
[box type=”bio”] Learning Point of the Article: [/box]
Melioidosis is a rare cause of multifocal osteomyelitis and is a differential to be considered in an appropriate clinico-epidemiological setting.
Case Report | Volume 9 | Issue 5 | JOCR September – October 2019 | Page 95-101 | Sharandeep Singh Saluja, M. Mohan Kumar, Sridhar Gopal. DOI: 10.13107/jocr.2019.v09i05.1552
Authors: Sharandeep Singh Saluja[1], M. Mohan Kumar[1], Sridhar Gopal[1]
[1]Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research Centre, Porur, Chennai – 600 116, TamilNadu, India.
Address of Correspondence:
Dr. Sharandeep Singh Saluja,
Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research Centre, Gents Hostel, Porur, Chennai- 600116, TamilNadu, India.
E-mail: sharan.rinkle72.rs@gmail.com
Abstract
Introduction: Melioidosis caused by Gram-negative bacterium Burkholderia pseudomallei. It usually causes abscesses in lung, liver, spleen, skeletal muscle, and parotids in patient with risk factors such as diabetes mellitus, heavy alcohol use, smoking, chronic lung disease, and corticosteroid use. Musculoskeletal melioidosis is not common in India even though sporadic cases have been reported mostly involving soft tissues.
Case Report: A 45-year-old gentleman, farmer by occupation, belong to state of TamilNadu, type 1 diabetes mellitus with poor glycemic control, presented to us with complaints of multiple joint spain which includes severe pain over left elbow followed by mild pain over bilateral knee and right ankle for past 3 months and on and off fever for past 10 days. Clinically, patient was toxic (shows features of infection). On further investigation (Magnetic resonance imaging and X-ray left elbow, bilateral knee, and right ankle), it was found to be consistent with multifocal osteomyelitis. On arthrotomy and surgical debridement of the left elbow joint followed by intra-operative pus culture shows Staphylococcus aureus growth and patient was started on intravenous cefoperazone-sulbactam 1.5 g for 2 weeks, following which symptoms reappear. 2-d echo was done to rule out infective endocarditis. Technetium 99-methyl diphosphonate (MDP) whole-body scintigraphy shows increase uptake in the left elbow, bilateral knee, and right ankle. Now heunderwent bilateral knee and right ankle arthrotomy and surgical debridement. Polymerase chain reaction for melioidosis was positive. Gram-stain shows growth of B.pseudomallei. Serial blood cultures grew Gram-negative bacilli, later identified as B.pseudomallei, and diagnosed to have melioidosis, following which he was started on injection ceftazidime 2 g TDS (Q8 hourly) for 4 weeks followed by oral cotrimoxazole for next 6 months. The patient was followed up for a period of 2 years (1, 3, 6, and 12 months) and he was found to be recovered completely with no recurrences.
Conclusion: Diagnosis of melioidosis missed in many parts of the world due to lack of awareness of this infection caused by B.pseudomallei. Delay in diagnosis or treatment against melioidosis can worsen the outcome. Initial therapy with intravenous antibiotics followed by oral maintenance therapy and appropriate surgical intervention remains vital in the management.
Keywords: Burkholderia pseudomallei, melioidosis, multifocal osteomyelitis, rare.
Introduction
Melioidosis is an infectious disease, caused by a Gram-negative obligatory aerobic non-spore forming bacillus, Burkholderia pseudomallei [1]. It was first diagnosed by Captain Alfred Whitmore, and his assistant, C.S. Krishnaswami, in 1911 in Burma [2]. It is a soil saprophyte, present in stagnant water, paddy fields, and infection is through the skin through abrasions or inhalation [3]. Patients with diabetes mellitus, chronic renal failure, alcoholism, cirrhosis, and immunocompromised status are more susceptible [4, 5]. High-risk patient for suspected melioidosis includes–the most common risk factor predisposing individuals to melioidosis is diabetes mellitus, which is present in >50% of all patients with melioidosis worldwide. Individuals with diabetes mellitus have a 100-fold higher risk of melioidosis after adjustment for age, sex, and other risk factors. Other known risk factors include exposure to soil or water (especially during the rainy season. Abundant in soil at depths of10 cm from the surface), male sex (probably because of a greater risk of environmental exposure), age of >45 years, excess alcohol consumption and liver disease, chronic lung disease, chronic kidney disease, and thalassaemia (which probably causes neutrophil dysfunction due to iron overload). Prolonged steroid use and immunosuppression can also predispose individuals to infection. Nonetheless, >80% of pediatric patients and ~20% of adult patients have no recognized risk factors. Melioidosis in adults who have no risk factors generally occurs in those who have been exposed to a high bacterial load, for example, by aspiration of surface water. However, there seems to be no association with human immunodeficiency virus (HIV). Melioidosis has expanded its occurrence from the tropics to other parts of the world. Melioidosis has emerged as an important cause of morbidity and mortality for the last several decades in the Southeast hemisphere. Melioidosis has expanded its occurrence from the tropics to other parts of the world, such as other Asian regions, South America, and the Caribbean [6, 7]. Clinical manifestations of melioidosis range from latent infection, localized cutaneous lesions, sub-acute pneumonia, bone and joint infections, abscesses in body organs, and cranial abscesses to life-threatening septicemia [8, 9]. Possible differencing points of B. pseudomallei from other micro-organismsarethat B. pseudomallei is not fastidious and grows on a large variety of culture media (blood agar, MacConkey agar, eosin methylene blue, etc.). Ashdown’s medium (or Burkholderia cepacia medium) may be used for selective isolation. Cultures typically become positive in 24–48 h (this rapid growth rate differentiates the organism from Burkholderiamallei, which typically takes a minimum of 72 h to grow). Colonies are wrinkled, have a metallic appearance, and possess an earthy odor. On Gram staining, the organism is a Gram-negative rod with a characteristic “safety pin” appearance (bipolar staining). On sensitivity testing, the organism appears highly resistant (it is innately resistant to a large number of antibiotics including colistin and gentamicin) and that again differentiates it from B. mallei, which is in contrast, exquisitely sensitive to a large number of antibiotics. For environmental specimens only, differentiation from the nonpathogenic Burkholderia thailandensis using an arabinose test is necessary (B. thailandensis is never isolated from clinical specimens). Laboratory identification of B. pseudomallei can be difficult, especially in Western countries where it is rarely seen. The large, wrinkled colonies look like environmental contaminants, so they are often discarded as being of no clinical significance.The organism grows more slowly than other bacteria that may be present in clinical specimens and in specimens from nonsterile sites is easily overgrown. Nonsterile specimens should, therefore, be cultured on selective media (e.g., Ashdown’s or B. cepacia medium). For heavily contaminated samples, such as feces, a modified version of Ashdown’s that includes norfloxacin, amoxicillin, and polymyxin B has been proposed. In blood culture, the BacT/ALERT MB system (normally used for culturing mycobacteria) by BioMERT MB has been shown to have superior yields compared to conventional blood culture media. Even when the isolate is recognized to be significant, commonly used identification systems may misidentify the organism as Chromobacterium violaceum or other nonfermenting, Gram-negative bacilli such as B. cepacia or Pseudomonas aeruginosa. Again, because the disease is rarely seen in Western countries, identification of B. pseudomallei in cultures may not actually trigger alarms in physicians unfamiliar with the disease. Routine biochemical methods for identification of bacteria vary widely in their identification of this organism: The API 20NE system accurately identifies B. pseudomallei in 99% of cases, as does the automated VITEK 1 system, but the automated VITEK 2 system only identifies 19% of isolates. The pattern of resistance to antimicrobials is distinctive and helps to differentiate the organism from P. aeruginosa. The majority of B. pseudomallei isolates are intrinsically resistant to all aminoglycosides (through an efflux pump mechanism) but sensitive to coamoxiclav: This pattern of resistance almost never occurs in P. aeruginosa and is helpful in identification. Molecular methods (polymerase chain reaction [PCR]) of diagnosis are possible, but not routinely available for clinical diagnosis. Fluorescence in situhybridization has also been described but has not been clinically validated, and it is not commercially available. Musculoskeletal infection due to melioidosis is not common in India. However, several cases of soft tissue infection have been reported in the past [10, 11, 12]. Clinically, it mimics pyogenic bacterial infection, Gram-negative sepsis, tuberculosis, or even polyarthritis [13, 14, 15]. An abscess may heal after incision and drainage but may recur. The patient may present with florid pneumonia and rapidly progress to fulminant septicemia with abscess, osteomyelitis, or septic arthritis. The diagnosis is likely to be missed by the clinician and microbiologist unless a high degree of suspicion is maintained. Histopathology may show necrotizing granuloma without acid-fast bacilli, which may confuse the picture with tuberculosis [16]. It is sensitive to ceftazidime, amoxy-clavulanic acid, cotrimoxazole, and doxycycline and resistant to aminoglycosides, macrolides, second-generation cephalosporins, fluoroquinolones, and rifamycins. Serology may be helpful in cases of culture-negative results, or in the absence of clinical samples from patients with melioidosis. However, the serology results should be interpreted cautiously in endemic areas, where local populations have raised melioidosis antibodylevels. We report a rare case of multifocal osteomyelitis a rare infection in India, presented to our institute from January2017 to January 2019. The patient was followed up for period of 2 years. This case highlights that melioidosis is an important differential for chronic multifocal osteomyelitis, in an appropriate setting. A combined approach involving adequate surgical debridement and appropriate antibiotic therapy can yield good outcomes in multifocal osteomyelitis because of melioidosis.
Case Report
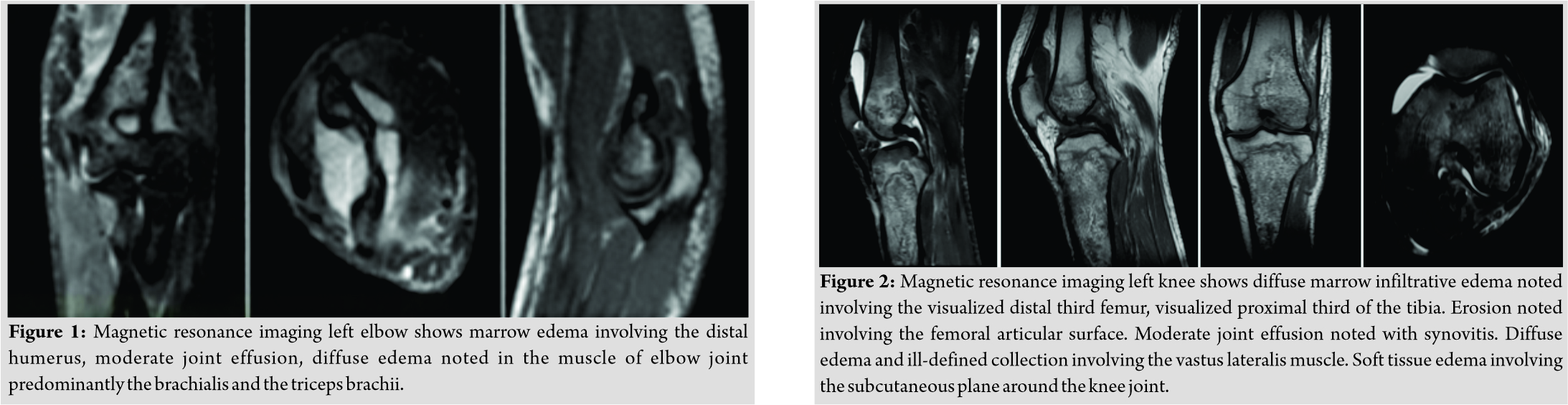
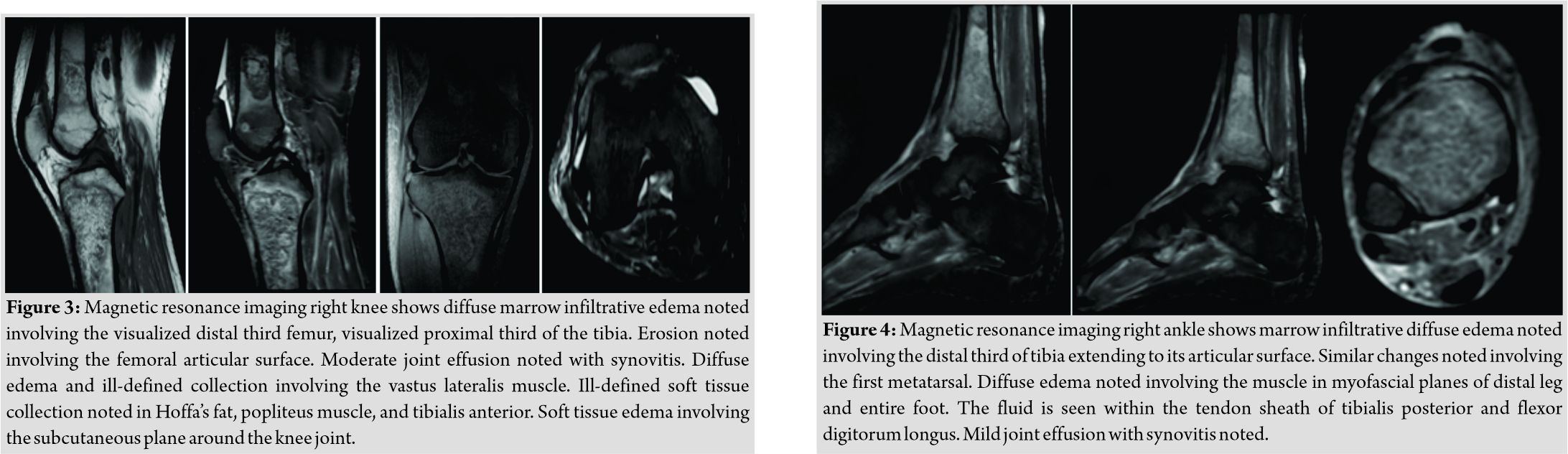
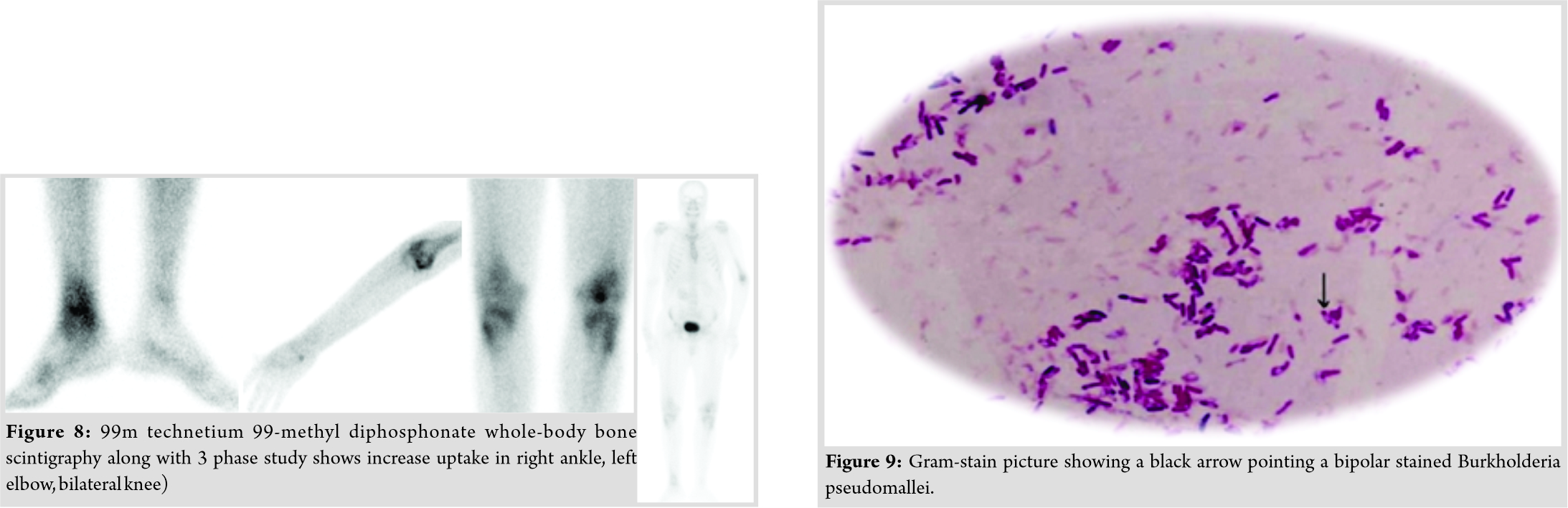
A 48-year-old gentleman from South India (resident of Chennai), farmer by occupation, presented with chief complaints of severe pain over left elbow followed by mild pain over bilateral knee and right ankle for past 3 months and on and off fever for past 10 days. History was significant for type 2 diabetes mellitus with poor glycemic control. His serology was negative for HIV. History was also significant for occupational exposure to soil. Magnetic resonance imaging (Fig. 1) of left elbow, bilateral knee (Fig. 2 and 3) and right ankle (Fig. 4) show multifocal osteomyelitis. On examination, he was febrile, tachypneic, and tachycardia. He was pale and mildly icteric.
Systemic examination was notable for mild hepatosplenomegaly, and musculoskeletal examination revealed swelling and tenderness over left elbow, bilateral knee, and right ankle with the restricted left elbow, bilateral knee, and ankle joint mobility. Initial evaluation revealed a normal white cell count (8400 cells/mm3, neutrophils 60%) and elevated inflammatory markers (erythrocyte sedimentation [ESR] rate 113 mm/h, C-reactive protein (CRP) 72 mg/L).X-ray of left elbow revealed distal humerus metaphyseal cortical irregularity and thickening with subchondralsclerosis (Fig. 5).
The patient initially underwent left elbow arthrotomy and surgical debridement. Per-operative pus was evacuated from intracapsular and intramuscular region. Intra-operative pus culture was sent. Post-operative pus culture from left elbow shows Staphylococcus aureus growth and treated with intravenous cefoperazone-sulbactam antibiotic for next 2 weeks. The patient improved briefly, after 2 weeks of intravenous antibiotic patient presented again with recurrence of same symptoms. Blood culture and echo (trans-esophageal echocardiography,trans-thoracic echocardiography)weredone to rule out infective endocarditis. X-rayof bilateral knee shows proximal tibia and distal femur metaphysis cortical irregularity and thickening (Fig. 6).

X-ray right ankle (Fig. 7) shows decrease joint space with mild subchondral sclerosis. Technetium 99-MDP whole-body scintigraphy shows increase uptake in left elbow, bilateral knee and right ankle (Fig. 8). In view of occupation, uncontrolled diabetes mellitus and non-improvement, melioidosis was suspected following which patient underwent bilateral knee and right ankle arthrotomy and surgical debridement. Per-operatively, he was noted to have involvement of bilateral knee and right ankle and intracapsular and intramuscular pus collection. Tissue sample for PCR for melioidosis was positive, and serial blood cultures grew Gram-negative bacilli, later identified asB.pseudomallei. Gram staining revealed typical bipolar stained B. pseudomallei (Fig. 9).
Fungal and mycobacterial cultures were sterile. Patient started on injection ceftazidime 2 g TDS (Q8 hourly) for 4 weeks followed by oral cotrimoxazole for next 6 months with complete clinical and biochemical parameter recovery. The patient was followed up at 1, 3, 6, and 12 months. At 12 months post-operativehe shows full clinical recovery (Fig. 10, 11, 12) His ESR at final follow-up was 14mm/h and CRP was 0.8 mg/L. He was well at completion of his eradication therapy with minimal restriction of knee joint range of movements.

His clinical picture (Fig. 13) shows complete healing with no sign of residual infection (redness, discharging sinus, and swelling).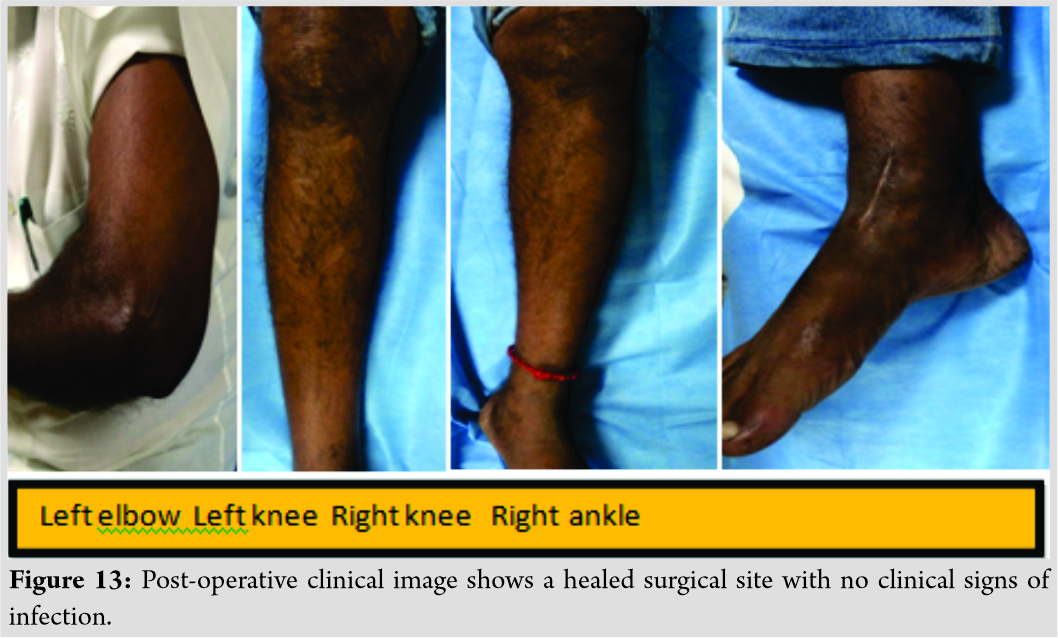
Discussion
Melioidosis caused by soil and water bacteriumB. pseudomallei is endemic to the tropical regions. India’s rural population lives in close proximity to agricultural land and is quite susceptible to this neglected killer disease. It occurs in our patients with far more frequency than imagined. However,it is underreported in India because of: (i) Lack of awareness of disease, (ii) low index of suspicion, and (iii) under-recognition of disease [16, 17]. Diabetes mellitus is the most important predisposing risk factor, and it increases the risk of melioidosis by 100-fold [18, 19, 20]. Other risk factors include splenectomy, aplastic anemia, cystic fibrosis, glucose sixphosphate dehydrogenase deficiency, and systemic lupus erythematosus [8]. High relapse rates inB.pseudomalleiinfections are mentioned in literature [21]. Relapse should be considered and treated as a first episode [22]. Recent studies have reported an increase in the cases of melioidosis diagnosed from India, dueto improved microbiological diagnostic techniques and PCR-based diagnostics [23]. Infection is acquired by inhalation, ingestion, and inoculation, and presentation can vary from localized abscesses to frank septicemia. Chronic disease is often mistaken for tuberculosis due to endemicity of both diseases in the same tropical regions [16]. Musculoskeletal involvement in the form of osteomyelitis and septic arthritis is commonly seen, and Currieet al., in a series of 540 cases of melioidosis, reported bone involvement to have an incidence of 4% [19]. Bone involvement in melioidosis can follow percutaneous inoculation or can occur in association with bacteremia, with subsequent seeding of the bone. Multifocal osteomyelitis is a rare presentation of melioidosis. Previously reported cases have been acute in their presentation, with a mean duration of symptoms of <2 weeks [24]. This suggests that a multifocal presentation usually follows bacteremia and subsequent inoculation of multiple sites. Our patient presented with symptoms for 3 months with multifocal osteomyelitis. Although any bone can potentially be involved in melioidotic osteomyelitis, there is a predilection for the involvement of long bones, especially bones around the knee joint [25, 26]. Most cases of osteomyelitis around the knee joint have associated septic arthritis. This pattern is consistent with contiguous spread of infection from one focus of seeding. Our case was unique in the fact that there was involvement of left elbow, bilateral knee, and right ankle. The clinical presentation is quite variable. It can mimic conditions from acute or chronic forms of infection to various rheumatoid disorders [16]. Cases of multifocal osteomyelitis have been noted to have poor outcomes due to delayed diagnosis. Although common infectious etiologies such as S. aureus and Neisseria species in acute settings and Brucellaspp. and Mycobacteriumspp. in chronic cases must be considered, the rare differential of multifocal osteomyelitis caused by B. pseudomallei should be kept in mind. Any delay in diagnosis and initiation of appropriate therapy could prove catastrophic. The earlier the diagnosis, the better the outcome of the patient. Hence, this needs to be thought of at the first medical contact the patient has, which very often is the primary care physician. In settings where microbiological support is suboptimal, carefully collected blood and pus samples need to be sent to centers that have appropriate microbiological and PCR-based diagnostic assays. Once antibiotic therapy is initiated empirically, cultures become sterile and often do not yield a positive culture. These cases are often treatment-modified and misdiagnosed as tuberculosis with a higher likelihood of re-presentation (at the same site or with different organ involvement), higher incidence of septicemia, and associated mortality. It is important to identify disease early, and a combined approach with prolonged antibiotic therapy, surgical debridement, and careful monitoring can give optimal results [27]. Our patient showed a good response to debridement and appropriate antibiotic therapy. At discharge, he was afebrile, ambulant, and advised a prolonged course of eradication therapy. This case highlights an unusual presentation of melioidosis, with multifocal osteomyelitis. B. pseudomallei must be considered as a differential for multifocal osteomyelitis in an appropriate clinic epidemiological setting. Primary care physicians have the best chance at making an accurate diagnosis, which weighs in significantly the mortality and long-term morbidity associated with this infection.
Conclusion
Diagnosis of melioidosis missed in many parts of the world due to a lack of awareness of this infection and lack of adequate diagnostic techniques. It mimics other disease such as tuberculosis and infections caused by S. aureus. A high index of suspicion of melioidosis is required to make the diagnosis. Delay in diagnosis or treatment against melioidosis can worsen the outcome. Initial therapy with intravenous antibiotics followed by oral maintenance therapy and appropriate surgical intervention remains vital in the management. Those patients with deep-seated or complicated infections require intravenous antibiotics for 4–8 weeks, followed by oral antibiotics for a minimum of 12 weeks. Ceftazidime is usually the intravenous antibiotic of choice, which is followed by oral therapy such as cotrimoxazole. Unfortunately no vaccine has yet been developed for this disease, which makes the awareness and understanding of melioidotic bone and joint infections, and the need for timely diagnosis and treatment, all the more relevant to microbiologists today. With increasing awareness and better diagnostic facilities, probably musculoskeletal melioidosis will be increasingly diagnosed in future.
Clinical Message
Melioidosis causing multifocal osteomyelitis is a rare condition and differential diagnosis of multifocal osteomyelitis which includes tuberculosis, infective endocarditis, pyogenic bacterial infection, and Gram-negative septicemia should be kept in mind. Early diagnosis and treatment playa key role in management.
References
1. Punyagupta S. Melioidosis: A great imitator. Ramathibodi Med J 1983;6:147-53.
2. Whitmore A, Krishnaswami CS. An account of the discovery of a hitherto undescribed infective disease occurring among the population of Rangoon. Indian Med Gaz 1912;47:262-7.
3. Leelarasamee A, Bovornkitti S. Melioidosis: Review and update. Rev Infect Dis 1989;11:413-25.
4. Chaowagul W, White NJ, Dance DA, Wattanagoon Y, Naigowit P, Davis TM, et al. Melioidosis: A major cause of community-acquired septicemia in Northeastern Thailand. J Infect Dis 1989;159:890-9.
5. Currie BJ, Fisher DA, Howard DM, Burrow JN, Lo D, Selva-Nayagam S, et al. Endemic melioidosis in tropical northern Australia: A 10-year prospective study and review of the literature. Clin Infect Dis 2000;31:981-6.
6. Gopalakrishnan R, Sureshkumar D, Thirunarayan MA, Ramasubramanian V. Melioidosis: An emerging infection in India. J Assoc Physicians India 2013;61:612-4.
7. Raja NS, Ahmed MZ, Singh NN. Melioidosis: An emerging infectious disease. J Postgrad Med 2005;51:140-5.
8. Cheng AC, Currie BJ. Melioidosis: Epidemiology, pathophysiology, and management. Clin Microbiol Rev 2005;18:383-416.
9. Vestal ML, Wong EB, Milner DA Jr., Gormley WB, Dunn IF. Cerebral melioidosis for the first time in the western hemisphere. J Neurosurg 2013;119:1591-5.
10. Rao PS, Dhawan R, Shivananda PG. Burkholderia pseudomallei infections: Case reports of five cases. Trop Doct 2002;32:174-5.
11. Kanungo R, Padhan P, Bhattacharya S, Srimannarayana J, Jayanthi S, Swaminathan RP, et al. Melioidosisa report from Pondicherry, South India. J Assoc Physicians India 2002;50:1438-9.
12. Mukhopadhyay C, Dey A, Sugandhi Rao P, Pandey V, Sripathi Rao P. Aetiology and management of chronic granulomatous osteomyelitis: Look before you leap. Singapore Med J 2007;48:e40-2.
13. Jayanetra P, Pipatanagul S, Punyagupta S, Ratanabanangkoon K, Varavithya W. Pseudomonas pseudomallei: 1. Infection in Thailand. Southeast Asian J Trop Med Public Health 1974;5:487-91.
14. Leelarasamee A. Epidemiology of melioidosis. J Infect Dis and Antimicrob Agents 1985;2:104-6.
15. McCormick JB, Weaver RE, Hayes PS, Boyce JM, Feldman RA. Wound infection by an indigenous Pseudomonas pseudomallei-like organism isolated from the soil: Case report and epidemiologic study. J Infect Dis 1977;135:103-7.
16. John TJ. Melioidosis, the mimicker of maladies. Indian J Med Res 2004;119:6-8.
17. Jesudason MV, Shanthakumari R, John TJ. Burkholderia pseudomallei-an emerging pathogen in India. Indian J Med Microbiol 1997;15:1-2.
18. Suputtamongkol Y, Hall AJ, Dance DA, Chaowagul W, Rajchanuvong A, Smith MD, et al. The epidemiology of melioidosis in Ubon Ratchatani, Northeast Thailand. Int J Epidemiol 1994;23:1082-90.
19. Currie BJ, Ward L, Cheng AC. The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS Negl Trop Dis 2010;4:e900.
20. Teparrakkul P, Tsai JJ, Chierakul W, Gerstenmaier JF, Wacharaprechasgu T, Piyaphanee W, et al. Rheumatological manifestations in patients with melioidosis. Southeast Asian J Trop Med Public Health 2008;39:649-55.
21. Currie BJ, Fisher DA, Anstey NM, Jacups SP. Melioidosis: Acute and chronic disease, relapse and re-activation. Trans R Soc Trop Med Hyg 2000;94:301-4.
22. Chaowagul W, Suputtamongkol Y, Dance DA, Rajchanuvong A, Pattara-arechachai J, White NJ, et al. Relapse in melioidosis: Incidence and risk factors. J Infect Dis 1993;168:1181-5.
23. Cousins S. India is at high risk from surge in cases of melioidosis, warn researchers. BMJ 2016;352:i275.
24. Nandurkar D, Lau K. Melioidosis as a cause of multifocal osteomyelitis. Clin Nucl Med 2006;31:25-7.
25. Raja NS, Scarsbrook C. Burkholderia pseudomallei causing bone and joint infections: A clinical update. Infect Dis Ther 2016;5:17-29.
26. Morse LP, Smith J, Mehta J, Ward L, Cheng AC, Currie BJ, et al. Osteomyelitis and septic arthritis from infection with Burkholderia pseudomallei: A 20-year prospective melioidosis study from Northern Australia. J Orthop 2013;10:86-91.
27. Shetty RP, Mathew M, Smith J, Morse LP, Mehta JA, Currie BJ, et al. Management of melioidosis osteomyelitis and septic arthritis. Bone Joint J 2015;97-B:277-82.
 |
 |
 |
| Dr. Sharandeep Singh Saluja | Dr. M. Mohan Kumar | Dr. Sridhar Gopal |
| How to Cite This Article: Saluja S S, Kumar M M, Gopal S. A Rare Case of Melioidosis Causing Multifocal Osteomyelitis in an Uncontrolled Diabetic Host. Journal of Orthopaedic Case Reports 2019 Sep-Oct;9(5): 95-101. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


