
[box type=”bio”] Learning Point of the Article: [/box]
Although an unlikely complication, distant rod migration as low as sacrum and pelvis can occur after thoracolumbar posterior pedicle screw fixation and should be kept in mind during follow-up and addressed timely to prevent complications.
Case Report | Volume 9 | Issue 5 | JOCR September – October 2019 | Page 31-34 | Sulaiman Sath, Kalyan Kumar Varma Kalidindi. DOI: 10.13107/jocr.2019.v09i05.1520
Authors: Sulaiman Sath[1], Kalyan Kumar Varma Kalidindi[1]
[1]Department of Spine Service, Indian Spinal Injuries Centre, Sector-C, Vasant Kunj, New Delhi, India.
Address of Correspondence:
Dr. Kalyan Kumar Varma Kalidindi,
Department ofSpine Service, Indian Spinal Injuries Centre, Sector-C, Vasant Kunj, New Delhi – 110070, India.
E-mail: kalyanvarmambbs@gmail.com
Abstract
Introduction: Introduction: Posterior surgical stabilization is commonly indicated for unstable thoracolumbar fractures. Short segment stabilization has the advantage of preserving mobile segments and reducing excessive loads on the adjacent discs but is not without complications. Rod migration is an extremely rare complication after thoracolumbar fracture fixation and can lead to catastrophic visceral and vascular injuries. To the best of our knowledge, this is the first case report of a surgically managed distant rod migration into the posterior sacrum and pelvis after a posterior thoracolumbar trauma fixation.
Case Report: A 25-year-old male patient presented to our center with complaints of the right buttock and groin pain for 8weeks. He had a history of an unstable thoracolumbar fracture treated by a short segment posterior stabilization 5years back. On examination and investigations, we found that the right-sided rod migrated into the posterior sacrum and partly into the pelvis. The fracture had united well in kyphosis. Anticipating complications, the rod was removed through an incision over buttock. The other implants were also removed. The patient was asymptomatic at 2-year follow-up.
Conclusion: One should keep in mind the rare possibility of rod migration during follow-up of thoracolumbar trauma fixation. A proper history and clinical examination may guide the surgeon into such a rare possibility. Radiological investigations should be performed if there is suspicion and surgery may be advised when complications are anticipated depending on the location of the rod.
Keywords: Rod migration, sacrum and pelvis, thoracolumbar trauma fixation.
Introduction
Thoracolumbar junction is a common site of injury due to the transition from a rigid thoracic spine to a flexible lumbar spine. Posterior surgical stabilization is commonly indicated for unstable thoracolumbar fractures. Short segment stabilization has the advantage of preserving mobile segments and reducing excessive loads on the adjacent discs. It is, however, associated with higher chances of implant failure and kyphoticcollapse [1]. Complications related to spinal stabilization include wound infection, non-union, and neurological compromise [2]. Rod migration is one of the rare complications of spinal stabilization and described rarely in literature with the majority of cases reported after anterior spine procedures [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. We describe a case of distant rod migration into the posterior sacral region with partial migration into the pelvis;5 years after, a thoracolumbar fracture-dislocationwas managed by short segment posterior pedicle screw fixation.
Case Report
A 25-year-old male patient presented to our center with pain in the right buttock and groin region for the past 8weeks. The pain was insidious in onset, non-progressive, pricking type, mild to moderate in intensity, and increased on sitting, particularly on hard surfaces or on the ground and relieved by lying down. There was no diurnal variation. A shopkeeper by profession, he had difficulty in doing activities which involved sitting for longer than 2–5 min. He did not have any history of recent trauma before the onset of symptoms. There were no associated systemic symptoms or bowel and bladder symptoms. The patient had a history of a road traffic accident 5 years back when he sustained anL1-L2fracture-dislocation (AO Type C) with weakness in both lower limbs (left>right) and urinary retention for which a short segment pedicle screw fixation from L1toL3 was done (Fig. 1 and 2). He had complete recovery of motor power and bladder control within 3 months of surgery and resumed his activities of daily living as well as his profession by3 months post-surgery.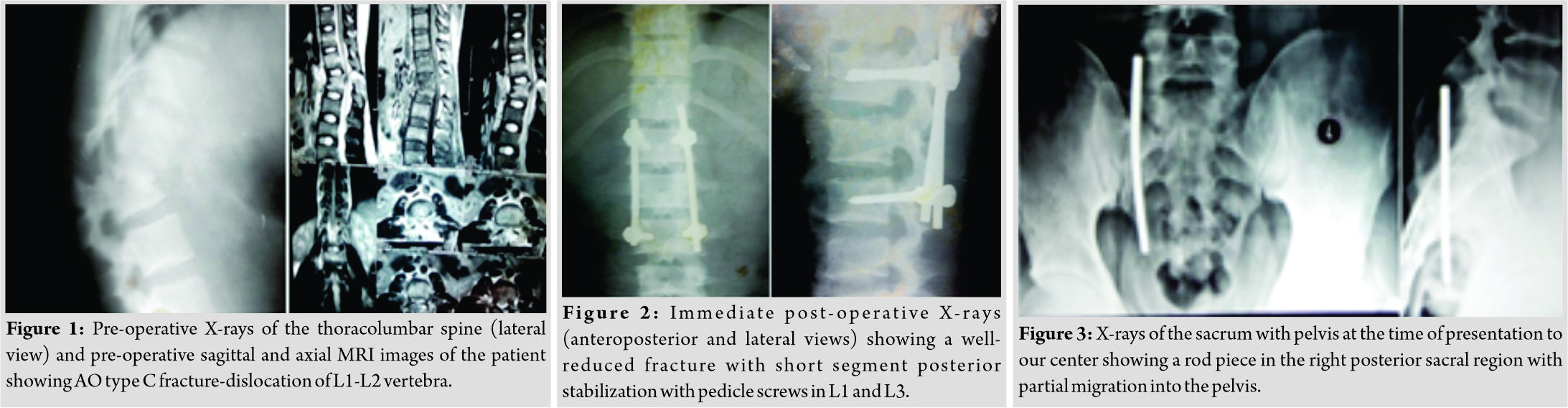
Physical examination revealed a hard and sharp localized swelling with well-defined margins in the right buttock region. The swelling was non-tender, non-fluctuant,not compressible, and non-pulsatile. The skin overlying the swelling and the surrounding region was normal. The swelling was slightly mobile and the skin was freely mobile over the swelling. There was a healed midline scar at the thoracolumbar junction. The neurological examination was unremarkable. The range of motion of the spine and hips was within normal limits. There were no clinical signs of infection and the blood tests (total blood counts, erythrocyte sedimentation rate, and C-reactive protein) were within the normal range. Anteroposterior and lateral X-rays of the pelvis revealed a rod in the right sacral region with partial migration into the pelvis (Fig. 3). X-raysof the lumbar spine showed that the rod piece on the right side was missing (Fig. 4). The fracture had completely healed and there was residual kyphosis at the fracture site. On this surprising finding, the patient was advised surgery to prevent possible skin damage by the tip of the rod or possible migration into the pelvic cavity. Written informed consent was taken. After a complete pre-operative workup, the patient was taken to the operation theater. The residual screws and rod at the site of the previous surgery were removed using the same previous incision. The set screws on the side of rod migration were found to be tight. The migrated rod was removed using a separate incision over the buttock at the site of projection of the rod through the skin (Fig.5). There was fibrosis around the rod which was released. He had complete resolution of symptoms and returned to his normal activities in 2 weeks.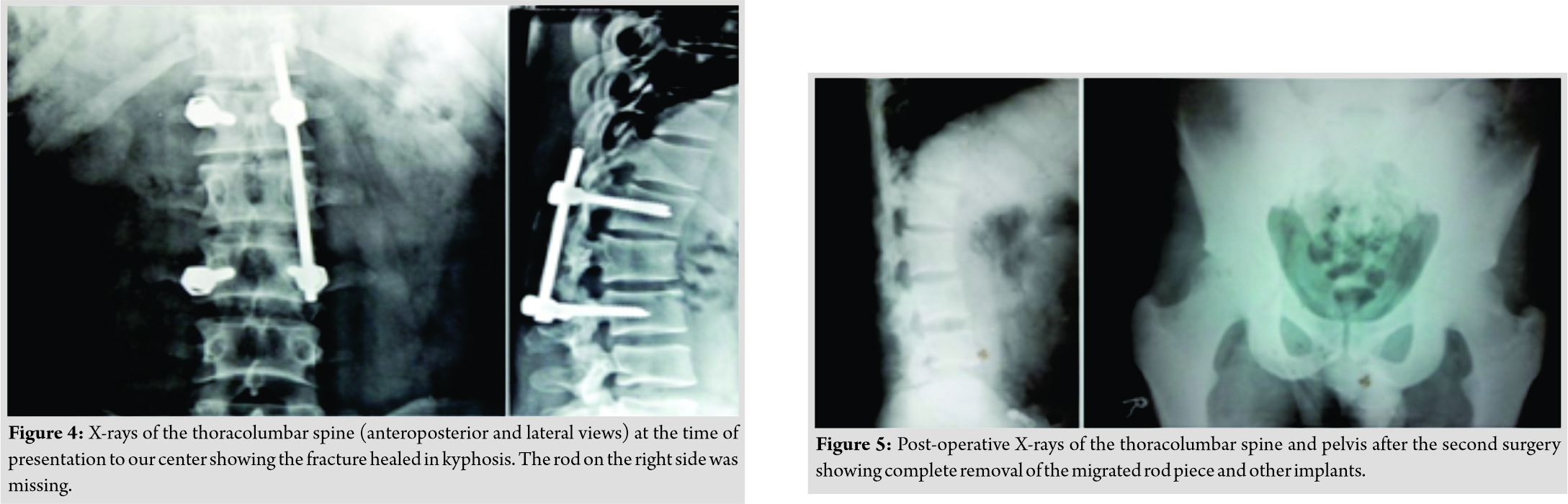
Discussion
Posterior stabilization by pedicle screw fixation has been the standard of care for the majority of unstable thoracolumbar fractures but is not without complications [2]. Short segment stabilization is reported to have a failure rate of around 9–54% with rekyphosis of 50–90% of patients with significant body collapse in some studies [14]. Most of the implant failures occur within the 1styear of surgery and rarely thereafter [15]. Distant rod migration is an extremely unusual complication after posterior spine surgery [9,10,13]. In our case, short segment fixation with fixation one level above and below the fractured vertebra was done excluding the fractured vertebra. Irrespective of an only four-screw construct, the patient recovered well and returned to normal activities within 3 months with the restoration of normal neurological status. Rod migration usually results in minimal displacement along the spinal column and most of them stay asymptomatic [12]. There have been case reports published earlier with migration of anterior instrumentation into the pleural cavity, iliopsoas muscle, thigh, knee joint and calf, and posterior migration of traditional posterior instrumentation systems (Harrington rods, CD instrumentation, and Luque rods) at the lower lumbar levels into the retroperitoneum and pre-sacral area [6,10,11,13]. In our case, there was distant migration of the rod into the sacral region and partial migration into the pelvis. Implant failure and rod migration commonly occur due to the failure of fusion and unbalanced motion at the stabilized segment [5,9,11]. In our case, there was a solid fusion at the fracture site and the patient was asymptomatic for many years. An inadequate surgical technique such as improper tightening of screws or implant-related factors may have led to the failure in our case. However, the long duration between the index surgery and onset of rod-related symptoms could not be explained. It is possible that the rod migration may have happened earlier, but it remained asymptomatic for years. Rod migration out of the spinal column is rare but can lead to catastrophic visceral and vascular injuries [3]. Some of the previous studies suggested follow-up instead of surgery, particularly in cases where the rod migration was asymptomatic [6,11]. Since there was a potential for visceral injury and skin damage in our case, the rod was removed through an incision over the buttock. The implant at the site of index surgery was also removed on the patient’s request as there was solid fusion at the fracture site and the status of the other rod was unknown. There was fibrosis around the rod in the buttock, indicating that the rod migration might have happened long before the onset of symptoms. To the best of our knowledge, this is the first case report of distant rod migration into the posterior sacrum and pelvis after a posterior thoracolumbar trauma fixation which had to be surgically removed.
Conclusion
A probable rod migration into the sacrum and pelvis is to be kept in mind during follow-up of thoracolumbar trauma fixation. A proper history and clinical examination may guide the surgeon into such a rare possibility. Radiological investigations are to be performed if there is suspicion and surgery may need to be advised when complications are anticipated depending on the location of the rod. We believe that proper attention is to be given while torque tightening the set screws over the rod to prevent such complications.
Clinical Message
Although an unlikely complication, distant rod migration as low as sacrum and pelvis can occur after thoracolumbar posterior pedicle screw fixation and should be kept in mind during follow-up and addressed timely to prevent complications.
References
1. Aly TA. Short segment versus long segment pedicle screws fixation in management of thoracolumbar burst fractures: Meta-analysis. Asian Spine J 2017;11:150-60.
2. Slone RM, MacMillan M, Montgomery WJ. Spinal fixation. Part 3. Complications of spinal instrumentation. Radiographics 1993;13:797-816.
3. Al-Binali AM, Sigalet D, Goldstein S, Al-Garni A, Robertson M. Acute lower gastrointestinal bleeding as a late complication of spinal instrumentation. J Pediatr Surg 2001;36:498-500.
4. Banit DM, Iwinski HJ Jr. Talwalkar V, Johnson M. Posterior spinal fusion in paralytic scoliosis and myelomeningocele. J Pediatr Orthop 2001;21:117-25.
5. Chun HJ, Bak KH, Kang TH, Yi HJ. Rod migration into the posterior fossa after harms operation: Case report and review of literatures. J Korean Neurosurg Soc 2010;47:221-3.
6. Dhatt S, Kumar S, Arora N, Dhillon M, Tripathy SK. Migration of anterior spinal rod from the dorsolumbar spine to the knee: An unusual complication of spinal instrumentation. Spine (Phila Pa 1976) 2010;35:E270-2.
7. Fitchett J, Williams GL, McKain ES, Stephenson BM. A hard object in the right iliac fossa. Ann R Coll Surg Engl 2008;90:W10-1.
8. Hirano K, Deguchi M, Kanamono T. The migration of a broken Luque rod: A case report. J Spinal Disord Tech 2007;20:176-9.
9. Iacoangeli M, Di Rienzo A, Nocchi N, Alvaro L, Gladi M, Colasanti R, et al. An unusual instrumentation-related s1 radiculopathy in a patient treated for a primary vertebral (l3) lymphoma. Clin Med Insights Oncol 2012;6:375-80.
10. Ilbay K, Yasa N, Ilbay G, Etus V. Migration of a lumbar rod to posterior sacral region: An extremely unusual complication of spinal instrumentation. J Neurol Sci Turk 2014;31:209-12.
11. Wood KE, Fitch RD, Burton DC, Keiger CJ. Anterior scoliosis rod migration to the lower extremity. Spine J 2009;9:e9-12.
12. Yablon IG, Cowan S, Mortara R. The migration of a Harrington rod after cervical fusion. Spine (Phila Pa 1976) 1993;18:356-8.
13. Bayri Y, Eksi MS, Doğrul R, Koç DY, Konya D. Migration of rod into retroperitoneal region: A case report and review of the literature. Korean J Spine 2014;11:241-4.
14. McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am 1993;75:162-7.
15. Mohi Eldin MM, Ali AM. Lumbar transpedicular implant failure: A clinical and surgical challenge and its radiological assessment. Asian Spine J 2014;8:281-97.
 |
 |
| Dr. Sulaiman Sath | Dr. Kalyan Kumar Varma Kalidindi |
| How to Cite This Article: Sath S, Kalidindi K K V. An Unusual Cause of Buttock Pain after Posterior Thoracolumbar Fixation: Rod Migration into the Pelvis. Journal of Orthopaedic Case Reports 2019 Sep-Oct; 9(5): 31-34. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


