
[box type=”bio”] Learning Point of the Article: [/box]
Slipped Capital Femoral Epiphysis, secondary to epileptic seizure, can occur even in very young children.
Case Report | Volume 9 | Issue 5 | JOCR September – October 2019 | Page 35-38 | Papavasiliou Kyriakos, Stamiris Dimitrios, Stamiris Stavros, Zafeiriou Dimitrios, Tsiridis Eleftherios, Sayegh Fares. DOI: 10.13107/jocr.2019.v09i05.1522
Authors: Papavasiliou Kyriakos[1], Stamiris Dimitrios[1], Stamiris Stavros[1], Zafeiriou Dimitrios[2], Tsiridis Eleftherios[1], Sayegh Fares[1]
[1]Department of Orthopaedic, Aristotle University of Thessaloniki Medical School, Papageorgiou General Hospital, Ring Road West 56403 NeaEfkarpia, Thessaloniki, Greece,
[2]Department of Paediatrics, “Hippokratio” General Hospital, Aristotle University of Thessaloniki Medical School, Thessaloniki, Greece.
Address of Correspondence:
Dr. Papavasiliou Kyriakos,
Departmentof 3rdOrthopaedic, Aristotle University of Thessaloniki Medical School, Papageorgiou General Hospital, Ring Road west 56403 NeaEfkarpia, Thessaloniki, Greece.
E-mail: papavasiliou.kyriakos@gmail.com
Abstract
Introduction: Slipped capital femoral epiphysis (SCFE) is a rather uncommon fracture, occurring usually in adolescence, during a period of rapid growth. Various pathogenetic risk factors contributing to its development have been identified. We present the case of a 10-month-old male infant who developed SCFE in his left hip following an epileptic seizure. To the best of our knowledge, this is the first such case report in the English literature.
Case Report: A 10-month-old male infant, with a known medical history of epileptic encephalopathy, was referred to the accident and emergency department of our hospital. The parents of the youngster reported inability of the child to move his left lower limb and inconsolable crying following several epileptic seizures. A radiograph revealed the existence of SCFE in the left hip. The fracture was reduced (with gentle closed traction under general anesthesia) and a hip spicacast was applied. It was removed at 8 weeks. Physical examination at this stage revealed a painless hip with a full range of motion. Painless hip range of motion was retained during all follow-up visits throughout the next 22 months. Amagnetic resonance imaging scan at 2 years post-reduction showed normal shape and size of the affected femoral head, with no signs of physeal arrest and/or avascular necrosis.
Conclusion: This unique case of a 10-month-old infant who developed SCFE following an epileptic seizure shows that this rare fracture may occur even in very young children. Although it is not currently indicated for the treatment of the vast majority of patients with SCFE, closed reduction and immobilization in a hip spicacast may be considered as an alternative treatment option in carefully selected patients.
Keywords: Epilepsy, epileptic seizures, infant, non-traumatic slipped capital femoral epiphysis.
Introduction
The displacement of the femoral head along the upper femoral physis that occurs in adolescence during a period of rapid growth is called slipped capital femoral epiphysis (SCFE) [1]. SCFE is a rather uncommon, Salter-Harris Type-I fracture [2]. Its incidence ranges from 0.71 to 3.41 cases per 100,000 adolescents [3]. It is characterized by the slippage of the proximal femoral metaphysis anteriorly and superiorly in relation to the epiphysis. This translation occurs through the hypertrophic zone of growth plate [4]. Various pathogenetic risk factors contributing to the development of SCFE have been identified, including male gender, obesity, specific ethnicities, endocrine disorders, femoral and/or acetabular retroversion, and coxa profunda [5]. Epileptic encephalopathies are a group of neurologic disorders characterized by persistent epileptic activity. The latter may contribute to progressive psychomotor dysfunction, which can aggravate overtime, leading to progressive cerebral dysfunction. Various syndromes have been recognized based on the age of onset, the type of seizures, and electroencephalogram patterns [6]. Musculoskeletal injuries are common in patients with childhood-onset epilepsy [7]. We present the case of a 10-month-old male infant who developed SCFE in his left hip following an epileptic seizure. To the best of our knowledge, this is the first such case report in the English literature.
Case Report
This study was conducted in accordance with the ethical standards of the institutional review board of our hospital and with the 1964 Helsinki Declaration and its later amendments ethical standards.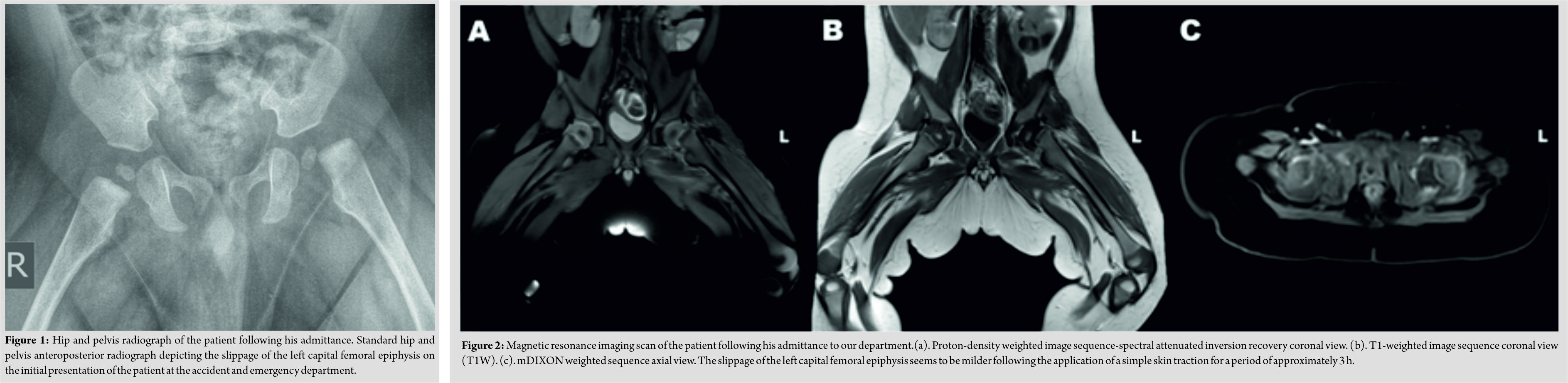
A 10-month-old male infant was referred to the accident and emergency department of our hospital by his pediatrician. The parents of the youngster reported inability of the child to move his left lower limb and inconsolable crying following any attempt to move or touch the affected limb. All symptoms had started 2 days before the referral and apart from an epileptic seizure, no other injury or any recent pathology was reported. The patient had a known medical history of epileptic encephalopathy, suffering from continuous epileptic seizures, as a result of a mutation in the chloride voltage-gated channel 2gene.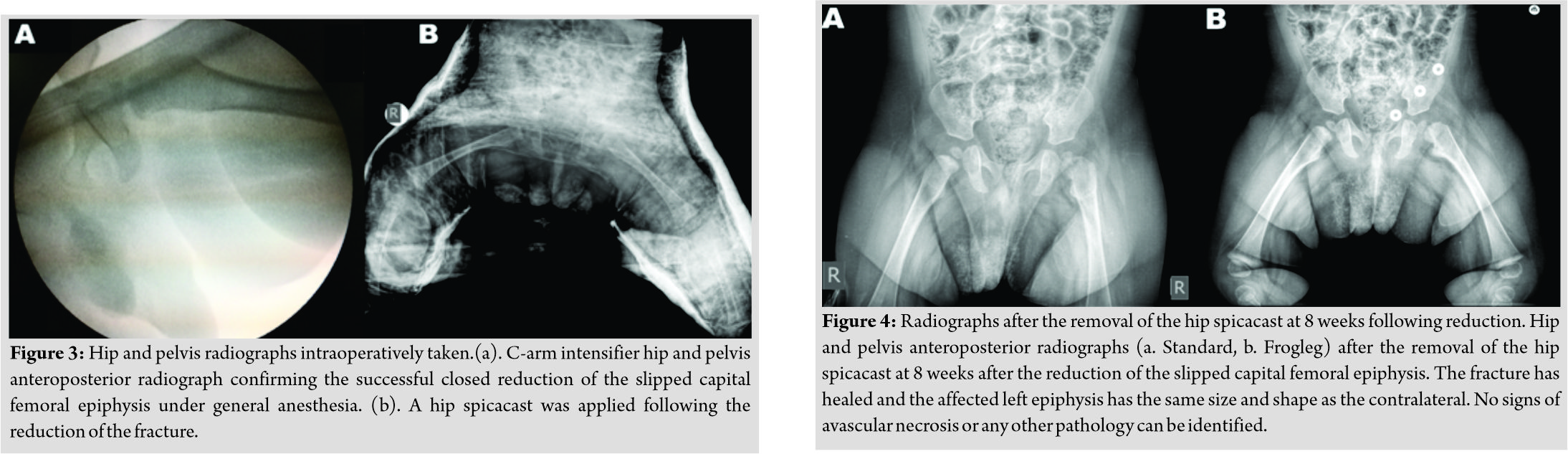
Physical examination revealed an otherwise healthy infant, with normal weight, height, and cranial perimeter for his age. The patient’s lower left limb appeared to be in pseudoparalysis;it remained in external rotation and every attempt to passively move it was painful. Routine blood test results (including inflammatory markers) were all within normal range. However, a radiograph revealed the existence of SCFE in the left hip (Fig. 1). A skin traction was put in place for analgesia and as a means to initiate– if possible– reduction of the fracture and the patient next underwent amagnetic resonance imaging (MRI)scan (Fig. 2), which confirmed the SCFE and excluded any other pathology.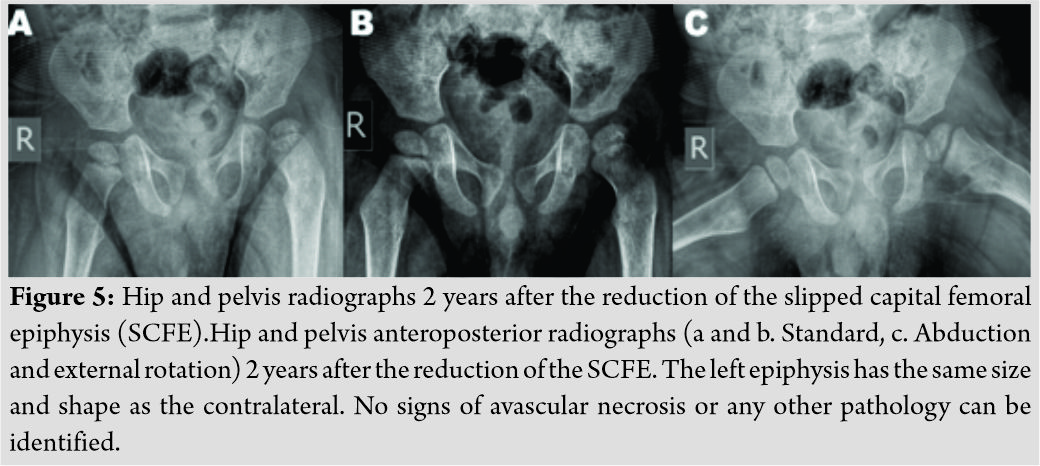
Approximately 6 h following his admittance to the hospital, the patient was transferred to the operating theater. Under general anesthesia, a gentle closed reduction was attempted, applying traction along the longitudinal axis of the limb and then internal rotation [8]. Successful reduction was confirmed with the use of a c-arm image intensifier and a hip spicacast with an anti-rotation bar was applied next (Fig. 3). On the next day, and because the patient continued to manifest epileptic seizures, despite the fact that he was receiving his usual treatment, he was transferred to the pediatric department, from where he was uneventfully discharged 4 days later.
The patient was followed up at our outpatients’ clinic every week for the 1stmonth and then every 15 days for another month. The spicacast was removed at 8 weeks (Fig. 4). Physical examination at this stage revealed a painless hip with a full range of motion. The patient’s physiotherapy and passive kinesiotherapy routine resumed at 6-month post-reduction. Despite the fact that he was not able to walk (and remained non-ambulatory on his latest follow-up visit) suffering from severe psychomotor dysfunction in the context of epileptic encephalopathy, painless hip range of motion was retained during all follow-up visits throughout the next 22 months. Consecutive follow-up radiographs obtained during the follow-up period, revealed good remodeling of the proximal femur and a femoral head with spherical contour and with no signs of avascular necrosis or chondrolysis (Fig. 5). An MRI scan at 2 years post-reduction showed normal shape and size of the affected femoral head, with no signs of physeal arrest and/or avascular necrosis (Fig. 6). Nevertheless, the child is under a tight follow-up schedule and it will remain under close observation until he has reached skeletal maturity.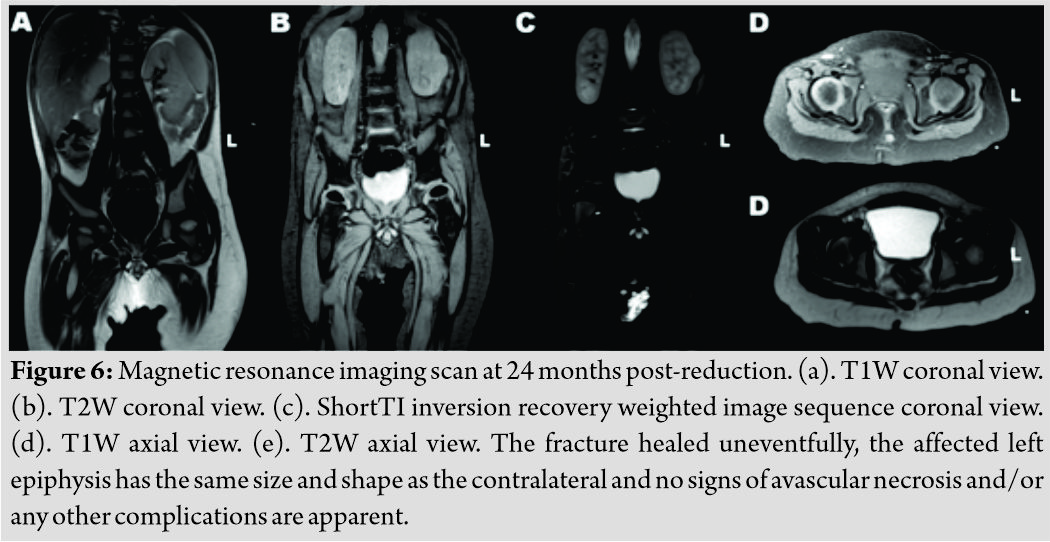
Discussion
SCFE is a hip condition, usually affecting older children and adolescents during a period of rapid growth [9]. This rather infrequent condition is manifested even more rarely in children younger than 10yearsold. Slippage in this group of patients is often associated with obesity, endocrine or metabolic disorders, septic arthritis, radiation therapy, and trauma [1,3,10,11]. The standard treatment of choice for SCFE is operative. Surgical options include bone peg epiphysiodesis, in situ fixation (either with smooth Steinmann pins or a screw), closed reduction and pinning and less commonly hip dislocation with subsequent realignment and fixation of the epiphysis and open or arthroscopic osteochondroplasty, and proximal femoral osteotomy [12, 13, 14]. Hip spicacast was found to be the treatment with the worst results, with rates of avascular necrosis up to 9%, chondrolysis up to 20.5%, and osteoarthritis up to 53%. As a result, this treatment modality has largely been abandoned in the management of SCFE [14]. Prophylactic treatment of the contralateral hip is often advocated since bilateral idiopathic adolescent SCFE may occur in up to 25% of cases. Alternatively, the young patient is closely followed-up until epiphyseal maturation has been achieved, and immediate operative intervention takes place, should SCFE is manifested in the contralateral hip as well[12,14]. We report the first– to the best of our knowledge–case in the English literature, of non-traumatic SCFE occurring in a 10-month-old infant. Taking the patient’s age and medical history into consideration, as well as the fact that he was in a “pre-walking” stage of development, and following consultation with the pediatric neurologist who was responsible for his treatment, we decided to follow a non-operative treatment plan. These were also the reasons we decided to avoid any prophylactic intervention in the contralateral hip. SCFE was successfully reduced and the fracture healed uneventfully with the application of a simple spicacast. No signs of femoral head avascular necrosis and/or any other complications were noted 2 years post-reduction. The reader, however, should interpret these results with caution since SCFE in our case occurred in a very young infant and its pathogenetic mechanism was different from the one usually encountered in children of older age and adolescents. Although – with a few exceptions [15]– it is not currently indicated for the treatment of the vast majority of patients with SCFE, closed reduction and immobilization in a hip spicacast may be considered as an alternative treatment option in carefully selected patients.
Conclusion
This unique case of a 10-month-old infant who developed SCFE following an epileptic seizure shows that this rare fracture may occur even in very young children. Although it is not currently indicated for the treatment of the vast majority of patients with SCFE, closed reduction and immobilization in a hip spicacast may be considered as an alternative treatment option in carefully selected patients.
Clinical Message
SCFE may occur even in very young children, under unusual circumstances and due to non-well-established pathogenetic factors. Closed reduction and immobilization in a hip spicacast may be considered as an alternative treatment option in carefully selected patients with SCFE.
References
1. Papavasiliou KA, Kapetanos GA, Kirkos JM, Beslikas TA, Dimitriadou AS, Papavasiliou VA, et al. The pathogenetic influence of I-parathyroid hormone on slipped capital femoral epiphysis. Towards a new etiologic approach? J Musculoskelet Neuronal Interact 2003;3:251-7.
2. Nguyen D,Morrissy RT. Slipped capital femoral epiphysis: Rationale for the technique of percutaneous in situ fixation. J PediatrOrthop1990;10:341-6.
3. Papavasiliou KA, Kirkos JM, Kapetanos GA, Pournaras J. Potential influence of hormones in the development of slipped capital femoral epiphysis: A preliminary study. J PediatrOrthop B 2007;16:1-5.
4. Aronsson DD, Loder RT, Breur GJ, Weinstein SL. Slipped capital femoral epiphysis: Current concepts. J Am AcadOrthop Surg 2006;14:666-79.
5. Novais EN, Millis MB. Slipped capital femoral epiphysis: Prevalence, pathogenesis, and natural history. Clin OrthopRelat Res 2012;470:3432-8.
6. Jain P, Sharma S, Tripathi M. Diagnosis and management of epileptic encephalopathies in children. Epilepsy Res Treat 2013;2013:501981.
7. Prasad V, Kendrick D, Sayal K, Thomas SL, West J. Injury among children and young adults with epilepsy. Pediatrics 2014;133:827-35.
8. Leadbetter GW. A treatment for fracture of the neck of the femur. Reprinted from J bone joint surg 20:108-113, 1938. Clin OrthopRelat Res 2002;399:4-8.
9. Otani T, Kawaguchi Y, Marumo K. Diagnosis and treatment of slipped capital femoral epiphysis: Recent trends to note. J Orthop Sci 2018;23:220-8.
10. Azzopardi T, Sharma S, Bennet GC. Slipped capital femoral epiphysis in children aged less than 10 years. J PediatrOrthop B 2010;19:13-8.
11. Keenan WN, Clegg J. Idiopathic bilateral slipped upper femoral epiphyses in a child under six years of age. J Bone Joint Surg Br 1994;76:495-6.
12. Bittersohl B, Hosalkar HS, Zilkens C, Krauspe R. Current concepts in management of slipped capital femoral epiphysis. Hip Int 2015;25:104-14.
13. Kushare I, Wiltfong RE, Klingele KE. Acute, unstable slipped capital femoral epiphysis with associated congenital coxa vara. J PediatrOrthop B 2015;24:511-4.
14. Naseem H, Chatterji S, Tsang K, Hakimi M, Chytas A, Alshryda S, et al. Treatment of stable slipped capital femoral epiphysis: Systematic review and exploratory patient level analysis. J OrthopTraumatol2017;18:379-94.
15. Pinheiro PC. Nonoperative treatment of slipped capital femoral epiphysis: A scientific study. J Orthop Surg Res 2011;6:10.
 |
 |
 |
 |
 |
 |
| Dr. Papavasiliou Kyriakos | Dr. Stamiris Dimitrios | Dr. Stamiris Stavros | Dr. Zafeiriou Dimitrios | Dr. Tsiridis Eleftherios | Dr. Sayegh Fares |
| How to Cite This Article: Kyriakos P, Dimitrios S, Stavros S, Dimitrios Z, Eleftherios T, Fares S. Non-traumatic Infantile Slipped Capital Femoral Epiphysis following an Epileptic Seizure – A Case Report. Journal of Orthopaedic Case Reports 2019 Sep-Oct; 9(5): 35-38. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


