in orthopedics. Prior studies reported that such patients are more prone to develop infection, hardware failure, malunion, prolonged procedure time, and many more adverse events [2, 3, 4,9]. Dealing with obese patients can be challenging in all fields of medicine when not taking good consideration, as it may require special techniques to tackle these limitations. Therefore, we would like to share our experience in how we evaluated and managed a supracondylar femur fracture in patient that is super-obese weighing 264 kg and demonstrate relative literature.
Case Report
A 68-year-old female with a body mass index (BMI) of 98.1 kg/m2presented with diabetes mellitus type 2, chronic kidney disease, hypothyroidism, and atrial fibrillation who suffered from left femur supracondylar extraarticular long oblique fracture 32-A2 (AO Muller classification) with a displacement of 31 mm (Fig.1)after stepping out of the vehicle twisting her left leg accompanied by a short distance fall to the ground. The patient has been transferred from another hospital 1 month since injury to King Khaled National Guard Hospital of Jeddah city in Saudi Arabia for evaluation and management. After looking at patient’s file, taking full history and using a portable X-ray machine for evaluation in authors’ institute, it was decided to consult concerning specialties to reevaluate patient’s general health and condition. The patient was at high risk of developing a thrombus, using warfarin with a 4 mg dose, and thus, it was advised to withdraw the warfarin and to insert an inferior vena cava (IVC) filter. Unfortunately, in accordance with the interventional radiologist, the patient was not eligible for an IVC filter due to mainly to her chronic kidney disease status, weight, and size. Regardless of such limitations, it was important to proceed for preparation of open reduction internal fixation after considering all risk factors and her medical condition.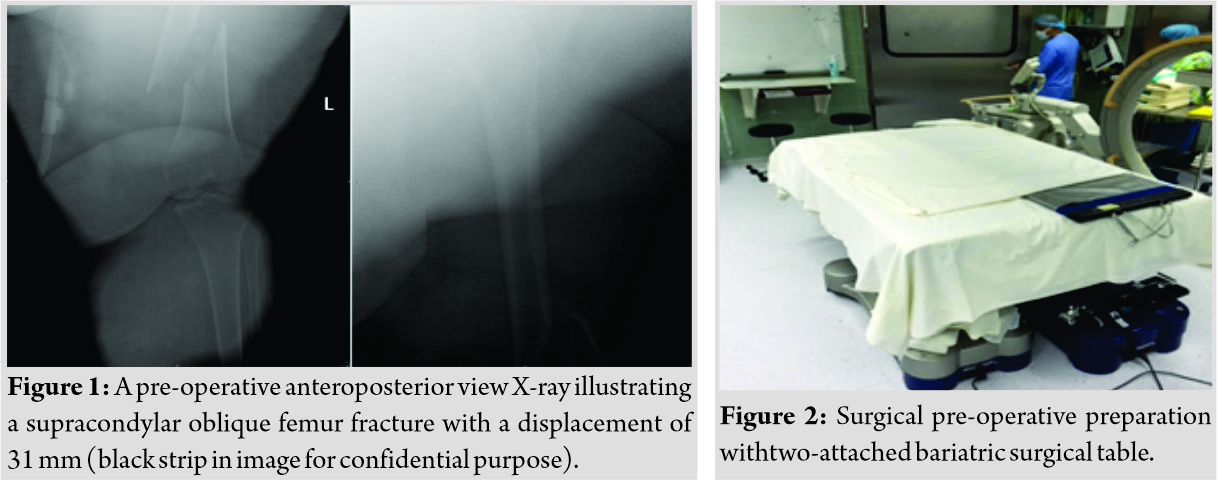
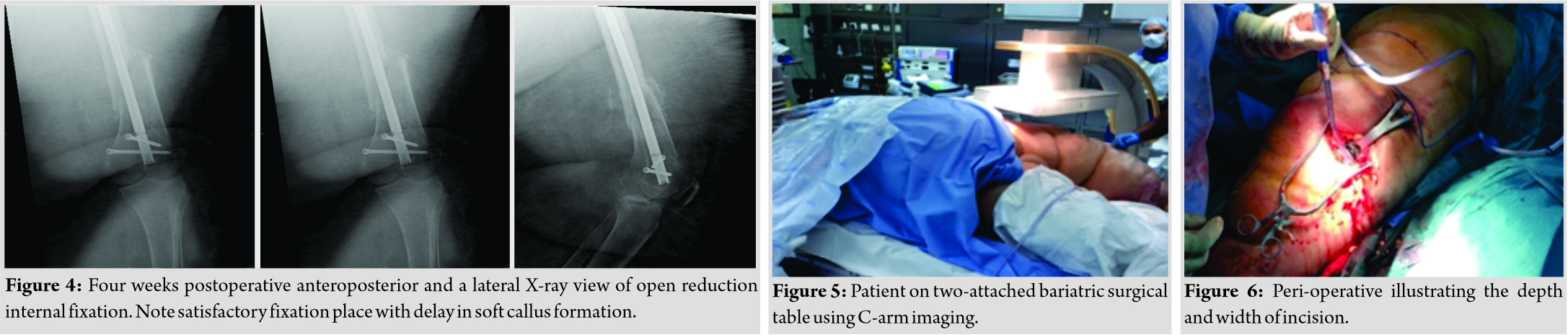
Standard pre-operative protocols and screening were performed according to international standard. However, it was of high importance to establish extra adjustments for our patient to operate in the safest environment as possible. First, it was advised to book an extra-wide bariatric intensive care unit (ICU) bed for post-operative careand second, to prepare two surgical bariatric tables that would fit her size (Fig. 2). The surgical room door was small for the extra-wide bariatric ICU bed to pass through, so she entered the room with one bariatric bed with side support. Once the patient was in theater, twelve staff members helped to transfer the patient to the two-attached bariatric surgical table (Fig.5). Third, two consultants and two specialists were prepared to participate in the surgery. Finally, an electromagnetic guidance device (TRIGEN SURESHOT, Electromagnetic targeting system, Smith and Nephew, USA) was prepared to facilitate imaging since C-arm by itself is limited to rotate freely around the patient.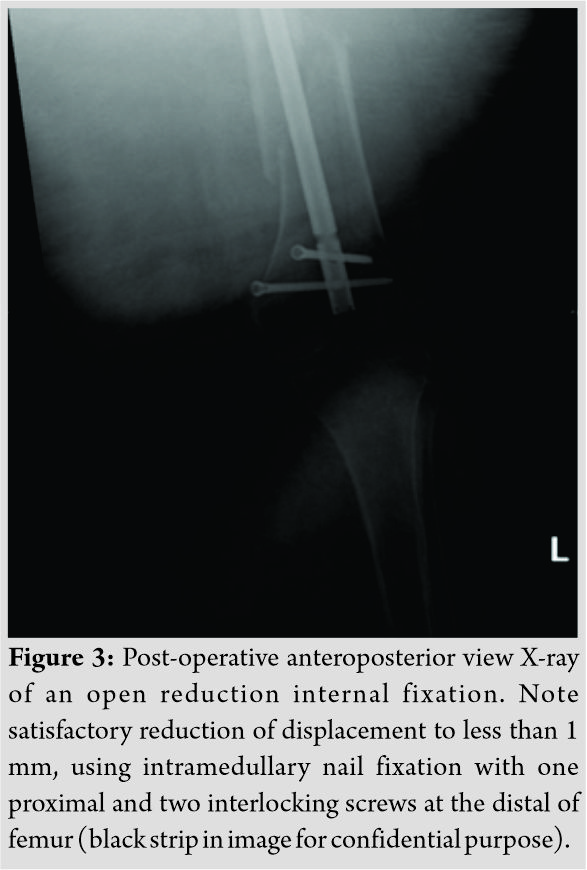
The patient ideally underwent a retrograde interlocked closed intramedullary nail (TRIGEN meta-retrograde, Smith and Nephew, retrograde intramedullary nail, USA) fixation of the femur. The surgery was performed by two experienced consultants in trauma surgery and two orthopedic specialists to assist. Extensive prep and drape preparation performed with the patient in supine position, a percutaneous entry point using guide wire achieved closed reduction. A freehand insertion of distal locking screws was established under image intensifier guidance, while proximal locking was achieved by the electromagnetic distal targeting device. The patient post-operative imaging showed satisfactory reduction on X-ray (Fig. 3).The patient did not develop any major early complication post-operatively. Surgical site infection (SSI) 6 days post-operatively was observed when patient started oozing serous fluid. Accordingly, the patient was not discharged until 4 weeks after operation due to the delay in wound closure. Meanwhile, laboratory culture result showed Staphylococcus aureus colonization, and the patient was treated efficiently with a 12-day course of vancomycin 5 mg/ml under infectious disease recommendations and changing of wound dressing (Mepilex Border, Safetac, all in one, USA) every 3 days with no necessity for debridement. Day of discharge imaging showed no infection of bone and a well-placed nail with a reduced fracture but minor delay in soft callus formation (Fig. 4).
Discussion
Handling patients that are morbidly obese can be complicated, as it was clearly illustrated in our case. In every step, a variety of challenges was observed from admission to discharge and even at home. Therefore, to reach optimal care, modification needs to be applied to some of the guidelines and procedures to accommodate the demands of patients in such form [2]. It was well reported that obese patients are at a higher risk of developing wound infection, an estimate of five folds when compared to non-obese patients [14]; however, the etiology is not completely understood. Moreover, it is reported that a wider incision also increases the chance of post-operative SSI [6]. According to the hospital recent revised protocols, it was advised to increase the dosage of pre-operative prophylactic antibiotic (cefazolin) in the obese patients from 1g to 2g which was adequately injected in our patient 30 minbefore incision [5]. Nevertheless, it was insufficient to prevent SSI. This could be explained by a recent study stated clearly that there is no clear cutoff for cefazolin injection and 2g is inadequate to prevent SSI in surgeries lasting longer than 180 min [15]. In contrast to what was previously concluded that regardless of BMI, a single dose of 2g of cefazolin provides sufficient antibiotic exposure [16]. We did not consider topical antibiotic even though a meta-analysis by McHugh reported that peri-operative topical antibiotic use has showed to be significantly beneficial in preventing SSI [17]. Considering the likelihood of SSI, the aim was to establish a minimal incision; however, the regular incision was not sufficient to accommodate the guide due to the thick skin and subcutaneous tissue around the knee, which necessitated a large incision to accommodate the metal attachment to the guide (Fig. 6). Blumensaat line was sufficiently observed as we had concern in that regard due to her weight and bone quality. Nonetheless, we also managed to successfully insert proximal locking screw of the nail using an electromagnetic guidance device as a conventional instrument since the C-arm was inapplicable because of the wide diameter of the two-attached bariatric beds, inhibiting its functional ability to rotate freely around the surgical bed. Unfortunately, for distal locking, the targeting device could not be attached, so we had to use a freehand insertion technique with an intensified X-ray imaging that required an experienced senior surgeon. Although fixation was successful, bed elevation was malfunctioning to adequately reach the level of operating table, making it difficult to transfer and position the patient. Even though our patient was susceptible in developing a thrombus, we decided to operate and take the risk to reduce the suffering of the patient. However, we carefully monitored the patient post-operatively in ICU for any signs of pulmonary embolism or related coagulopathy. Finally, when looking through the literature, cases of patients who developed a fracture who are massively obese had almost no trace in the literature; most studies had patients averaging around a BMI of 50 kg/m2 [Table1] which is almost half of our patient’s BMI. With this, for the purpose of SSI prevention, we recommend in a similar case although there is no clear formula to consider, to increasing the prophylactic dose of cefazolin more than 2g pre-operatively in a surgery that will last longer than 180 min with the use of local antibiotic peri-operatively [5, 14, 15, 16, 17]. Furthermore, a thorough and extensive prep and drape of the skin folds is necessary [2]. It is also recommended to use an electromagnetic distal targeting system as an alternative to the C-arm for locking of screws. In addition, when positioning the patient, make sure that the bed and operating table are both vertically adjustable and it is advised to have at least five staff members to adequately position the patient on surgical bed. Moreover, an extra preparation of operative instrumentation as a backup needs to be within hand. Finally and most importantly, a multidisciplinary approach is very critical for this patient.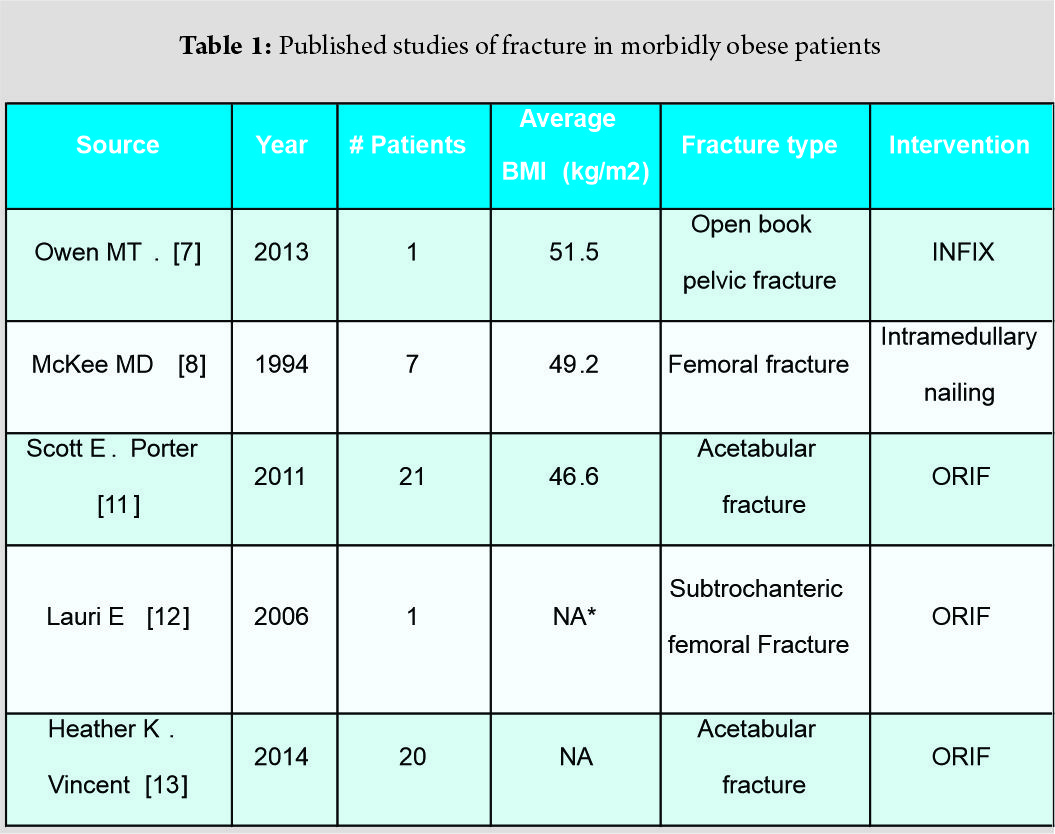
Conclusion
Clearly facing a patient of a BMI of 98.1 kg/m2is rare; standard protocols, equipment, and techniques were inapplicable and insufficient in our patient. Even in a well-equipped and established hospital, it was a burdensome to adequately treat our patient. It is advised to take into consideration the above-written recommendations. Regardless, limitation of literature made it even more challenging, sensing the need for further cases on the topic to be published as obesity is a on growing population.
Clinical Message
It is rare to treat patients with a BMI of 98 kg/m2. It is known that such patients are at risk of developing manycomplications if not addressed appropriately. It is important to consider a variety of strategies to manage such patientsefficiently.
References
1. DeNicola E, Aburizaiza OS, Siddique A, Khwaja H, Carpenter DO. Obesity and public health in the kingdom of Saudi Arabia. Rev Environ Health 2015;30:191-205.
2. Matt LG, George VR. Supracondylar femoral fracture treatment in an obese population. CurrOrthopPract2011;22:25-34.
3. Aneja A, Yang E, Briscoe M, Graves ML, Porter SE, Bergin P, et al. Intramedullary nailing of femur fractures in the obese: A retrospective comparison of patients with normal weight versus the obese. Austin J Trauma Treat 2014;1:1-5.
4. Sems SA, Johnson M, Cole PA, Byrd CT, Templeman DC, Minnesota Orthopaedic Trauma Group.et al. Elevated body mass index increases early complications of surgical treatment of pelvic ring injuries. J Orthop Trauma 2010;24:309-14.
5. Forse RA, Karam B, MacLean LD, Christou NV. Antibiotic prophylaxis for surgery in morbidly obese patients. Surgery 1989;106:750-6.
6. Nagaria T, Kujur A, Thakur N. Incision length: An emerging risk factors for surgical‐site infection following cesarean section. Int J Reprod Contracept ObstetGynecol2017;6:1829-33.
7. Owen MT, Tinkler B, Stewart R. Failure and salvage of “INFIX” instrumentation for pelvic ring disruption in a morbidly obese patient. J Orthop Trauma 2013;27:e243-6.
8. McKee MD, Waddell JP. Intramedullary nailing of femoral fractures in morbidly obese patients. J Trauma 1994;36:208-10.
9. Karunakar MA, Shah SN, Jerabek S. Body mass index as a predictor of complications after operative treatment of acetabular fractures. J Bone Joint Surg Am 2005;87:1498-502.
10. Al-Almaie SM. Prevalence of obesity and overweight among Saudi adolescents in Eastern Saudi Arabia. Saudi Med J 2005;26:607-11.
11. Porter SE, Graves ML, Maples RA, Woodall J Jr., Wallace JG, Russell GV, et al. Acetabular fracture reductions in the obese patient. J Orthop Trauma 2011;25:371-7.
12. Handolin LE, Hiltunen OJ. Peroperative di yculties in xuoroscopy of the femoral head in massive obese patient: Enhanced visualization by intra-articular contrast agent. Arch Orthop Trauma Surg2006;126:498-9.
13. Vincent HK, Haupt E, Tang S, Egwuatu A, Vlasak R, Horodyski M, et al. Perioperative and acute care outcomes in morbidly obese patients with acetabular fractures at a level 1 trauma center. J Orthop2014;11:58-63.
14. Waisbren E, Rosen H, Bader AM, Lipsitz SR, Rogers SO Jr., Eriksson E, et al. Percent body fat and prediction of surgical site infection. J Am Coll Surg 2010;210:381-9.
15. Ho VP, Nicolau DP, Dakin GF, Pomp A, Rich BS, Towe CW, et al. Cefazolin dosing for surgical prophylaxis in morbidly obese patients. Surg Infect (Larchmt) 2012;13:33-7.
16. Hites M, Deprez G, Wolff F, Ickx B, Verleije A, Closset J, et al. Evaluation of total body weight and body mass index cut-offs for increased cefazolin dose for surgical prophylaxis. Int J Antimicrob Agents 2016;48:633-40.
17. McHugh SM, Collins CJ, Corrigan MA, Hill AD, Humphreys H. The role of topical antibiotics used as prophylaxis in surgical site infection prevention. J Antimicrob Chemother 2011;66:693-701.
 |
 |
 |
| Dr. E M S Badghish | Dr. Hani H Alsulaimany | Dr. M Schotanus |
| How to Cite This Article: Badghish E M S, Alsulaimany H H, Schotanus M. A Case Report and Literature Analysis: A Supracondylar Femur Fracture in a Super-Obese Patient. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 30-33. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


