
[box type=”bio”] Learning Point of the Article: [/box]
One must maintain high suspicion and perform critical evaluation of patients presenting with neck pain after trauma, even if remote, so not to miss potentially devastating injuries to the cervical spine.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 84-87 | Joseph Elsissy, Andrew Kutzner, Olumide Danisa. DOI: 10.13107/jocr.2019.v09i04.1492
Authors: Joseph Elsissy[1], Andrew Kutzner[2], Olumide Danisa[1]
[1]Department of Orthopedic Surgery, Loma Linda University School of Medicine, Loma Linda, California,
[2]Department of Orthopedic Surgery, Spectrum Health-Michigan State University, Grand Rapids, Michigan.
Address of Correspondence:
Dr. Joseph Elsissy,
Department of Orthopedic Surgery, Loma Linda University, 11234 Anderson St. Westerly C, Loma Linda, California 92354, USA.
E-mail: Jelsissy@llu.edu
Abstract
Introduction: Traumatic cervical instability, which includes bilateral facet dislocation, unilateral facet dislocation, and bilateral facet perch or subluxation, is generally treated expeditiously. Treatment is focused on providing stability of the cervical spine and mitigating sequelae such as spinal cord injury, nerve injury, cervical deformity, chronic pain, and even death. Surgical stabilization of traumatic bilateral cervical facet subluxation is the norm. There is not much-published literature concerning late treatment of neglected cervical facet subluxations or dislocations.
Case Report: We present the case of a 53-year-old female who sustained cervical spine injury in 2010 after a single car motor vehicle accident. She did not seek immediate medical care but rather self-medicated with heroin, non-prescribed oral opiates and alcohol. She also wore a store-bought soft collar for support. She presented to our office in 2016 with persistent severe neck pain along with neck stiffness, fixed cervical flexion deformity, dysphagia, and left C6 radiculopathy. Plain radiographs demonstrated regional cervical kyphosis from C4 to C6 measuring 50°as well as autofusion at the C5/6 level. Cervical computed tomography (CT) confirmed traumatic ankylosis of C5/6 and anterolisthesis at C4/5. Cervical magnetic resonance imaging revealed multilevel cervical disc degeneration, moderate central stenosis at C4/5, and multilevel foraminal stenosis. We performed circumferential surgery: Anterior C5 and C6 corpectomy, placement of an expandable cage, and anterior C4 to C6 plating. This was followed by posterior decompression, lateral mass instrumentation, and fusion from C4-7. We were able to restore forward gaze, eliminate her dysphagia and the left C6 radiculopathy, and diminish the global neck pain.
Conclusions: Neglect of unstable cervical injuries portends poor clinical results. In this case, the neglect was self-induced in part from the patient’s lifestyle, social situation, and lack of early access to healthcare. Despite the delayed treatment, surgical intervention was able to improve her quality of life and decrease her deformity.
Keywords: Neglected, delayed, cervical, fracture.
Introduction
Traumatic cervical instability, which includes bilateral facet dislocation, unilateral facet dislocation, and bilateral facet perch or subluxation, is generally treated expeditiously. Treatment of this injury type is focused on providing stability of the cervical spine as well as mitigating sequelae, which include spinal cord injury, nerve injury, cervical deformity, chronic pain, and even death. Acute surgical stabilization of traumatic bilateral cervical facet subluxation is the norm. There is a shortage of published literature concerning delayed treatment of neglected cervical facet subluxations or dislocations. Furthermore, the import of socioeconomic factors as they related to access to health care is poorly understood. This case demonstrates both delay of surgical intervention secondary to socioeconomic factors and the benefit of surgical intervention for the treatment of remote traumatic cervical instability.
Case Report
A 53-year-old female was referred to our spine clinic with complaints of chronic neck pain and stiffness; the left arm pain which radiated down the radial aspect of her arm, forearm, and hand; fixed kyphotic posture of the neck; and difficulty swallowing. She reported sustaining a traumatic neck injury 6 years prior when she was an unrestrained front seat passenger in a stolen car. Apparently, she and the driver of the vehicle were under the influence of methamphetamines when they crashed the vehicle into a tree. Both fled from the scene and did not seek medical treatment for fear of legal consequences. She developed immediate neck pain and neck stiffness. Shortly after, she developed electric-like left arm pain which radiated down the radial aspect of the upper extremity. She was homeless, uninsured, and she feared criminal prosecution as she was injured in the act of committing a felony. She began self-medicating to control her neck pain, using heroin, street bought oral opiates, and alcohol. She purchased a soft cervical collar from a local pharmacy and wore it exclusively for several months. Approximately 6 months after the injury, she noted progressive flexed cervical posture with difficulty maintaining forward gaze. Less than1 year after the accident, she was incarcerated in a local correctional facility for repeated drug convictions. The duration of incarceration was for 10 months with an additional court-ordered 6-month inpatient drug rehabilitation program. During this incarceration, the patient was evaluated for a high degree of global neck pain and deformity. Although imaging was performed in this evaluation, this patient’s cervical subluxation was not diagnosed. On completion of her rehabilitation, she was able to acquire government-assisted health insurance. At that time, the patient sought care from a primary care physician regarding her neck pain and stiffness. Initial attempts at physical therapy were unsuccessful. Outpatient plain cervical radiograph revealed a deformity and the patient was then subsequently referred to our spine clinic. On examination, she had a fixed flexion posture of her neck with limited axial rotation. She had no upper motor neuron signs nor did her exhibit weakness in upper or lower extremities. Sensory examination was normal. She had a markedly positive Spurling’s maneuver which recreated electric-like pain radiating down the left radial arm, forearm, and hand.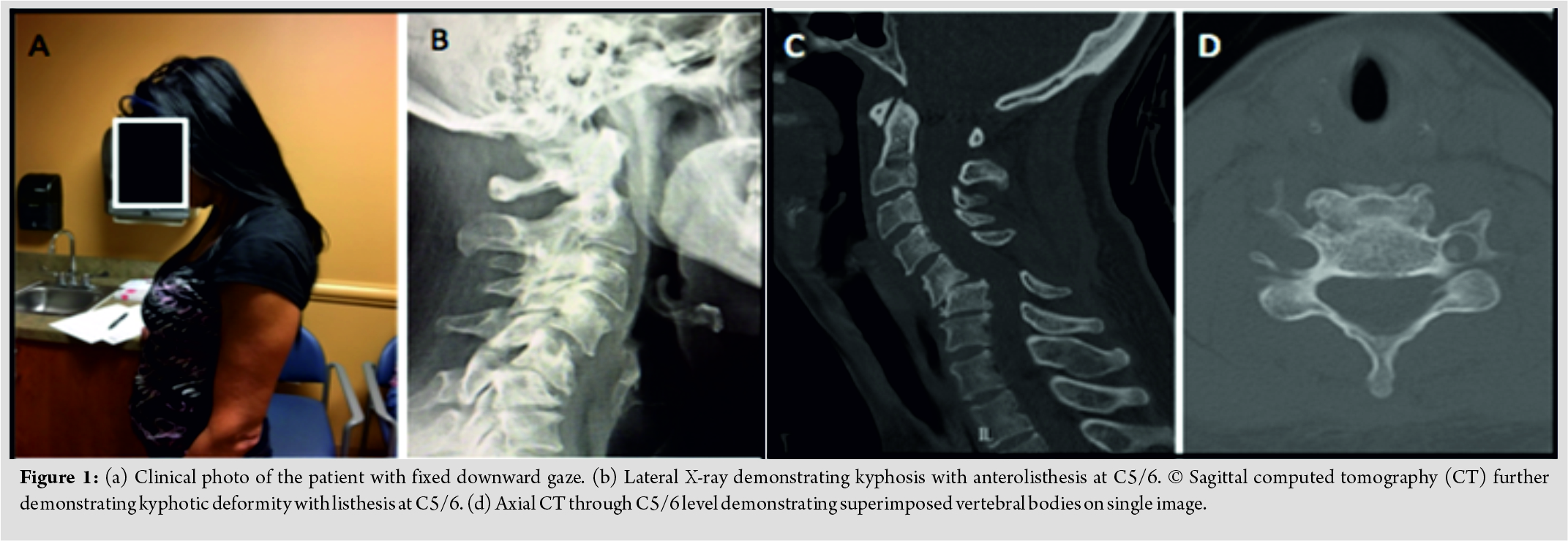
Full-length plain spine radiographs revealed regional kyphosis from C4 to C6 measuring 50°, but a normal SVA (Fig. 1). There was 3mm of anterolisthesis of C4 on C5, bony ankylosis of C5/6 at the disc level and posteriorly at the facets. Cervical CT confirmed the sagittal cervical malalignment and fusion of the C5/6 level. Cervical magnetic resonance imaging revealed multilevel cervical disc degeneration, focal kyphosis in the mid-cervicalspine, and mild-to-moderate central stenosis (worst at C4/5) and multilevel mild foraminal stenosis.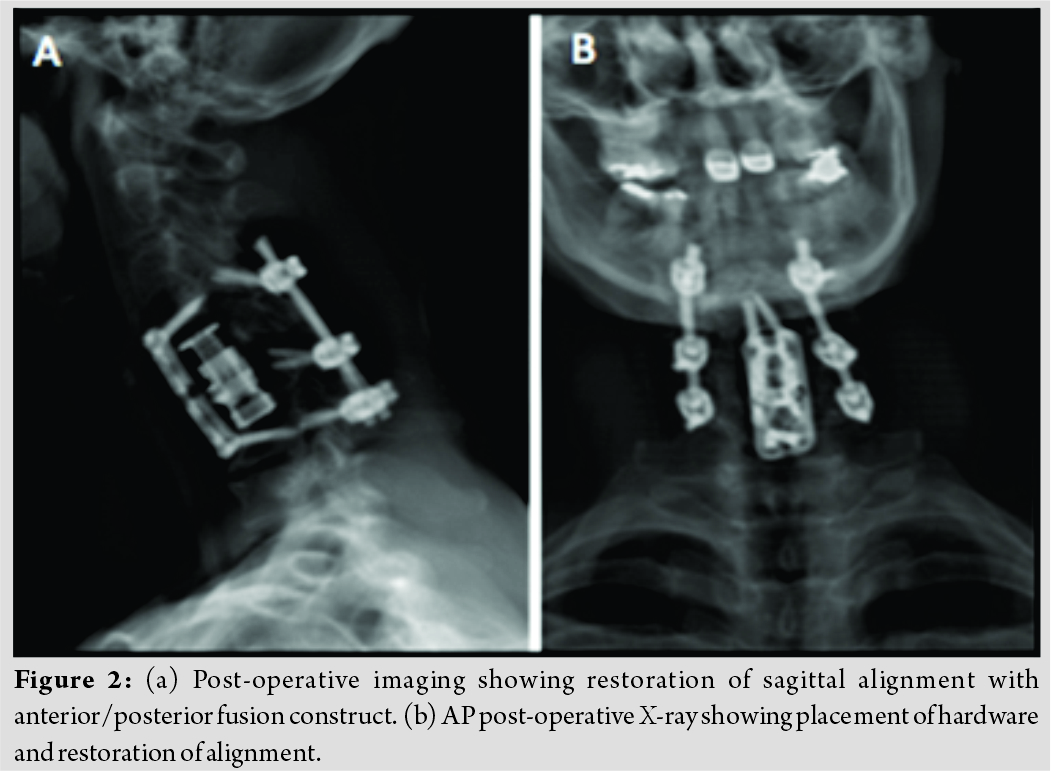
The patient was taken for elective circumferential surgery. Initial procedure was an anterior C5 and C6 corpectomy, anterior placement of an expandable titanium cage from C4-C7 and this construct was augmented by anterior plating from C4-C7. The posterior procedure comprised posterior cervical decompression from C4-7 along with lateral mass instrumentation and fusion. She was hospitalized for 3 days and was subsequently transferred to inpatient rehabilitation for 10 days. After her rehab stays, she was discharged to her daughter’s home. She wore a hard collar for 6 weeks and she also stopped smoking. She noted immediate improvement in her cervical posture in that she could achieve a forward gaze. Her dysphagia improved and left cervical radiculopathy resolved within weeks. At 2-year post-operative follow-up, her overall neck pain was improved, but she still required low-dose narcotics (Norco 5 mg every 12 h) to control this pain to an acceptable degree. The patient gave written informed consent for print and electronic publication of this report, as well as for reprint in foreign editions of this journal. The authors have no financial, or other, conflicts of interest to disclose.
Discussion
Traumatic injuries to the cervical spine resulting in cervical instability include bilateral facet dislocation, unilateral facet dislocation, and bilateral facet perch or subluxation. Such fracture-dislocation injuries of the cervical spine generally receive expeditious and appropriately aggressive intervention. Inadequate or significantly delayed treatment of these injuries is infrequently reported [1]. Such neglect of these injuries most commonly results secondary to failure to diagnose the fracture-dislocation injury in the context of limited access to medical care, as in a developing nation, but may also be the result of restraints placed by socioeconomic factors [2, 3]. Indeed, such socioeconomic factors contributed to the neglect in care of the cervical injury in the case reported. This patient, as a result of drug abuse, was in repeated violation of the law and was subsequently incarcerated. Fear of legal ramifications prevented this patient from seeking medical care after initially sustaining the trauma. This case offers a specific illustration of the wide-reaching detriment affected on the administration of timely and appropriate healthcare by substance abuse issues and on the “opioid epidemic,” in general. While legal trespasses on the part of this patient resulted in her incarceration, it should be noted that this subluxation of the cervical spine went undiagnosed throughout her legal confinement, even as the patient complained of a high degree of global neck pain and deformity and imaging was performed. Failure to appropriately address these injuries in a timely manner presented significant risk toward diminishing the patient’s quality of life or even resulting in death. Short of patient mortality, potential consequences of missed or delayed treatment of spinal injuries include progressive deformity, persistent pain, and the development of progressive neurological deficits [4]. In the case of our 53-year-old female with neglected cervical spine fracture dislocation, deformity resulted in inability to forward gaze as well as in dysphagia. This patient also suffered from severe neurologic pain of the left arm, forearm, and hand. Guidelines of treatment for these neglected injuries to the cervical spine are not well established in literature and are generally determined on a case-by-case basis [5]. Treatment is focused on providing stability of the cervical spine and mitigating sequelae such as spinal cord injury, nerve injury, deformity of the cervical spine, chronic pain, and even death. In the determination of treatment course, considerations are made for age, comorbidities, impairment in quality of life, degree of instability, as well as severity and progression of neurologic deficits. Treatment options range from conservative management in the young patient with a high degree of stability, to aggressive surgical intervention in elderly or instable patients. In the case presented, although pre-operative imaging suggested an acceptable level of stability, the impairment in quality of life in the case presented was determined to be severe. Following failure of conservative management with physical therapy, it was concluded that a more aggressive surgical approach presented an appropriate treatment option. Following the previously detailed surgical intervention, this patient experienced a marked improvement in quality of life by way of improvement of cervical deformity as well as a decrease in patient-reported global neck pain. Although there is noted clinical improvement reported in this case, the patient does continue to experience a subsequently decreased level of discomfort over the left arm, forearm, and hand, that is, severe to the point of requiring pain medication to control the discomfort. This case represents a rarely reported occurrence, particularly within the developed world, in which a traumatic insult to the cervical spine, resulting in cervical instability, was treated in a delayed fashion [6]. Although there developed significant impairments in quality of life resulting from this neglected injury, it is clear that the delayed intervention resulted in significant clinical improvement.
Conclusion
Neglect of unstable cervical injuries portends poor clinical results. In the presented case, the neglect was a result of lack of early access to health care, attributable to socioeconomic factors that had resulted in part due to the patient’s lifestyle. This specific case illustrates the detriment that the ongoing opioid epidemic affects toward access to health care.While incarcerated, the patient complained of symptoms congruous with cervical spine injury. While imaging was obtained, a missed diagnosis still resulted. This demands recognition of a bias in health-care provision against opioid abusing individuals. Despite the delayed treatment, surgical intervention was able to improve her quality of life and decrease her deformity.
Clinical Message
Cervical facet subluxations or dislocations are typically treated expeditiously. Outcomes of delayed treatment of these injuries have not been widely reported. This case demonstrates the beneficial effect of delayed treatment of cervical facet subluxations or dislocations. It is critical that proper close attention is allotted to the history and physical examination of individuals who present with a history of trauma, recent or remote, as well as symptoms including neck pain, stiffness, and loss of neck motion. Attention to imaging studies is required. Diagnosis, through careful history, physical examination, and imaging studies, allows for proper treatment, even at a date much removed from the initial injury. In this manner, the patient’s quality of life may be much improved. Furthermore, as this case demonstrates, it is essential that psycho-socioeconomic factors are addressed within history. The effect that said opioid abuse imposes on access to healthcare is demonstrated in this case. However, the scale of the impact that such socioeconomic factors have on access to healthcare remains poorly understood. There exists a need for further studies to delineate the relationship between the ongoing opioid epidemic and denial or delay of health care.
References
1. Sengupta DK. Neglected spinal injuries. Clin Orthop Relat Res 2005;???:93-103.
2. Chhabra HS, Arora M. Neglected traumatic spinal cord injuries: Causes, consequences and outcomes in an indian setting. Spinal Cord 2013;51:238-44.
3. Reid DC, Henderson R, Saboe L, Miller JD. Etiology and clinical course of missed spine fractures. J Trauma 1987;27:980-6.
4. Gerrelts BD, Petersen EU, Mabry J, Petersen SR. Delayed diagnosis of cervical spine injuries. J Trauma 1991;31:1622-6.
5. Agrawal A, Kumar SS, Ghotra HS, Singh SP. Neglected fracture-dislocation of the cervical spine without neurological deficits. Asian Spine J 2013;7:156-7.
6. Sapkas GS, Stathakopoulos DP, Chronopoulos E, Papadakis S. Neglected complete fracture-dislocation at the cervico-thoracic level without neurological deficit. Injury 1998;29:385-9.
 |
 |
 |
| Dr. Joseph Elsissy | Dr. Andrew Kutzner | Dr. Olumide Danisa |
| How to Cite This Article: Elsissy J, Kutzner A, Danisa O. Delayed Diagnosis and Management of Traumatic Cervical Spine Subluxation. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 84-87. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


