
[box type=”bio”] Learning Point of the Article: [/box]
Why to consider synovial chondromatosis of the first metatarsophalangeal joint as a differential diagnosein a monoarticular synovitis of this joint, especially in refractory cases.
Case Report | Volume 9 | Issue 5 | JOCR September – October 2019 | Page 55-58 | Josep-Oriol Gimferrer-Arriaga, Javier Gascó-Adrien, Laura Perelló-Moreno, Matías J Esteras-Serrano. DOI: 10.13107/jocr.2019.v09i05.1532
Authors: Josep-Oriol Gimferrer-Arriaga[1], Javier Gascó-Adrien[1], Laura Perelló-Moreno[1], Matías J Esteras-Serrano[1]
[1]Department of Trauma and Orthopaedic Surgery, Hospital Universitari Son Llàtzer,Ctra. Manacor km 4, 07198, Palma de Mallorca, Spain.
Address of Correspondence:
Dr. Josep-Oriol Gimferrer-Arriaga,
Department of Trauma and Orthopaedic Surgery, Hospital Universitari Son Llàtzer, Ctra. Manacor km 4, 07198, Palma de Mallorca, Spain.
E-mail: oriolgimferrerarriaga@gmail.com
Abstract
Introduction: Synovial osteochondromatosis is a rare condition characterized by the formation of multiple cartilaginous nodules, which involves metaplastic changes of the synovium and is commonly found in larger joints. Occurrence in foot and ankle is uncommon, even less in metatarsophalangeal joints.
Case Report: A 54-year-old woman with primary synovial osteochondromatosis in the first metatarsophalangeal joint was treated by complete excision plus synovectomy. After 8years of follow-up, the patient remains symptom free with no recurrence observed. A summary of the case and review of all published cases found in the current literature around this location is discussed.
Conclusion: Though rare, synovial chondromatosis should be considered as a differential diagnosis in a refractory synovitis and tumor mass in the metatarsophalangeal joint of the hallux.
Keywords: Foot, metatarsophalangeal joint, soft tissue tumor, synovialchondromatosis.
Introduction
Synovial chondromatosis is an uncommon soft tissue tumor characterized by the formation of cartilaginous nodules. It usually occurs in the larger joints. It is rarely found around the foot and even less in the metatarsal and interphalangeal joints. We report a case of primary synovial chondromatosis in the first metatarsophalangeal joint of the foot in a 54-year-old patient. In literature, there are very few reports of synovial chondromatosis in these locations [1, 2, 3, 4, 5] and so the suspicion and diagnosis of this condition are challenging.
Case Report
Our patient is a 54-year-old woman, housewife, presented with a painful mass in the first webspace of her right foot, which had worsened progressively over the past 12 months. There was no previous history of trauma or any significant medical history or any family history of arthropathies. The onset of pain coincided with the detection of the mass and worsened steadily, eventually preventing her from carrying out basic activities of daily life.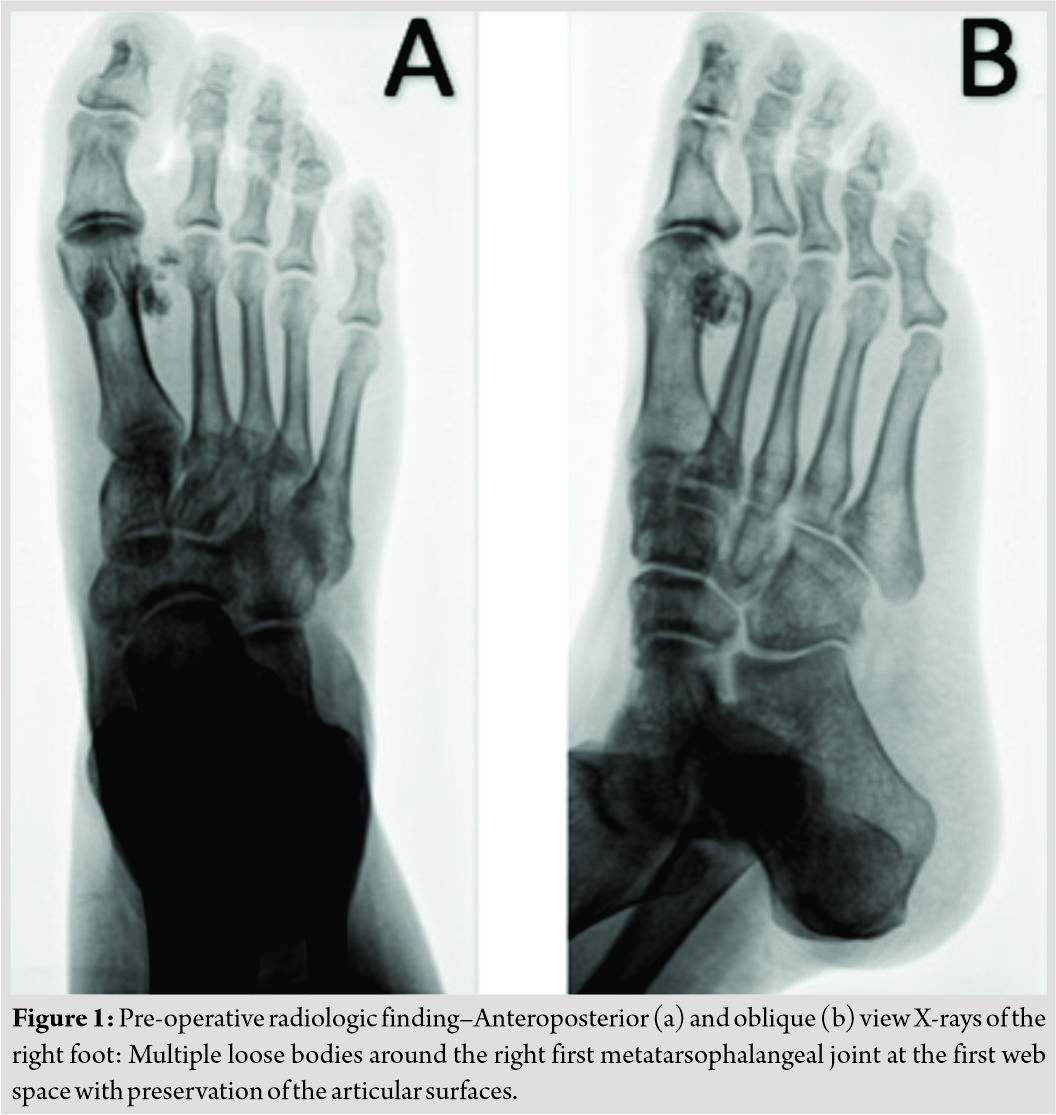
Examination confirmed a tender fixed mass on the dorsal aspect of the first webspace with slight swelling and no temperature or skin changes. The range of motion of the metatarsophalangeal joint was complete, although movement was painful in all positions. The rest of the examination was unremarkable. Plain radiographs of the foot showed multiple oval ossified lesions adjacent to the lateral side of the first metatarsal head in the first webspace, with bone remodeling of the first metatarsal head and a preserved joint line (Fig. 1). Computed tomography (CT)scan showed a multiple lobulated soft tissue mass with curvilinear calcification around the head of the first metatarsal (Fig. 2).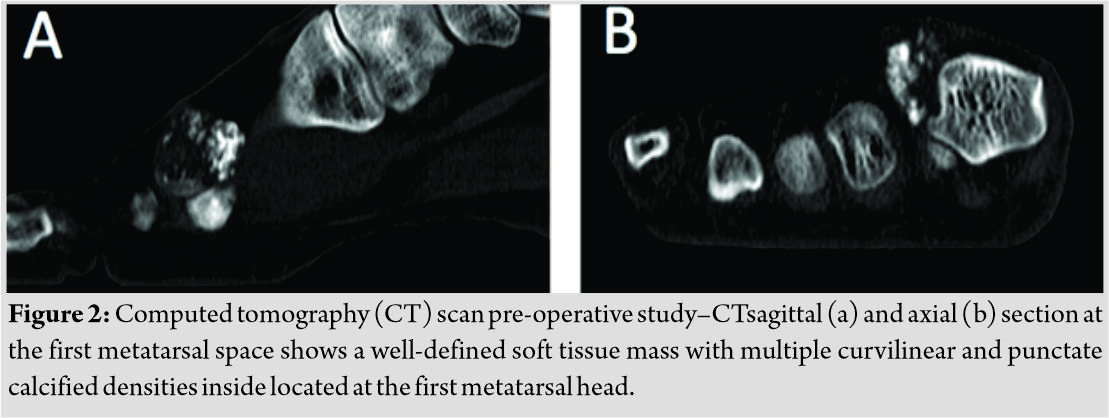
Coronal magnetic resonance (MR) imaging revealed multiple soft tissue masses, the largest one about 22×11mm in size with high signal on T1 in the first webspace. Small internal regions showed low signal on both T1 and T2. In view of the image study and the patient’s symptoms, surgical treatment was proposed. A complete resection of the bursa with all osteochondral bodies was performed under locoregional anesthesia (Fig. 3).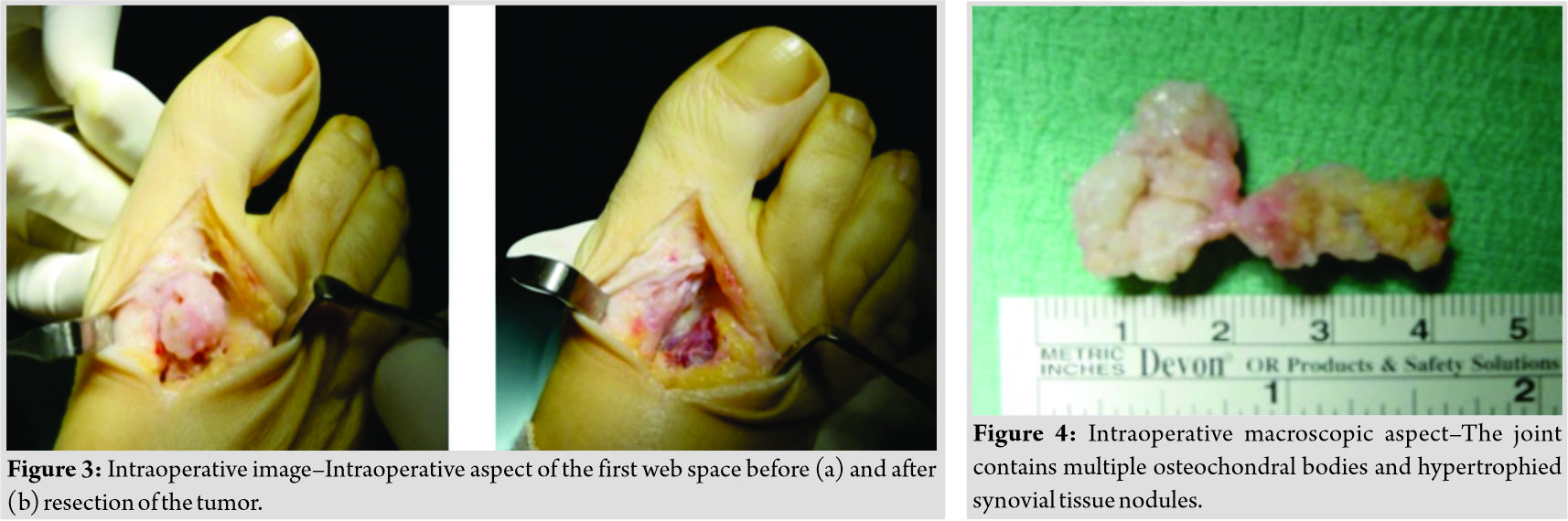 A partial synovectomy was also performed and the tissue sent for histological examination (Fig. 4), which subsequently confirmed the diagnosis of synovial chondromatosis (Fig. 5). After 8 years of follow-up, the patient remains satisfied with the result and is symptom free with no clinical or radiographic signs of lesion recurrence. She is able to carry out daily live activities without any difficulty.
A partial synovectomy was also performed and the tissue sent for histological examination (Fig. 4), which subsequently confirmed the diagnosis of synovial chondromatosis (Fig. 5). After 8 years of follow-up, the patient remains satisfied with the result and is symptom free with no clinical or radiographic signs of lesion recurrence. She is able to carry out daily live activities without any difficulty.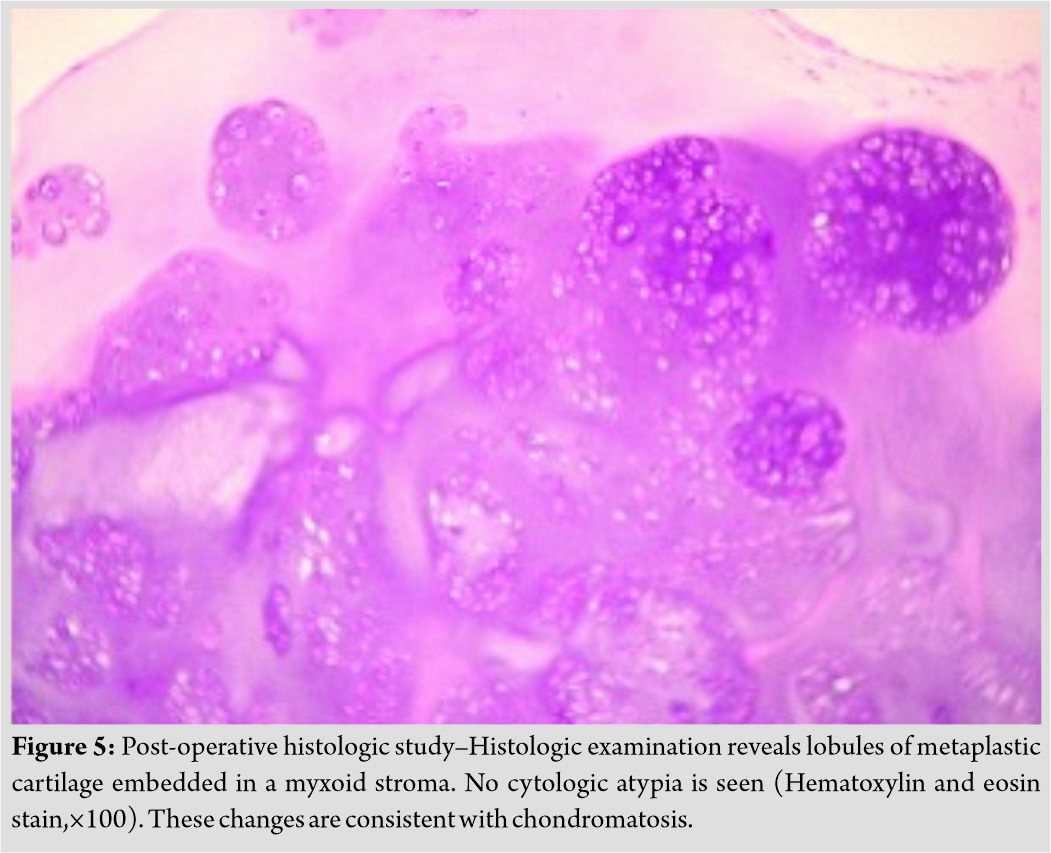
Discussion
For our literature review, we used the terms “synovial chondromatosis” and “foot” Mesh headings in a PubMed search. We reviewed all the articles found between 1986 and 2016 written in English and focused on the ones published in high impact factor reviews. We found only 10 reports of synovial chondromatosis affecting the forefoot: Three affecting interphalangeal [6, 7, 8] and seven metatarsophalangeal joints [1, 2, 3, 4, 5, 8, 9]. Of these seven cases, the first metatarsophalangeal joint was affected in five. Primary synovial osteochondromatosis is a rare idiopathic synovial proliferative disease. It is usually monoarticular and tends to occur between the third to fifth decades of life. It is more common in males (male:female ratio 4:2). Synovial osteochondromatosis may involve the synovial lining of the joint, tendon sheath, and bursa [10]. It has been widely reported in larger joints, with over 50% occurring in the knee [6]. Cases in the foot are rare. It has occasionally been described in metatarsophalangeal, interphalangeal, and talonavicular joints [1, 2, 3, 4, 5,7, 11]. Milgram classified chondromatosis in three phases depending on the activity of the synovitis and the presence of loose bodies, although the pathogenesis remains controversial [8, 12]. In literature, synovial chondromatosis is usually subdivided into primary and secondary disease, depending on the presence or absence of contributory factors such as osteoarthritis, rheumatoid arthritis, avascular necrosis, or osteochondral fracture. From the clinical perspective, previously reported cases in metatarsophalangeal joints show a notable similarity to ours, with the presence of slight swelling and tenderness around the joint without erythema or changes in the skin. In all cases, the affected joint presented full pain-free active and passive range of motion. Plain radiograph is useful if synovium calcification or loose bodies are present. However, between 5% and 33% are undetectable [11]. CT scan and MR imaging can both demonstrate the presence of loose bodies even before calcification and indicate the location and number to plan surgery. MR imaging also allows differential diagnosis with other masses that present calcification in the foot such as synovial hemangioma, synovial sarcoma, pigmented villonodular synovitis ossificans, lipomatous lesion, tumoral calcinosis, extraskeletal chondroma, and pseudomalignant osseous tumors [10, 13]. Due to the proximity of their location, the differential diagnosis should consider other conditions such as tenosynovial chondromatosis and soft tissue chondroma. The first one is regarded as the same process, with a similar morphology. The only difference is its location: Synovial chondromatosis is an intra-articular process while tenosynovial chondromatosis is extra-articular, arising from tenosynovial membranes. Soft tissue chondroma is also an extra-articular process with an anatomical distribution similar to tenosynovial chondromatosis, but it tends to form a periarticular solitary mass and has a different age distribution [14]. We include angioleiomyoma in the differential diagnosis in view of a case reported in our unit with initial suspicion of synovial chondromatosis, which was definitively diagnosed based on histopathological study of the resected mass. Surgery is the treatment of choice in this location, as this disorder may damage the joint. Full surgical exeresis of loose bodies and the affected synovium achieve good results. The techniques used in cases reported affecting the first metatarsophalangeal joint range from simple loose body removal to radical synovectomy, which achieves similar clinical results at 6–24 months of follow-up. Milgram recommended loose body excision in all cases associated with synovectomy only if the disease is active or transitional. However, the surgical strategy remains controversial [8]. Local recurrence rates vary depending on the series from 3% to 23% [6, 15] and seem to be related to a residually active synovium since complete synovium excision is not always possible. Malignant transformation, though extremely rare, has also been reported. Following surgical intervention, our patient has been completely symptom free for 8 years. Although the condition is benign and recurrence very unusual, considering the risk of malignancy reported in several cases, we continue to perform annual clinical and radiologic follow-up.
Conclusion
Synovial chondromatosis around the hallux is an uncommon disease, and it should be included as a differential diagnosis of monoarticular synovitis of the first metatarsophalangeal joint, especially in refractory patients.
The paucity of publications regarding suspicion and treatment of this rare soft tissue tumor makes it difficult to establish a concrete recommendation for management and follow-up. As no treatment protocol specific to the first metatarsophalangeal joint is described, experience contribution with more case reports may help to better understand this uncommon condition.
Clinical Message
Synovial chondromatosis is an uncommon soft tissue tumor that should be included in the differential diagnose of monoarticular synovitis of the first metatarsophalangeal joint, especially in refractory cases. Full surgical exeresis is the recommended treatment. The paucity of publications makes it difficult to establish a follow-up recommendation, as malignant transformation has been described.
References
1. Anract P, Katabi M, Forest M, Benoit J, Witvoët J, Tomeno B, et al. Synovial chondromatosis and chondrosarcoma. A study of the relationship between these two diseases. Rev ChirOrthopReparatriceAppar Mot 1996;82:216-24.
2. Brucher N, Faruch-Bilfeld M, Molinier F, Brouchet-Gomez A, Lapegue F, Sans N, et al. Primary synovial osteochondromatosis of the first interphalangeal joint of the foot: A case report. Diagn Interv Imaging 2014;95:451-3.
3. Chiang CH, Jou IM, Wang PH, Chern TC, Huang MT. Synovial osteochondromatosis of the second metatarsophalangeal joint: A case report. J Foot Ankle Surg 2011;50:458-61.
4. Fetsch JF, Vinh TN, Remotti F, Walker EA, Murphey MD, Sweet DE, et al.Tenosynovial (extraarticular) chondromatosis: An analysis of 37 cases of an underrecognized clinicopathologic entity with a strong predilection for the hands and feet and a high local recurrence rate. Am J Surg Pathol2003;27:1260-8.
5. Gulati A, Williamson DM. Synovial chondromatosis: A rare cause of a dislocated metatarso-phalangeal joint. Foot Ankle Surg 2010;16:e21-3.
6. Kenan S, Abdelwahab IF, Klein MJ, Lewis MM. Case report 817: Synovial chondrosarcoma secondary to synovial chondromatosis. Skeletal Radiol 1993;22:623-6.
7. Khan Z, Yousri T, Chakrabarti D, Awasthi R, Ashok N. Primary synovial osteochondromatosis of the first metatarsophalangeal joint, literature review of a rare presentation and a case report. Foot Ankle Surg 2010;16:e1-3.
8. Kim JB, Song IS, Shin SY, Yoon JY. Primary synovial chondromatosis of the talonavicular joint: A case report. Foot Ankle Surg 2016;22:e25-e28.
9. Matsuyama T, Suzuki T, Yoshida Y, Mori M, Tokuhiro S, Katayama N, et al. Synovial osteochondromatosis of the metatarsophalangeal joint of the great toe. Gan No Rinsho1986;32:1051-5.
10. McCarthy C, Anderson WJ, Vlychou M, Inagaki Y, Whitwell D, Gibbons CL, et al. Primary synovial chondromatosis: A reassessment of malignant potential in 155 cases. Skeletal Radiol 2016;45:755-62.
11. McKenzie G, Raby N, Ritchie D. A pictorial review of primary synovial osteochondromatosis. Eur Radiol2008;18:2662-9.
12. Milgram JW. Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
13. Galat DD, Ackerman DB, Spoon D, Turner NS, Shives TC. Synovial chondromatosis of the foot and ankle. Foot Ankle Int 2008;29:312-7.
14. Ryan JD, Garwood C, Lickiss J. Synovial chondromatosis surrounding the first metatarsophalangeal joint: A case report. Foot Ankle Spec 2016;9:174-8.
15. Lim SC, Kim YS, Kim YS, Moon YR. Extraskeletal osteochondroma of the buttock. J Korean Med Sci 2003;18:127-30.
 |
 |
 |
 |
| Dr. Josep-Oriol Gimferrer-Arriaga | Dr. Javier Gascó-Adrien | Dr. Laura Perelló-Moreno | Dr. Matías J Esteras-Serrano |
| How to Cite This Article: Gimferrer-Arriaga J, Gascó-Adrien J, Perelló-Moreno L, Esteras-Serrano M J. Synovial Chondromatosis in the First Metatarsophalangeal Joint: A Case Report of this Uncommon Condition and Review of Current Literature. Journal of Orthopaedic Case Reports 2019 Sep-Oct; 9(5): 55-58. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


