
[box type=”bio”] Learning Point of the Article: [/box]
Types of post-operative vision loss, factors contributing to it, and methods to prevent it.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 58-62 | Dhurvas Ramlal Ramprasath, Vasudevan Thirunarayanan, Arjun Rajan. DOI: 10.13107/jocr.2019.v09i04.1480
Authors: Dhurvas Ramlal Ramprasath[1], Vasudevan Thirunarayanan[2], Arjun Rajan[3]
[1]Department of Orthopaedics, Institute of Orthopaedics and Traumatology, Coimbatore Medical College Hospital, Coimbatore, Tamil Nadu, India,
[2]Department of Orthopaedics, Government Medical College, Omandurar Estate, Chennai, Tamil Nadu, India,
[3]Department of Orthopaedics, Apollo Speciality Hospitals, Chennai, Tamil Nadu, India.
Address of Correspondence:
Dr. Arjun Rajan,
6/8 Muneeswar Niwas, New No. 23 Arulambal Street, T. Nagar, Chennai – 600 017, Tamil Nadu, India.
E-mail: arjun.something@gmail.com
Abstract
Introduction: Post-operative vision loss (POVL),i.e., blindness is an uncommon complication of any major surgery. In orthopedics, it is encountered mostly in spine surgery. POVL may be due to various pathologies such asischemic optic neuropathy (ION) and central retinal artery occlusion. A rise in intraocular pressure is one of the contributing factors. ION associated with lumbar spine surgery has been designated as lumbar ION. Even though its incidence is as low as 0.02%, once occurs, the consequence is disastrous. Our case of POVL due to posterior ION has certain distinct features which differentiate it from the routine cases reported in literature.
Case Report: Our case is a 33-year-old gentleman who underwent revision lumbar spine surgery, for L3-L4 disc protrusion (recurrence) and L4-L5 disc protrusion with bilateral foot drop, in the form of posterior decompression, pedicle screw fixation from L3 to L5, and two-level transforaminal lumbar interbody fusion using cages. The patient developed POVL involving one eye which was diagnosed on operating table itself (immediately after extubation). Immediate appropriate treatment was initiated with the cooperation of ophthalmologist. The patient subsequently recovered, from no perception of light, to a visual acuity of 6/24, and is doing well regarding vision as well as neurology.
Conclusion: Since POVL is an avoidable complication, knowledge regarding POVL and its contributing factors can lead to the prevention of the development of this complication. Moreover, since POVL has poor prognosis for recovery, prevention is the key. Since POVL can occur after any major surgery (apart from orthopedics), its knowledge can help surgeons in other specialties also.
Keywords: Vision loss, spine surgery, ischemic optic neuropathy, central retinal artery occlusion, blindness, eye.
Introduction
Post-operative visual loss(POVL) is a relatively uncommon condition that can occur after any major surgery but mostly encountered in cardiac, spine, head, and neck surgeries [1]. The first case of blindness after prone spine procedure was reported by Slocum et al., in 1948(improper head positioning on a Bailey headrest was the cause) [2, 3]. The POVL may be due to various pathologies such asischemic optic neuropathy (ION),central retinal artery occlusion (CRAO), and cortical blindness (CB). IONis of two types, anterior ION(AION) and posterior ION (PION). PION has been commonly associated with lumbar spine surgery and, hence, designated as lumbar ION [4]. Visual loss after spine surgery was previously reported as 0.2% [5, 6], but according to one recent largest study, it is 0.028% [4, 5] and according to another recent study, it is 0.0309% [5]. Various surgeries that can lead to POVL include spine fusion, cardiac, obstetric surgeries, minimally invasive proctocolectomy, laparoscopic nephrectomy, and robotic prostatectomy [7]. POVL can occur both in supine and prone positions and may be unilateral or bilateral. Studies mentioning large number of cases of POVL only compiled the information gathered from various surgeons in various institutions. All other studies have only reports of one or two cases. With this background, we are reporting a case of POVL encountered in a revision lumbar spine instrumented fusion surgery performed in prone position. Our case has certain distinguished features to be noted when compared to cases reported in literature.
Case Report
A 33-year-old gentleman came to our emergency department with a history of accidental fall from a ladder of about 10 feet height. Clinically, the patient had motor weakness in L4, L5, and S1 myotomes on the left side. There was no sensory deficit. Magnetic resonance imaging (MRI) revealed traumatic L3-L4 disc protrusion (Fig. 1). On the next day itself, L3 laminectomy with L3-L4 discectomy was done. The patient was discharged on the 5th post-operative day (POD) and was advised periodical follow-up. However, the patient did not review for a period of 4 months. At the end of 4 months, he presented with back pain and bilateral foot drop (L>R). MRI (Fig. 2) revealed recurrence of disc protrusion at L3-L4 level along with L4-L5 disc protrusion.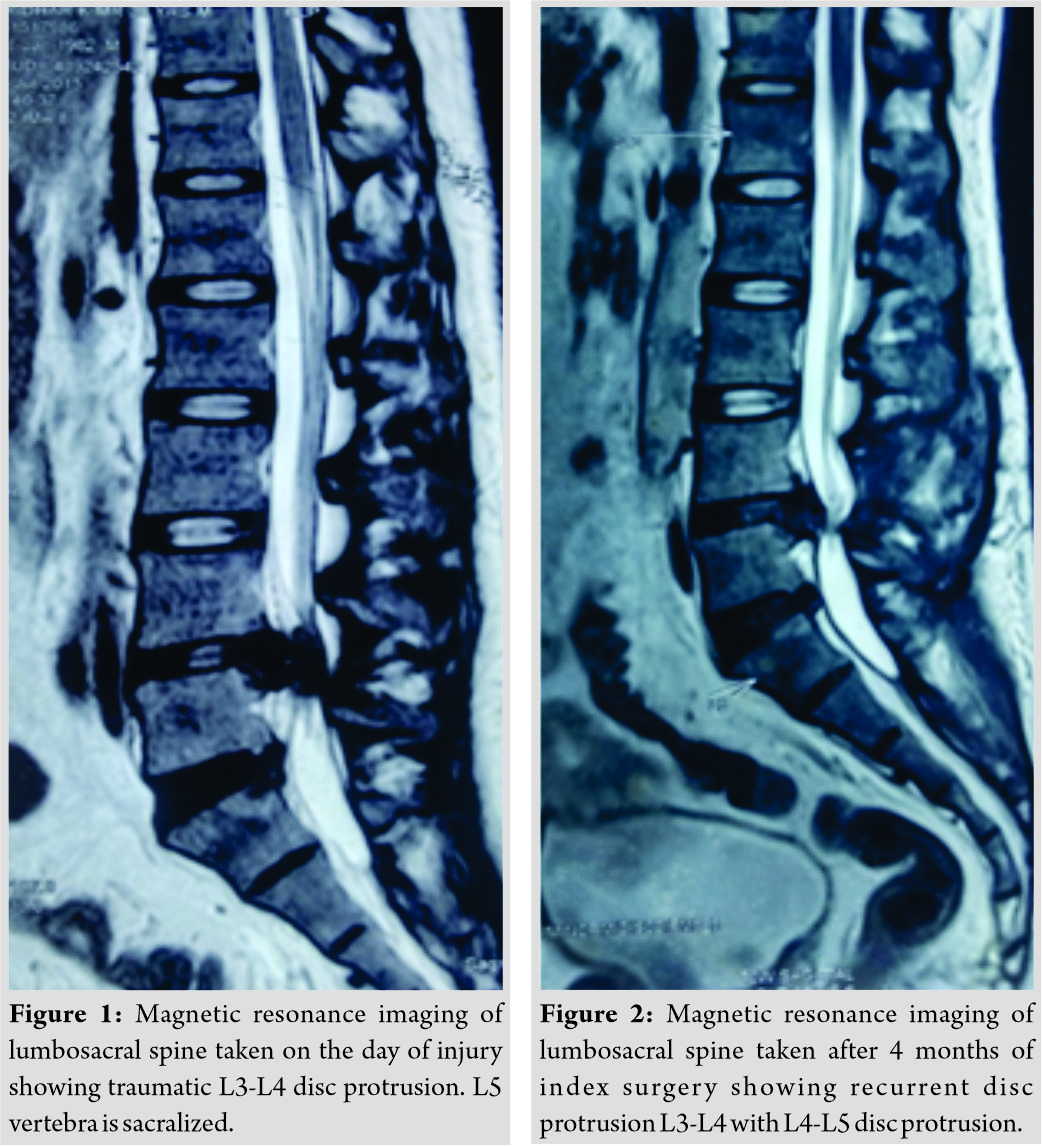
We performed revision spine surgery. With the patient placed prone to Hall’s frame (Fig. 3) with head ring for the face, under general anesthesia by extending the incision over the previous scar, L4 laminectomy, pedicle screw stabilization of L3, L4, and L5 levels, discectomy at L3-L4 and L4-L5 levels, and double level transforaminal lumbar interbody fusion with cages at L3-L4 and L4-L5 levels (Fig. 4) was performed. Surgery was uneventful and so was extubation. The amount of blood loss was calculated to be 1500ml and duration of anesthesia was 5.5 h. Immediately after extubation, on the operating table itself, the patient was questioned regarding his vision. The patient had complete loss of vision in the left eye. Pupillary reflex was absent. Examination of the right eye revealed normal vision. A diagnosis of post-operative vision loss (POVL) was made and a single dose of inj. hydrocortisone succinate 100mg was administered intravenously.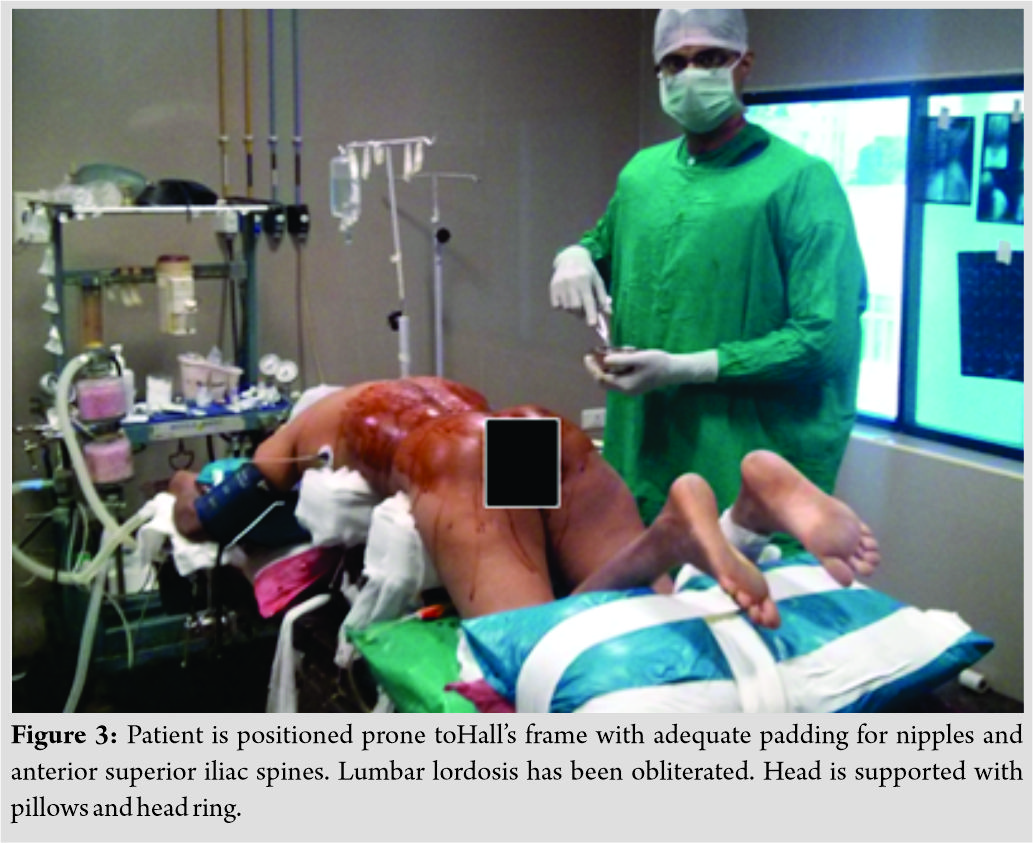
Immediately, ophthalmologist was called over and the examination (done after 2 h) revealed periorbital edema (Fig. 5), conjunctival chemosis with erythema, and presence of pupillary reflex (along with fundoscopic findings of hazy cornea). Hazy cornea obscured the examination of fundus. Since the POVL was unilateral, provisional diagnosis of CRAO was made and empirically started on oral acetazolamide, intravenous mannitol, and ocular massages. On the 1stPOD, echocardiogram was done and thromboembolic phenomenon was ruled out. Until the 6th POD, same CRAO protocol was instituted. On the 7th POD, once the patient was able to sit up and cornea was clear, a direct ophthalmoscopic examination of the fundus was done and found to be normal. As advised by the ophthalmologist, an optical coherence tomography (OCT) was done at this stage, and based on the OCT findings, diagnosis was revised as PION (Fig. 6). From this stage, inj. methylprednisolone succinate 500mg BD was administered intravenously until the 10th POD followed by oral prednisolone 20mg TDS until the 21st POD. After 3 weeks, no drug was administered for POVL.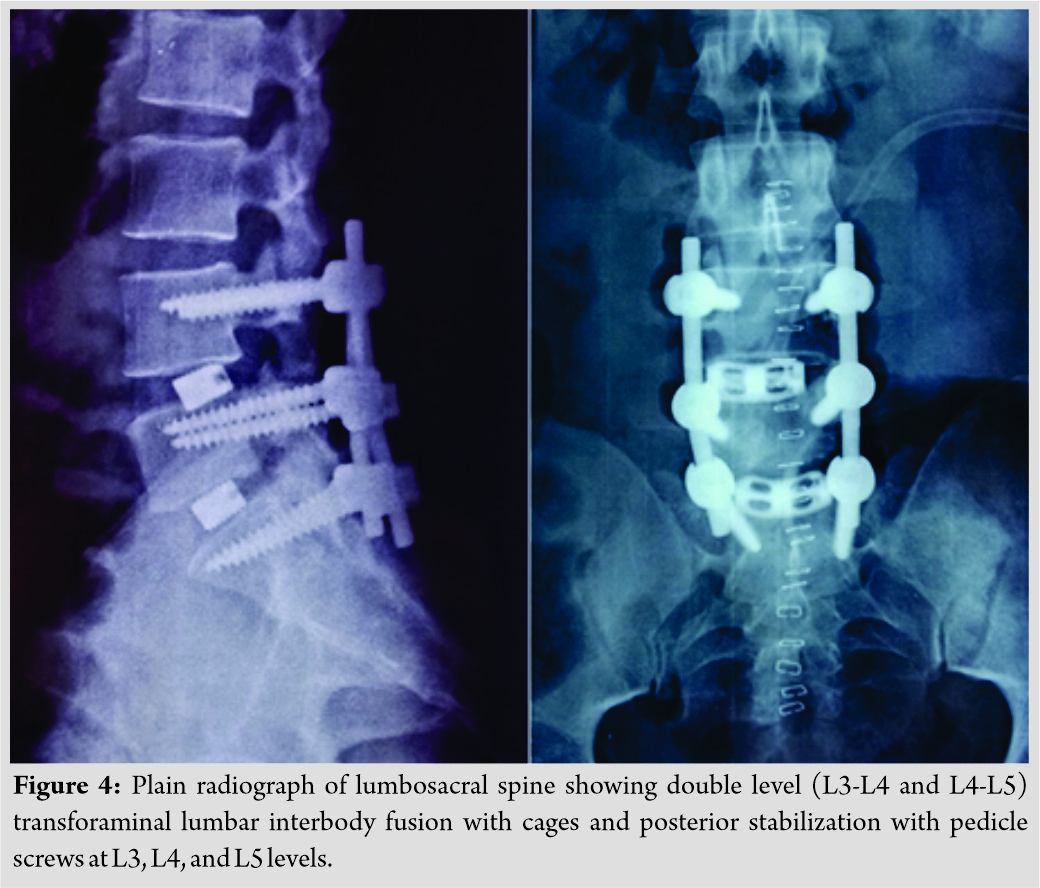
Follow-up
The recovery of vision from no perception of light on the day of surgery, progressed to perception of light on the 1st POD, hand movements on the 2nd POD, finger counting on the 7th POD, 3/60 on the 12th POD, 5/60 on the 23rd POD, 6/60 at 6-week follow-up, and 6/24 at 12-week follow-up. Once the visual acuity recovered reasonably, field of vision was mapped and found to be inferior hemianopia which improved to inferotemporal quadrantanopia at 12-week follow-up review. Intraocular pressure was not recorded until 6-week post operatively because we had fear that IOP measurement using a contact tonometer (Schiotz tonometer) might perforate the cornea (which was recovering from a hazy state). Measurement done after 6 weeks was found to be normal. Thirty-six months follow-up revealed status quo with visual acuity of 6/24 and visual field deficit of inferotemporal quadrantanopia. The patient is comfortable and performing his activities of daily living and has gone back to his wall painting job with some modifications. Regarding the neurological status, except for the extensor hallucis longus (0/5) on the left side, other deficits have recovered to 4/5. Radiologically, implants are in situ.
Discussion
Human optic nerve contains 1.2 million nerve fibers which are highly vulnerable to ischemic changes, more so due to its presence in a non-expandable bony structure [1]. Even though autoregulation of blood flow in cerebral vessels has been well demonstrated in humans [1, 8], it is not clear whether the optic nerve in humans has the ability to autoregulate [1]. Hence, various pathogeneses involving increased intraocular interstitial pressure, venous stasis, and arterial occlusion can lead to ocular ischemia and vision loss. Apart from this, cerebral involvement (e.g., CB and PRES) can lead to POVL. Numerous reports of vision loss after spine surgery exist in literature [6, 9, 10]. Even though POVL is more common in cardiac surgery (0.0864%) [5], our discussion will be centered around spine surgery (0.0309%) [5]. The fundoscopic findings can be useful in differentiating conditions such as AION, PION, CRAO, and CB. In AION, optic disc edema with or without flame-shaped hemorrhages, afferent pupillary defect will be seen. In PION, there is normal early fundoscopic examination with afferent pupillary defect. Eventually, optic nerve pallor is consistent with AION and PION. In CRAO, pale retina with cherry-red spot and afferent pupillary defect are present. In CB, fundoscopy is normal and light reflex is also normal. Following are the contributing factors for POVL– direct pressure on eye, hypotension, blood loss, anemia, hypovolemia, hypoxia, hemodilution,use of vasopressors, infusion of large amount of crystalloids, prolonged duration of surgery, prone and head-down position, and increased venous pressure [4]. Direct pressure on the eye as a contributing cause has been reported extensively in literature [3, 10, 11]. The presence of local ecchymosis and periorbital numbness in many cases with POVL substantiate the etiology. However, the development of POVL in other surgeries performed in supine position, reiterate the fact that direct pressure on the eye alone is not the etiology. Blood loss beyond certain limit has been observed in certain cases of POVL. The decreased hematocrit and/or hypotension have been attributed as contributing causes. “Substantial blood loss” has been defined as the loss that reaches an average of 44.7% of estimated blood volume [2]. In another study, estimated blood loss ≥1000ml or anesthesia duration ≥6 h was present in 96% of POVL cases [1]. The evidence of hypotension causing vision loss is made stronger by the fact that ION can occur after syncopal attacks and also rapid correction of malignant hypertension, both of which have a common denominator of hypotension without bleeding or surgery or positioning [10]. In the surgeries involving deliberate hypotension (in those patients without chronic hypertension), it is recommended that the blood pressure should be maintained within 24% of the estimated MAP or with a minimal systolic blood pressure of 84 mmHg [2, 12]. Although POVL has been encountered irrespective of whether surgery is performed in supine or prone position, the prone position adds insult to injury by creating excessive extraocular pressure, due to malpositioned headrest. This has been specifically named as “headrest syndrome” [13]. Ocular perfusion pressure is defined as the difference between mean arterial pressure and intraocular pressure [9]. Therefore, a fall in the mean arterial pressure or rise in the intraocular pressure will predispose to a compromise in ocular perfusion.
The following are the contributing factors which increase IOP [9]:
1. Increased extraocular pressure due to headrest
2. Increased peritoneal pressure and in turn central venous pressure due to prone position
3. Supine head down (Trendelenburg position), also prone head-down position
4. Increase arterial CO2 tension
5. Positive intraoperative fluid balance due to excessive use of crystalloids rather than colloids (predisposing to decreased oncotic pressure so that intraocular interstitial fluid pressure is increased, causing ischemia).
In another study [14], facial tissue pressure and development of pressure ulcers in prone position have been documented, but the effect on vision loss has not been addressed in the study. Review of literature in relation to statistics reveals that ION is usually bilateral and CRAO is almost always unilateral [1]. ION more often and more profoundly affects left eye [13]. In spite of the fact that more females undergo spine surgery, the incidence of POVL (ION and CRAO) is clearly more in males [5]. The protective effect of estrogen may contribute to lesser incidence in female [1,15]. Most cases of POVL are seen in the age group above 50 years except in cases due to CB where individuals <18 years have a higher prevalence [5]. Charlson comorbidity index [5] is a risk indicator specifically in POVL due to central retinal artery occlusion and CB, but not in ION. Furthermore, it is a risk indicator in cardiac but not spine surgery. For the 1sttime in history, Shen et al. have demonstrated POVL in hip replacement/femur treatment (0.0186%) and knee arthroplasty(0.0108%) surgeries [5]. According to literature, the POVL was discovered only on the 2ndPOD in 81% of patients, and in some patients, the delay in diagnosis extended upto 2-week postoperatively [10]. A common observation in almost all documented evidence suggests the absence of recovery of vision except in one case(with bilateral visual loss due to PION) where complete recovery was seen in one eye alone [13].
Our case stands distinctly when compared to cases in literature in the following aspects:
1. Age 33 years(<50 years)
2. Unilateral PION
3. Detected immediately on extubation
4. Extraorbital pressure evidenced by periorbital ecchymosis and edema
5. No other comorbidities (diabetes mellitus, hypertension, cardiac arrhythmias, etc.)
6. Recovery of vision to near normal status (6/24).
Conclusion
Considering the huge number of spine surgeries done nowadays, knowledge regarding POVL and its contributing factors becomes essential because one can avoid its complications and also avoid litigations. Once established, POVL has poor prognosis for recovery; therefore, prevention is the key.
Clinical Message
Even though POVL is a rare condition, knowledge regarding the factors contributing to its development will help to prevent the problem and, hence, will lead to increase in success rate of spine surgery. Since ION is an irreversible condition, methods to prevent its development are enumerated in this article. This article will be useful not only for orthopedic surgery but also for other surgical specialties.
References
1. Lee LA, Roth S, Posner KL, Cheney FW, Caplan RA, Newman NJ, et al. The American society of anesthesiologists postoperative visual loss registry: Analysis of 93 spine surgery cases with postoperative visual loss. Anesthesiology 2006;105:652-9.
2. Pierce V, Kendrick P. Ischemic optic neuropathy after spine surgery. AANA J 2010;78:141-5.
3. Slocum HC, O’neal KC, Allen CR. Neurovascular complications from malposition on the operating table. Surg Gynecol Obstet 1948;86:729-34.
4. Grover V, Jangra K. Perioperative vision loss: A complication to watch out. J Anaesthesiol Clin Pharmacol 2012;28:11-6.
5. Shen Y, Drum M, Roth S. The prevalence of perioperative visual loss in the United States: A 10-year study from 1996 to 2005 of spinal, orthopedic, cardiac, and general surgery. Anesth Analg 2009;109:1534-45.
6. Stevens WR, Glazer PA, Kelley SD, Lietman TM, Bradford DS. Ophthalmic complications after spinal surgery. Spine (Phila Pa 1976) 1997;22:1319-24.
7. Nickels TJ, Manlapaz MR, Farag E. Perioperative visual loss after spine surgery. World J Orthop 2014;5:100-6.
8. Drummond JC. The lower limit of autoregulation: Time to revise our thinking? Anesthesiology 1997;86:1431-3.
9. Cheng MA, Todorov A, Tempelhoff R, McHugh T, Crowder CM, Lauryssen C, et al. The effect of prone positioning on intraocular pressure in anesthetized patients. Anesthesiology 2001;95:1351-5.
10. Myers MA, Hamilton SR, Bogosian AJ, Smith CH, Wagner TA. Visual loss as a complication of spine surgery. A review of 37 cases. Spine (Phila Pa 1976) 1997;22:1325-9.
11. Wolfe SW, Lospinuso MF, Burke SW. Unilateral blindness as a complication of patient positioning for spinal surgery. A case report. Spine (Phila Pa 1976) 1992;17:600-5.
12. American Society of Anesthesiologists Task Force on Perioperative Blindness. Practice advisory for perioperative visual loss associated with spine surgery: A report by the American society of anesthesiologists task force on perioperative blindness. Anesthesiology 2006;104:1319-28.
13. Dunker S, Hsu HY, Sebag J, Sadun AA. Perioperative risk factors for posterior ischemic optic neuropathy. J Am Coll Surg 2002;194:705-10.
14. Grisell M, Place HM. Face tissue pressure in prone positioning: A comparison of three face pillows while in the prone position for spinal surgery. Spine (Phila Pa 1976) 2008;33:2938-41.
15. Jover T, Tanaka H, Calderone A, Oguro K, Bennett MV, Etgen AM, et al. Estrogen protects against global ischemia-induced neuronal death and prevents activation of apoptotic signaling cascades in the hippocampal CA1. J Neurosci 2002;22:2115-24.
 |
 |
 |
| Dr. Dhurvas Ramlal Ramprasath | Dr. Vasudevan Thirunarayanan | Dr. Arjun Rajan |
| How to Cite This Article: Ramprasath D R, Thirunarayanan V, Rajan A. LumbarIschemic Optic Neuropathy Complicating Spine Surgery – A Case Report. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 58-62. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


