
[box type=”bio”] Learning Point of the Article: [/box]
Entrapment of the anterior tibial artery and/or deep peroneal nerve is a risk with distal third tibia fractures.
Case Report | Volume 9 | Issue 5 | JOCR September – October 2019 | Page 51-54 | Laura Lewallen, Adam Theissen, Daniel J Sucato. DOI: 10.13107/jocr.2019.v09i05.1530
Authors: Laura Lewallen[1], Adam Theissen[1], Daniel J Sucato[1]
[1]Department of Orthopaedic Surgery, Texas Scottish Rite Hospital for Children, 2222 Welborn Street Dallas, TX 75219, USA
Address of Correspondence:
Dr. Daniel J Sucato,
Texas Scottish Rite Hospital for Children 2222 Welborn Street Dallas, TX 75219.
E-mail: dan.sucato@tsrh.org
Abstract
Introduction: Arterial injury/entrapment is an uncommon sequelae of long bone fractures, particularly in closed injuries. The proximity of the anterior tibial artery to the distal tibia poses a risk of entrapment with a fracture at this level. To the best of our knowledge, this is the first case report of a partial nonunion due to entrapment of the anterior tibial artery in a healed tibia fracture in a pediatric patient.
Case Report: We describe a case of a 16-year-old male who presented with leg pain 2 years after a left distal third oblique tibia fracture. The fracture was initially treated non-operatively with excellent alignment. He did well for many months and returned to playing football with some vague persistent discomfort in his leg. Two years after the original injury, he was hit while playing football and started experiencing increasing left leg pain. The subsequent evaluation and findings are outlined here.
Conclusion: This is an original case report of an adolescent patient with a partial tibial nonunion requiring surgical intervention. Possible entrapment of neurovascular structures should be considered when managing these patients following injury.
Keywords: Case report, tibial nonunion, arterial entrapment.
Introduction
Arterial injury/entrapment is an uncommon sequelae of long bone fractures, particularly in closed injuries [1, 2, 3]. The proximity of the anterior tibial artery to the distal tibia poses a risk of entrapment with a fracture at this level [4, 5].This is particularly true in younger patients, with greater healing and remodeling potential, and, therefore, callus formation at the fracture site. There are two previous reports of similar cases, both of whom were adult patients. Miki et al. presented a case of an adult with a spiral distal third fracture, with entrapment of the calcified vessels within the fracture site (identified on computed tomography [CT] images) [6].
Case Report
Our patient is a 16-year-old otherwise healthy male who sustained an injury to the left leg while playing football, 2 years before presentation. He was found to have a left distal third oblique tibia fracture (Fig. 1) and was splinted in an outside emergency department that evening. Soon after, he was transitioned to a cast which remained in place for 6 weeks, and then to a boot for an additional 4 weeks. The patient then returned to playing football and did well, with mild occasional symptoms of aching pain for approximately 2 years. Two years after the initial injury, the patient was tackled from the side while playing football. He had immediate pain in the left tibia in the same location of the previous fracture. The pain persisted for approximately 6 months. It was localized to the site of the prior tibia fracture and extended to the anterior aspect of the foot. The patient also noted occasional numbness and tingling in the tips of his toes. Initial assessment at the time of presentation to our institution showed the left lower extremity to be grossly normal in appearance, with no swelling or deformity. The patient had tenderness to palpation along the left distal tibia. He had no neurologic deficit, with normal motor and sensory function throughout the lower extremities. Vascular exam was also normal. Radiographs showed an apparent channel in the lateral aspect of the distal tibia, consistent with a partial nonunion; however, the remainder of the fracture appeared well-healed (Fig. 2). A CT scan was obtained for further evaluation and showed a tubular channel running through the lateral cortex of the distal third of the tibia, at the previous fracture site (Fig 3). The appearance was consistent with entrapment of the neurovascular bundle, warranting further imaging with an magnetic resonance imaging (MRI) (Fig. 3).
MRI demonstrated the anterior tibial artery and deep peroneal nerve embedded within the lateral distal tibial cortex (Fig. 4). Given the patient’s persistent pain at the fracture site and concern for entrapment of the neurovascular bundle in the setting of partial nonunion, surgical intervention was offered. The decision was made to proceed with exploration and removal of the neurovascular bundle from within the cortical bone. We discussed that if the artery appeared to be coursing through the bone, it would likely not be functional. Given his foot remained well perfused, bypass was not planned (even if the anterior tibial artery was nonfunctional). A longitudinal incision was made along the distal third of the anterior tibial crest of the left leg. Sharp dissection was carried down through the floor of the anterior tibialis tendon sheath. The periosteum was elevated using a Cobb elevator, to expose the anterior tibial artery and deep peroneal nerve. Exploration of the deep peroneal nerve showed it to be adherent to the periosteum, but not encased within the bone. The nerve was mobilized and neurolyzed throughout the entire zone of injury. The nerve was protected for the remainder of the procedure. The anterior tibial artery was encased in bone, entering the tibial cortex approximately 9 cm above the tibiotalar joint and exiting approximately 4 cm above the tibiotalar joint (Fig. 5).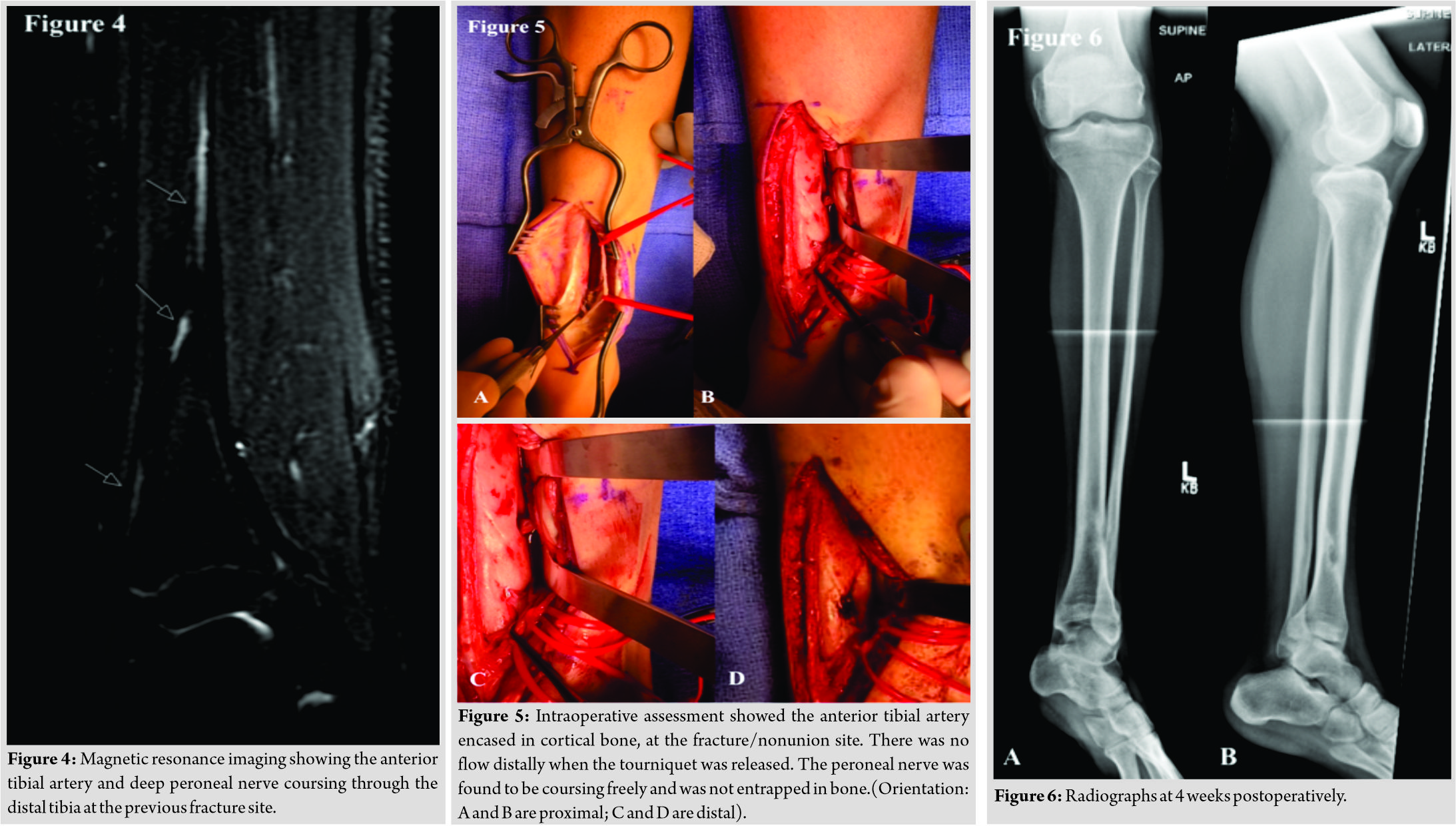
An osteotome was used to create a trough in the tibia, extending from the entrance and exit points of the anterior tibial artery. The artery was easily removed from the bone after creation of the trough and was left in continuity. The artery was found to be non-pulsatile when the tourniquet was released. The patient was placed in a soft dressing and allowed to weight bear as tolerated in a walking boot. The post-operative course was uncomplicated. The patient was seen at 6 weeks postoperatively. He reported significant improvement in his pain compared to preoperatively. He had been wearing the boot while out of the house. He had not yet returned to sporting activities. Examination at that time showed no motor or sensory deficits and a normal vascular exam. Radiographs showed the cortical defect along the lateral distal tibia with signs of ongoing healing at the fracture site (Fig. 6). The patient was allowed to gradually return to his activities. He will be seen again at 6 months postoperatively.
Discussion
Arterial injury/entrapment is an uncommon sequelae of long bone fractures, particularly in closed injuries. The proximity of the anterior tibial artery to the distal tibia poses a risk of entrapment with a fracture at this level. This is particularly true in younger patients, with greater healing and remodeling potential, and therefore callus formation at the fracture site. Hey et al. reported a case of deep peroneal entrapment in scar tissue around a proximal fibula fracture [7]; but to the best of our knowledge, this is the first case report of a partial nonunion due to entrapment of the anterior tibial artery in a healed tibia fracture in a pediatric patient. There are two previous reports of similar cases, both of whom were adult patients. Miki et al. presented a case of an adult with a spiral distal third fracture, with entrapment of the calcified vessels within the fracture site (identified on CT images) [6]. These authors cautioned that this situation should be kept in mind, particularly when considering reduction and fixation options, so as not to exacerbate the injury or cause further iatrogenic injury. Tan et al. reported a case of a 38-year-old woman with a closed, spiral fracture of the distal tibia. No neurologic deficit or vascular impairment was present at the time of injury [8]. The patient subsequently developed pain over the lateral aspect of the ankle with prolonged walking. She continued to have full, symmetric strength, and a normal neurovascular exam. Radiographs 10 months after the initial injury showed the fracture to be well healed, though with a cleft along the anterolateral aspect of the distal tibia. An MRI confirmed these findings and showed a partial nonunion of the fracture as well as entrapment of the neurovascular structures within the nonunion site. The patient was managed non-operatively. The authors emphasize the utility of MRI in confirming the diagnosis. It is important to note that in both of these reports, as in our case, the patient’s motor and neurovascular exam was normal. As described by Tytherleigh et al. and Gökkuş et al., a palpable dorsalispedis pulse does not reliably rule out anterior tibial artery injury as retrograde flow may produce a dorsalispedis pulse [9, 10].
Conclusion
Entrapment of the anterior tibial artery and/or deep peroneal nerve is a risk with distal third tibia fractures. Recognition of this injury is important. To the best of our knowledge, this is the first reported case in an adolescent patient and the first report in which the patient’s symptoms warranted surgical treatment. This was successful in removing the soft tissue structures allowing fairly rapid healing.
Clinical Message
Entrapment of the anterior tibial artery and/or deep peroneal nerve is a risk with distal third tibia fractures. Recognition of this injury is important.
References
1. Schmidt AH, Finkemeier CG, Tornetta P 3rd. Treatment of closed tibial fractures. Instr Course Lect 2003;52:607-22.
2. Court-Brown CM, McBirnie J. The epidemiology of tibial fractures. J Bone Joint Surg Br 1995;77:417-21.
3. Wedler V, Labler L, Köhler C, Guggenheim M, Künzi W, Trentz O. Iatrogenic neurovascular entrapment injuries caused by reduction and intramedullary fixation of fractures of the lower limb. Eur JTrauma 2006;32:381-6.
4. EbraheimNA, Lu J, Hao Y, Biyani A, Yeasting RA. Anterior tibial artery and its actual projection on the lateral aspect of the tibia: A cadaveric study. Surg RadiolAnat 1998;20:259-62.
5. Shah DM, Corson JD, Karmody AM, Fortune JB, Leather RP. Optimal management of tibial arterial trauma. J Trauma 1988;28:228-34.
6. Miki RA, Lawrence JP, Gillon TJ, Lawrence BD, Zell RA. Anterior tibial artery and deep peroneal nerve entrapment in spiral distal third tibia fracture. Orthopedics 2008;31:orthosupersite.com/view.asp?rID=32935.
7. Hey HW, Tan TC, Lahiri A, Wilder-Smith EP, Kumar VP, Kagda FH, et al. Deep peroneal nerve entrapment by a spiral fibular fracture: A case report. J Bone Joint Surg Am 2011;93:e113(1-5).
8. Tan ET, Tan TJ, Poon KB. Entrapment of the deep peroneal nerve and anterior tibial vessels by a spiral tibial fracture causing partial non-union: A case report. Skeletal Radiol 2016;45:551-4.
9. Tytherleigh MG, Charnley GJ, Wilkins DC. Closed rupture of the posterior tibial artery secondary to a soccer injury. Ann R Coll Surg Engl 1998;80:266-8.
10. Gökkuş K, Sagtas E, Comert N, Unal MB, Baloglu M. The changed route of anterior tibial artery due to healed fracture. Case Rep Vasc Med 2016;2016:5013013.
 |
 |
 |
| Dr. Laura Lewallen | Dr. Adam Theissen | Dr. Daniel J Sucato |
| How to Cite This Article: Lewallen L, Theissen A, Sucato D J. Partial Tibial Nonunion due to Entrapment of Anterior Tibial Artery: A Case Report. Journal of Orthopaedic Case Reports 2019 Sep-Oct; 9(5): 51-54. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


