
[box type=”bio”] Learning Point of the Article: [/box]
Next to the approach to the posterior axillary fold, this article includes information about repairing the latissimus dorsi tendon with tension slide buttons.
Case Report | Volume 9 | Issue 5 | JOCR September – October 2019 | Page 82-86 | Malte Holschen, Maria Körting, Jörn Steinbeck, Kai-Axel Witt. DOI: 10.13107/jocr.2019.v09i05.1546
Authors: Malte Holschen[1], Maria Körting[2], Jörn Steinbeck[2], Kai-Axel Witt[2]
[1]Department of Orthopaedic Surgery, Raphaelsklinik, Loerstr. 23, 48143 Münster, Germany,
[2]Department of Orthopaedic Surgery, Orthopaedic Practice Clinic, Von-Vincke-Str. 14, 48143 Münster, Germany.
Address of Correspondence:
Dr. Malte Holschen,
Department of Orthopaedic Surgery, Fellow Physician, Raphaelsklinik, Loerstr. 23, 48143 Münster, Germany.
E-mail: holmal@web.de
Abstract
Introduction: Traumatic tears of the latissimus dorsi tendon (LDT) are a rare sports injury that may occur during exercises involving horizontal and vertical pulling. A standardized treatment algorithm for this injury does not yet exist.
Case Report: A 30-year old male CrossFit Athlete experienced sudden unbearable pain in his right posterior shoulder during a bar muscle-up exercise. The contour of his right posterior shoulder had changed immediately, and the patient could not do any more exercises involving his right shoulder. BMagnet resonance imaging (MRI) revealed an isolated tear of the LDT. The repair of the tendon was performed using a posterior approach in the lateral decubitus position. After arming the tendon with non-absorbable sutures it was reinserted onto the crest of the lesser tuberosity of the proximal humerus with two monocortical suture buttons. Postoperatively, the patient was immobilized with an abduction pillow for 6 weeks. After 9 months he reported a 90% function of his shoulder. MRI showed complete anatomical reinsertion of the LDT. The patient was able to master 15 pull-ups in a row.
Conclusions: Surgical repair of the LDT may achieve good functional results as well as an acceptable recovery period.
Keywords: Acute tendon tear, crest of lesser tuberosity, CrossFit, latissimus dorsi tendon, suture button.
Introduction
The latissimus dorsi muscle (LDM) is a large flat muscle originating from the mid to the lower back. The insertion of the latissimus dorsi tendon (LDT) is located at the crest of the lesser tuberosity of the proximal humerus posterior to the pectoralis major tendon and anterior to the teres major tendon. The most important functions are adduction, extension, and internal rotation of the shoulder. The LDM is strongly involved and trained during horizontal and vertical pulling exercises such asrowing and pull-ups. During exercises stressing the LDM, isolated ruptures of its tendon are possible. The bar muscle-up exercise (BMU) is a combination of a pull-up exercise and a dip exercise.The athlete hangs on a bar and combines both exercises in a swinging motion starting with the pull-up exercise. The LDT isgreatly stressed during this particular CrossFit exercise. Few case reports have dealt with traumatic tears of the LDT. Both surgical treatment and conservative treatment have been reported (1, 2, 3, 4, 4, 5, 6, 7, 8, 9).This is the first case report about a CrossFit athlete with an acute LDT tear who was operated using a minimal-invasive posterior approach in combination with tension-slide suture buttons.
Case Report
The patient of this case report is a semi-professional CrossFit athlete who takes part in national and international competitions. Since 10years, he trains 10–15 h weekly including weight-lifting, sport-specific exercises, and cardiovascular exercises. Before the injury of his LDT, he had not suffered from any tendon injury or other severe injuries. During the BMU, he experienced a sudden pain in his right shoulder. He was forced to stop his training right away. Regarding himself in the mirror, the patient noticed an altered contour of his right shoulder and his right upper back. The injury was detected2 days after the initial trauma using MRI.
Clinical findings
The patient was assessed clinically in our practice 4 days after trauma. The CrossFit athlete was 190 cm tall and his weight was 92 kg.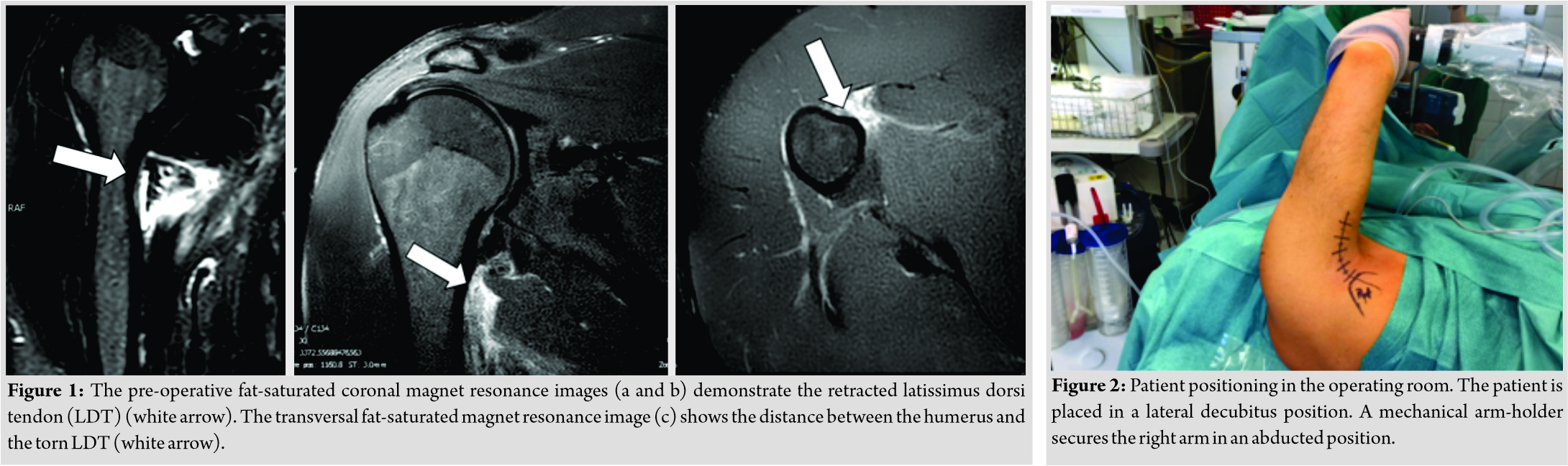 During palpation, the right LDM and region of the posterolateral aspect of the shoulder were tender. Active elevation and forward flexion measured 70° each. Active external rotation (30°) and internal rotation (buttock) were limited. Strong pain could be provoked manually by palpating the anterior axilla beneath the pectoralis major tendon.
During palpation, the right LDM and region of the posterolateral aspect of the shoulder were tender. Active elevation and forward flexion measured 70° each. Active external rotation (30°) and internal rotation (buttock) were limited. Strong pain could be provoked manually by palpating the anterior axilla beneath the pectoralis major tendon.
Pre-operative imaging
Preoperatively, the injury was assessed in coronal and transversal MRI scans. The images revealed a complete tear of the LDT tendon, while the rotator cuff, the teres major tendon, and the pectoralis major tendon were intact. The maximum retraction of the tendon in relationship to the crest of the lesser tuberositiy rated 8 mm. Fluid around the tear site could be observed in fat-saturated MRI sequences. Pre-operative MRI scans are presented in Fig. 1a-c.
Surgical treatment
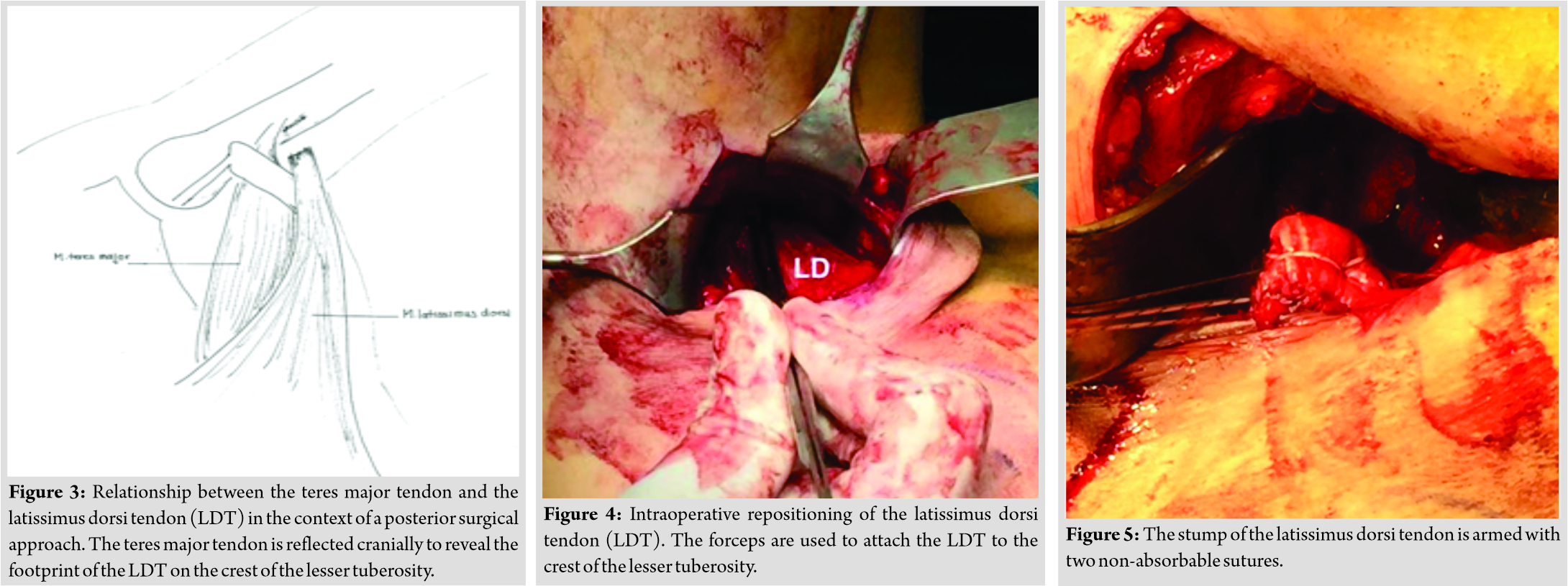
The patient was positioned in a lateral decubitus position on his left side. A mechanical arm-holder (Trimano Arthrex Inc., Naples, Florida) secured the right arm in a position of 90°abduction, neutral rotation (Fig. 2). A 10cmskin incision was made along the posterior margin of the deltoid muscle in the posterior axillary fold. After identification of the teres major muscle, the adhesions of the LDM were released and a Langenbeck retractor was inserted to lift the teres major muscle cranially to expose the insertion of the LDT (Fig. 3).Subsequently, the retracted stump of the LDT was identified and mobilized manually. A forceps was used to assess the tension of the LDT while moving it toward its insertion (Fig. 4, Video 1). Subsequently, the LDT was armed with two non-absorbable sutures (Fiber-Wire No. 2, Arthrex Inc., Naples, Florida), thus creating a proximal and a distal pair of suture limbs (Fig. 5 and 6). The crest of the lesser tuberosity was identified beneath the insertion of the teres major tendon and abraded to a bleeding surface with a rasp. The free ends of each paired suture were passed through the 12-mm tension slide button (Distal BicepsButton, Arthrex Inc., Naples, Florida) in an alternating fashion. After drilling two 3.2-mmmonocortical holes with a distance of 3 cm into the insertion of the LDT, the proximal and the distal button were inserted with the provided inserter. Pulling on the suture limbs flipped both monocortical buttons, thus preparing the tension-slide reinsertion of the LDT (Fig. 6). Afterward, the suture limbs were pulled tight and secured with seven half hitches for each button. After the procedure, the LDT showed an optimal attachment to its insertion.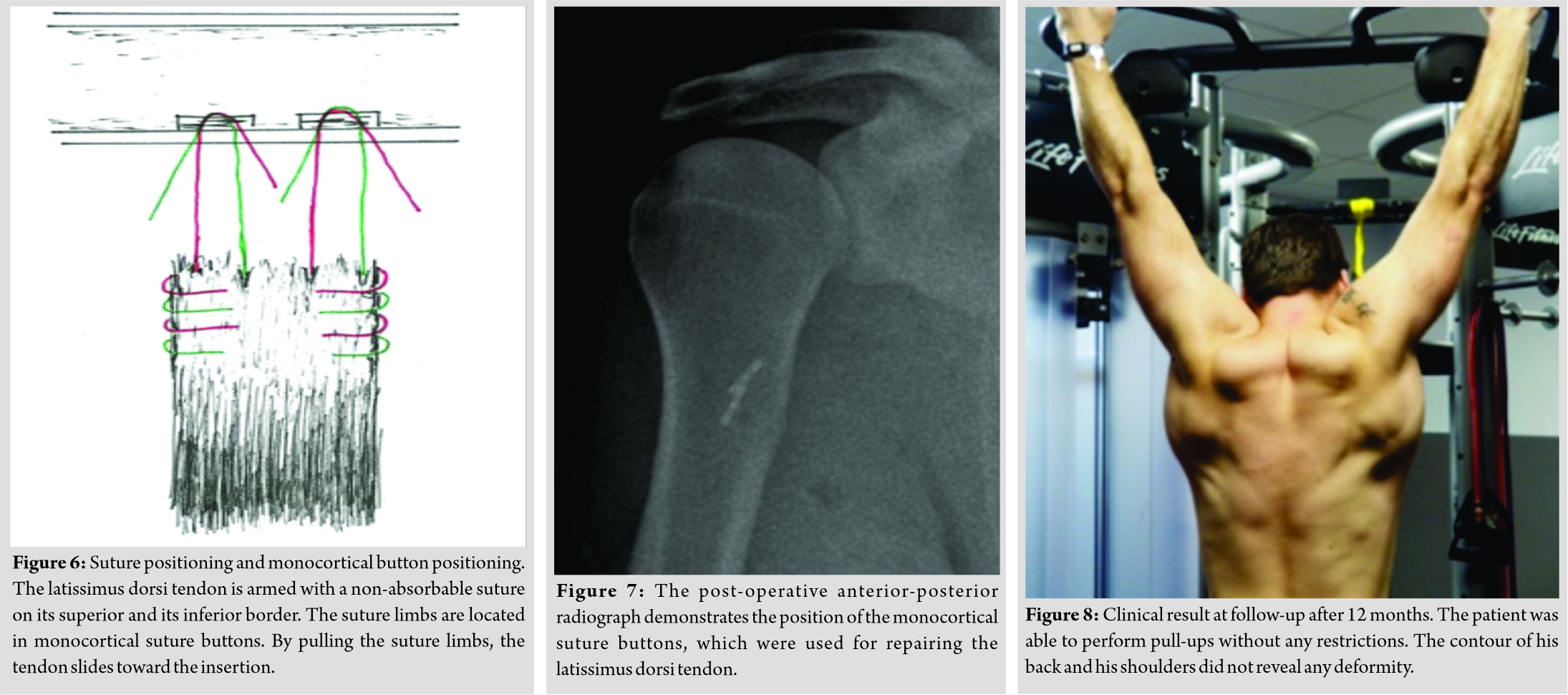 The post-operative radiograph demonstrated the position of the monocortical suture buttons in the humerus (Fig. 7).
The post-operative radiograph demonstrated the position of the monocortical suture buttons in the humerus (Fig. 7).
Post-operative rehabilitation
Postoperatively, the patient’s arm was immobilized using an abduction pillow for 6 weeks. After 3 weeks, the patient started passive physiotherapy with maximum abduction of 60° and external rotation until the neutral position. After 6 weeks, the patient started active exercises until 120° of abduction and 30° of external rotation. After 12 weeks, the range of motion was not restricted anymore. The patient was allowed to start active exercises with weights for the affected shoulder including the LDM. Six months after surgery, the patient was allowed to return to his previous semiprofessional sports level.
Follow-up assessment
Twelve months after the surgical procedure, the patient-rated his subjective shoulder value of the right shoulder with 90%. The patient did not report any rest pain or stress pain. The range of motion of the right shoulder was unrestricted. The patient was already able to perform most of his weight-lifting exercises and CrossFit exercises. (Fig. 8) demonstrates the athlete while doing a pull-up exercise in the gym.
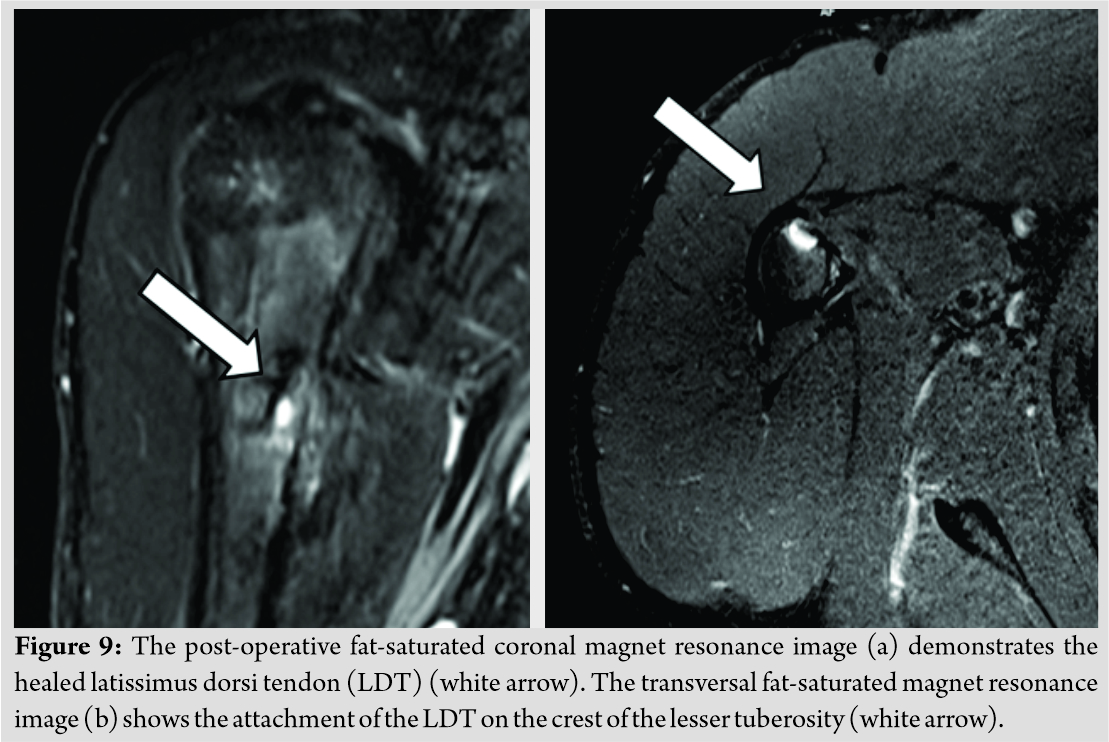
Follow-up MRI images revealed a healed LDT and an optimal position of the suture buttons (Fig. 9a and b).
The athlete wanted to take part in his next international tournament 2 months after a follow-up assessment.
Discussion
Although an isolated rupture of the LDT is a rare shoulder injury, reports about conservative and operative treatment have already been published [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11].
Standardized treatment recommendations do not exist. Operative management of LDT ruptures involves reattaching the LDT to the humerus through a combined anterior and posterior approach [7, 12], or a posterior approach [1, 4, 6]. We chose a posterior approach in the lateral decubitus position to be able to mobilize the LDM, if necessary. Both the approach and the patient positioning is recommendable and safe for an isolated repair of the LDT. Next to the reported approaches, the fixation techniques of other case reports differed from our technique. Most other authors used suture anchors [1, 4, 12], while Livesey et al. performed a transosseous fixation [7]. The monocortical tension-slide suture buttons, we used for the repair seem to be a safe and reproducible technique, which leads to an optimal tension of the superior and inferior border of the armed LDT. The visibility of the buttons during fluoroscopy or standard radiographs is beneficial, if a pull out of the implant is suspected. Since a loss of the whole LDM does not lead to a severely impaired shoulder function [13], the necessity of a surgical repair is debatable. In low-demand patients, conservative treatment should be favored, because of potential surgical risks. These risks involve injuries to the radial nerve and the axillary nerve as well as the posterior circumflex humeral artery, which are endangered during the surgical approach. Conservative treatment of LDT tears has been reported to be a valuable treatment option with some functional deficits, which hindered the affected patients to regain full recovery [11, 14, 15]. If the repair of the LDT is performed in cases of chronic lesions, a good functional outcome can be expected, too [1]. This is why the repair of an injured LDT should not always be performed immediately. Retracted LDT tears may be treated with delayed surgery in combination with an Achilles tendon allograft [16]. We informed our patients about the possibility of conservative treatment. Due to his high functional demands concerning his sport he refused conservative treatment. Although a very good clinical result was achieved in our patient, conservative treatment seems to be a reasonable alternative for this injury. Friedman et al. [8] reported a similar case of a CrossFit athlete who was treated conservatively. In this case, conservative treatment achieved a good functional result, but the patient was not able to perform muscle up exercises anymore, and the contour of his back showed an asymmetry. Demanding and complex sports like CrossFit may lead to a higher frequency of this particular injury in the future. The repair of the LDT with suture buttons using a posterior approach is a safe and reproducible procedure for this injury. Patients should be informed about the advantages and disadvantages of surgical and non-surgical treatment thoroughly. In high-demand athletes operative treatment seems to be advantageous.
Conclusion
Tears of the LDT may be treated conservatively or operatively. Both treatment options should be discussed thoroughly. While patients with high functional demands may only achieve a full recovery when treated operatively, patients with lower demands should be treated conservatively. Surgical treatment yields the risk for neurovascular injury and should be reserved for experienced surgeons.
Clinical Message
Sports with high physical demands such as CrossFit yield the risk for acute tears of the LDT. Acute pain and an altered contour of the affected shoulder are clinical findings for this injury. MRI should be employed to detect the injury. Repair of the LDT can be achieved using a posterior approach to the axilla.
References
1. Cox EM, McKay SD, Wolf BR. Subacute repair of latissimus dorsi tendon avulsion in the recreational athlete: Two-year outcomes of 2 cases. J Shoulder Elbow Surg 2010;19:e16-9.
2. Budoff JE, Gordon L. Surgical repair of a traumatic latissimus dorsi avulsion: A case report. Am J Orthop (Belle Mead NJ) 2000;29:638-9.
3. Henry JC, Scerpella TA. Acute traumatic tear of the latissimus dorsi tendon from its insertion. A case report. Am J Sports Med 2000;28:577-9.
4. Hiemstra LA, Butterwick D, Cooke M, Walker RE. Surgical management of latissimus dorsi rupture in a steer wrestler. Clin J Sport Med 2007;17:316-8.
5. Levine JW, Savoie FH 3rd. Traumatic rupture of the latissimus dorsi. Orthopedics 2008;31:799-801.
6. Lim JK, Tilford ME, Hamersly SF, Sallay PI. Surgical repair of an acute latissimus dorsi tendon avulsion using suture anchors through a single incision. Am J Sports Med 2006;34:1351-5.
7. Livesey JP, Brownson P, Wallace WA. Traumatic latissimus dorsi tendon rupture. J Shoulder Elbow Surg 2002;11:642-4.
8. Friedman MV, Stensby JD, Hillen TJ, Demertzis JL, Keener JD. Traumatic tear of the latissimus dorsi myotendinous junction: Case report of a crossfit-related injury. Sports Health 2015;7:548-52.
9. Celebi MM, Ergen E, Ustuner E. Acute traumatic tear of latissimus dorsi muscle in an elite track athlete. Clin Pract 2013;3:e15.
10. Ellman MB, Yanke A, Juhan T, Verma NN, Nicholson GP, Bush-Joseph C, et al. Open repair of retracted latissimus dorsi tendon avulsion. Am J Orthop (Belle Mead NJ) 2013;42:280-5.
11. Spinner RJ, Speer KP, Mallon WJ. Avulsion injury to the conjoined tendons of the latissimus dorsi and teres major muscles. Am J Sports Med 1998;26:847-9.
12. Ellman MB, Yanke A, Juhan T, Verma NN, Nicholson GP, Bush-Joseph C, et al. Open repair of an acute latissimus tendon avulsion in a major league baseball pitcher. J Shoulder Elbow Surg 2013;22:e19-23.
13. Mollenhoff G, Buchholz J, Mackowski S, Knopp W, Muhr G, Steinau HU. Muscle power and shoulder joint function after removal of the latissimus dorsi muscle. HandchirMikrochirPlastChir1994;26:75-9.
14. Butterwick DJ, Mohtadi NG, Meeuwisse WH, Frizzell JB. Rupture of latissimus dorsi in an athlete. Clin J Sport Med 2003;13:189-91.
15. Nagda SH, Cohen SB, Noonan TJ, Raasch WG, Ciccotti MG, Yocum LA. Management and outcomes of latissimus dorsi and teres major injuries in professional baseball pitchers. Am J Sports Med 2011;39:2181-6.
16. Aldosari SS, McRae SM, MacDonald PB. Surgical reconstruction of chronic latissimus dorsi tear using achilles tendon allograft. J Shoulder Elbow Surg 2016;25:e75-9.
 |
 |
 |
 |
| Dr. Malte Holschen | Dr. Maria Körting | Dr. Jörn Steinbeck | Dr. Kai-Axel Witt |
| How to Cite This Article: Holschen M, Körting M, Steinbeck J, Witt K. Traumatic Tear of the Latissimus Dorsi Tendon in a CrossFit Athlete: Surgical Management. Journal of Orthopaedic Case Reports 2019 Sep-Oct;9(5): 82-86. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


