
[box type=”bio”] Learning Point of the Article: [/box]
GCT of metacarpal bone although rare, can be successfully salvaged by tumor excision and reconstruction by fibular strut graft fixed with mini-recon plate, if detected early by MRI.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 11-14 | Ashok Kumar Gachhayat, Sanjeev Patnaik, Akshaya Kumar Sahoo, R R Karthik. DOI: 10.13107/jocr.2019.v09.i06.1566
Authors: Ashok Kumar Gachhayat[1], Sanjeev Patnaik[1], Akshaya Kumar Sahoo[1], R R Karthik[1]
[1]Department of Orthopaedics, Apollo Hospital, Bhubaneswar, Odisha, India.
Address of Correspondence:
Dr. Sanjeev Patnaik,
Department of Orthopaedics, Apollo Hospital, Bhubaneswar, Odisha, India.
E-mail: sportho1973@yahoo.co.in
Abstract
Introduction: Giant cell tumor (GCT) or osteoclastoma is an osteolytic, mostly benign but locally aggressive tumor occurring in young adults at the meta-epiphyseal region of long bones such as lower end of the femur, upper end of the tibia, and lower end of the radius, and proximal humerus in descending order of frequency. Only 2% of all GCT of bone occur in hand. GCT of metacarpal (MC) has different characteristics than that of other long bones. It has more aggressive behavior with involvement of entire length of MC with soft tissue extension.
Case Report: We are reporting a case of GCT of the 3rdMC in a 19-year-old female. She presented to us with a painful, firm, ovoid, and gradually progressive swelling measuring 4 cm × 3 cm over the dorsum of the left (non-dominant)hand, since past 6 months. Fine-needle aspiration cytology was suggestive of GCT of the tendon sheath. Pre-operative magnetic resonance imaging and computed tomography scan revealed the extent of the lesion with no neurovascular involvement. Although various reconstructive procedures to salvage the affected Ray have been reported in literature, we planned for a surgical resection of the lesion leaving behind 1 cm of healthy MC base which appeared to be normal radiologically and intraoperatively. Reconstruction of the defect was done using non-vascularized contoured fibular strut graft, fixed with 2.5 mm mini reconstruction plate, along with reconstruction of the collateral ligaments of the metacarpophalangeal joint. The histopathological study confirmed the diagnosis of GCT.
Conclusion: GCT of hand is a rare tumor, due to its relatively more aggressive behavior and high chance of recurrence it, nevertheless, provokes quite difficult issue to solve. Prognosis, treatment, and results are directly dependent on early diagnosis and adequate therapy.
Keywords: Giant cell tumor, 3rd metacarpal, surgical resection, fibular strut graft, 2.5mm mini reconstruction plate.
Introduction
Giant cell tumor(GCT) or osteoclastoma of the bone is a benign, locally aggressive osteolytic tumor which is relatively rare and has a high tendency of local recurrence [1]. There is a possibility of mainly pulmonary metastasis or transformation in a malignancy [2]. It usually affects the meta-epiphyseal region of long bones such as lower end of the femur, upper end of the tibia, and lower end of the radius, and proximal humerus in descending order of frequency [3]. GCT of bone accounts for about 4–9.5% of all primary tumors of bone [2]. GCT of hand is rare, accounting for 2–4% of all GCT [4]. Unni reports an incidence of 1.7% for GCT of metacarpals (MCs). Biscalgia has reported an incidence of 1% for GCT of the MC. Averill et al. reported an incidence of <1.5% in MC bones, while Huvos reported 3.7% and Mirra et al. 4% GCT of the hand, including MC bones [5]. GCT of MC has different characteristics than that of other long bones. It has more aggressive behavior with involvement of entire length of MC with soft tissue extension, due to limited free space and exquisite sensitivity of hand even a small hand produce significant swelling, pain, and dysfunction, and recurrence rate is higher as compared to other long bones even after wide resection and reconstruction [6]. It occurs predominantly in young people with more aggressive courses. It occurs commonly in adults between ages of 20 and 40 years with a female preponderance [2, 3]. In this report, we present a case of GCT of the 3rd MC of the left hand, which we treated with enbloc resection of tumor and reconstruction with autologous fibula strut graft, fixed with 2.5 mm mini reconstruction plate.
Case Report
A 19-year-old female presented with pain and swelling over dorsum of the left hand (non-dominant) overlying the 3rd MC for 6 months. The pain was spontaneous, insidious in onset, dull aching in nature; the swelling was ovoid in shape with well-defined margins and progressively increasing in size. There was also a painful restriction of movement of the 3rd metacarpophalangeal (MCP) joint. There were no H/O trauma, weight loss, and loss of appetite. There were no significant medical comorbidities.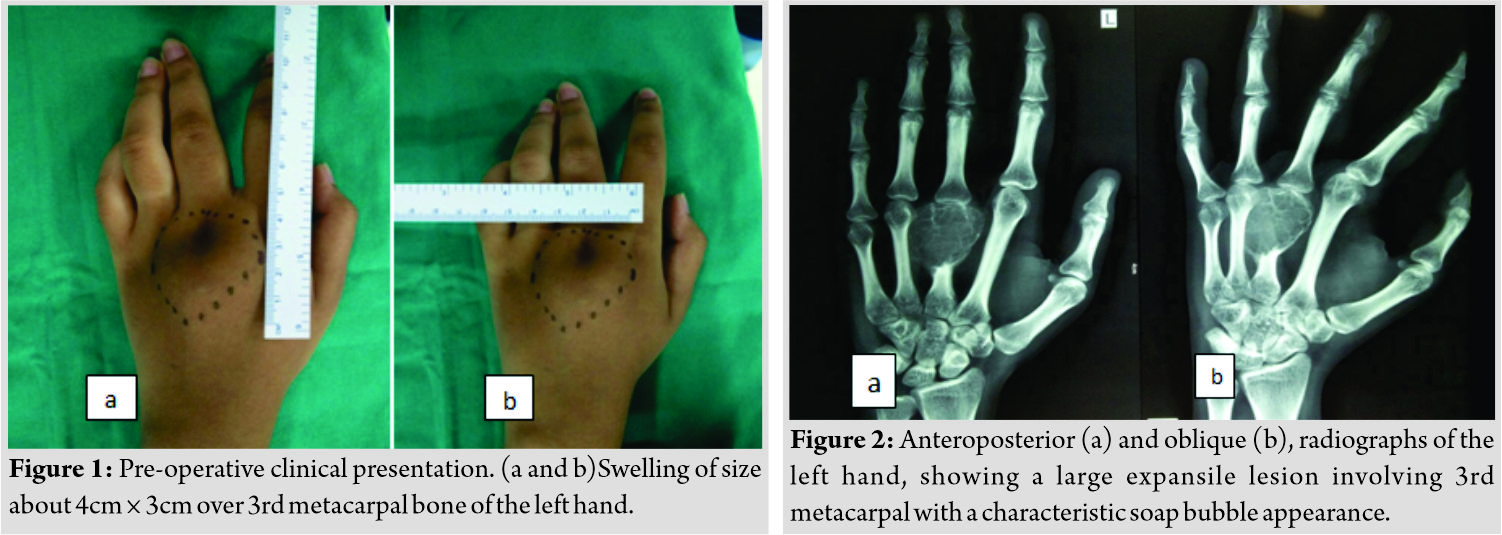
On physical examination, the swelling was of size 4cm × 3cm overlying left 3rd MC bone, firm in consistency, and painful on palpation. The overlying skin was normal (Fig. 1). The movement of MCP was painful and restricted. Routine lab parameters were within normal limits. The radiograph and magnetic resonance imaging (MRI) showed expansile lytic lesion involving the distal part including the head of the 3rd MC bone. Erosion of both anterior and posterior cortex with soft tissue component displacing the flexor and extensor tendon, but a periosteal reaction was lacking. The X-ray of the expansile lesion showed characteristic soap bubble appearance (Fig. 2 and 3).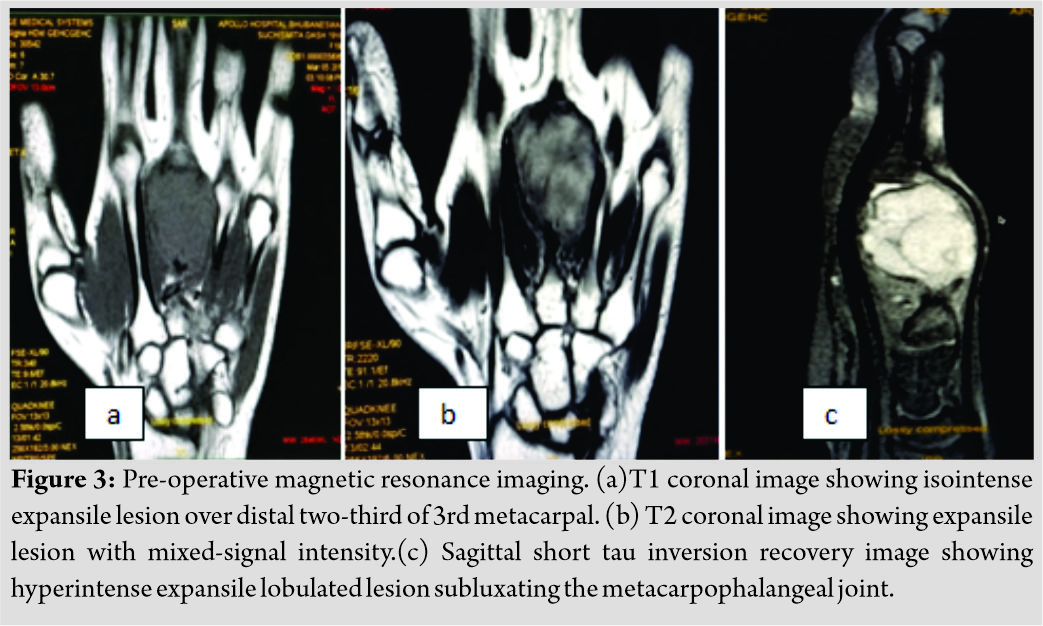
The patient underwent surgical excision of the mass under general anesthesia. The skin incision was given over the dorsal aspect longitudinally along the 3rd MC bone, meticulous soft tissue dissection was done, and underlying GCT mass was exposed in total. GCT mass was excised with margins along with partial osteotomy of the MC bone, leaving behind about 1cm healthy base of MC bone, which appeared normal both intraoperatively and radiologically (Fig. 4). Reconstruction of the defect was done using non-vascularized contoured fibular strut graft taken from ipsilateral middle one-third of fibula, fixed with 2.5 mm mini reconstruction plate, along with reconstruction of the collateral ligaments of the MCP (Fig. 5). Separate instrumentation was used for graft harvesting.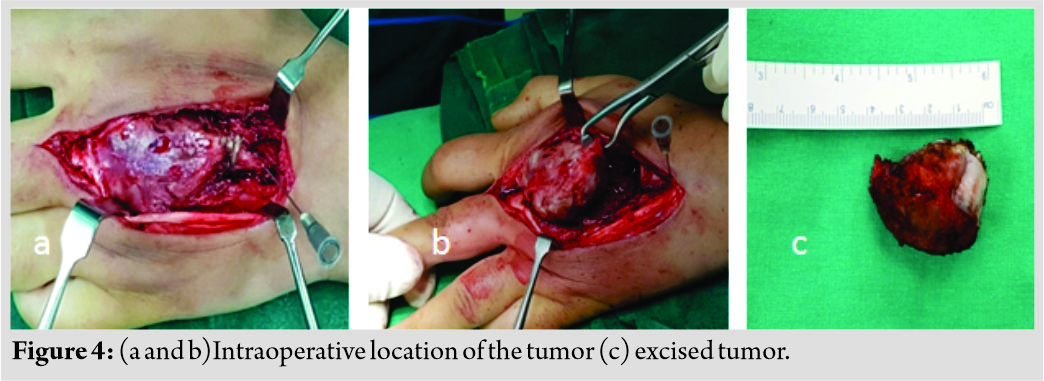
The excised mass was sent for histopathological study, which confirmed the diagnosis of GCT. The microscopic features showed circumscribed nodular neoplasm composed of diffusely scattered multinucleated osteoclastic giant cells, closely intermingled with plump fibroblast, and delicate blood vessels. The peripheral area showed mature bony trabeculae (Fig. 6). Postoperatively, the patient was given below elbow functional volar slab supporting upto the distal interphalangeal joint for 2 weeks followed by wrist splint for 2 more weeks with the initiation of range of motion exercises of fingers as per tolerance. The patient was followed up at regular intervals and at latest follow-up of 2 years that there was complete union of fibular autograft with no evidence of local recurrence, with an esthetically acceptable and functional hand (Fig. 7 and 8).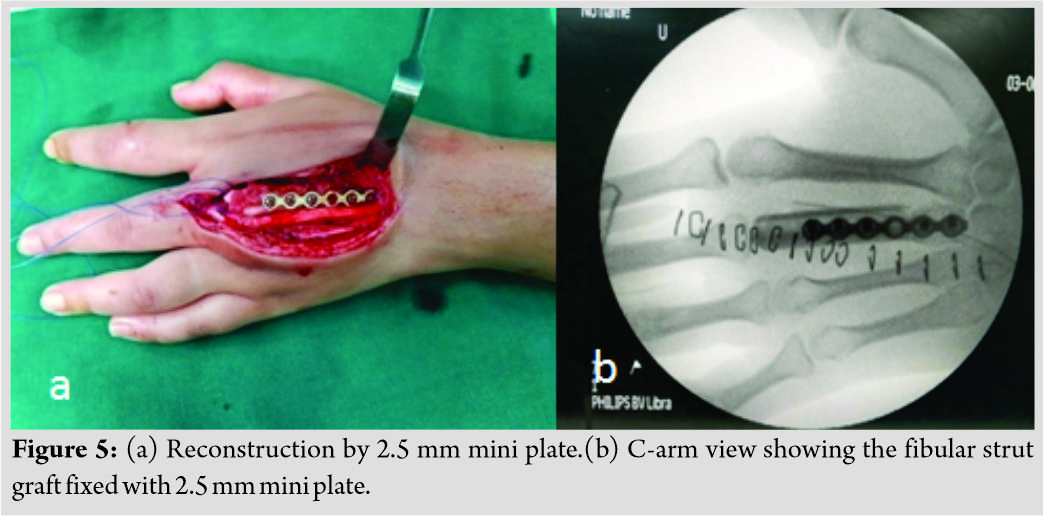
Discussion
GCT of bone affecting the hand is a rare lesion and is usually diagnosed at an advanced stage with a high rate of recurrence [2]. GCT is described as a predominantly osteoclastogenic stromal cell tumor of mesenchymal origin [7]. It is composed of three cell types, mainly neoplastic giant cells (tumor stromal cell), mononuclear monocytic cell, and multinucleated giant cell [7, 8].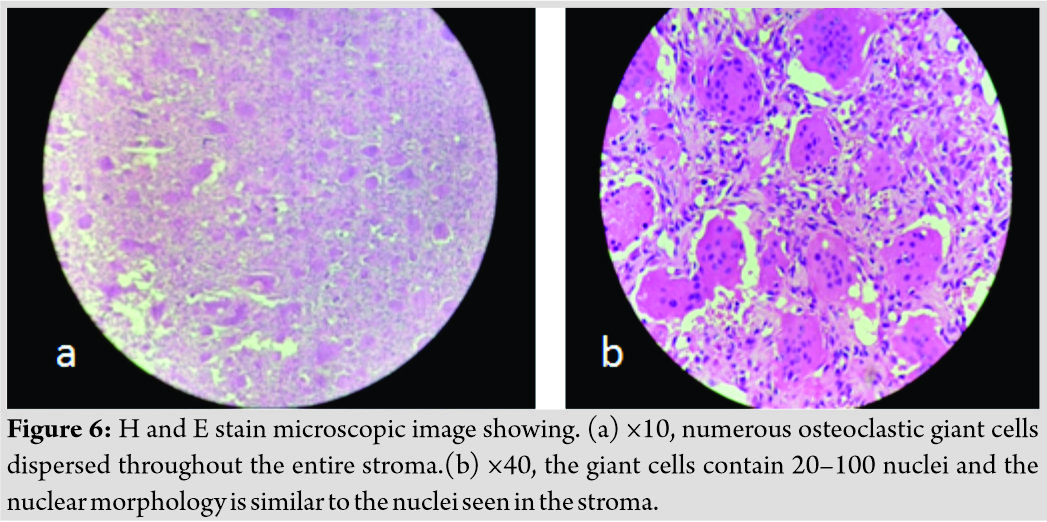
GCT of bone affecting the hand is a rare lesion and usually diagnosed in advanced stages and that of the 3rd MC is even a rarity. It recurs more rapidly in hand than at other locations. The metaphyseal region of MC and phalanges is a common site of origin in hand. The hand has limited free space and more sensitive so even a small mass can cause significant swelling, pain, and disability [3]. In 18% of cases of GCT of the hand, it is multicentric [3].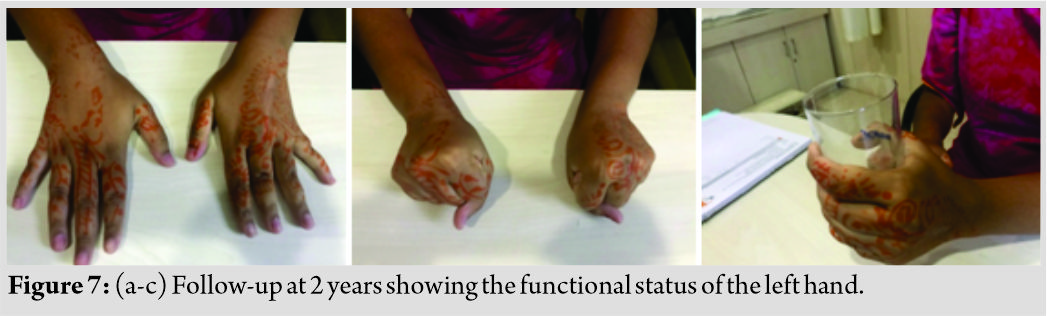
The radiological finding of GCT Includes well-defined lytic lesion, eccentrically located in the metaepiphyseal region of long bones, but in the hand, it tends to be more often central. The cortex is usually thinned without any periosteal reaction [9]. Campanacci et al. classified GCT of bones into three grades: Grade 1 has minimal cortical involvement; Grade 2 presents with thinned and bulged cortex; and Grade 3 has cortical breach with soft tissue involvement [2].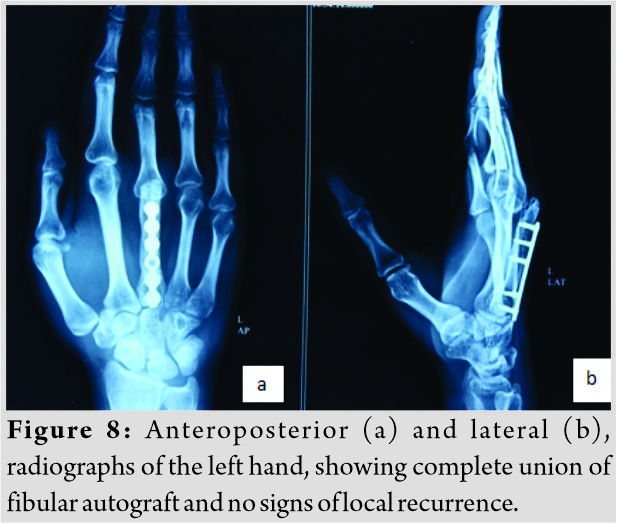
Computed tomography (CT) and MRI are essential in evaluating and staging of GCT. CT is useful in the evaluation of cortical bone, especially the thinning of cortex, pathological fracture, periosteal reaction, and absence of matrix mineralization. In case of cortical breach and soft tissue involvement, MRI is superior to CT. MRI also helps detect the fluid-fluid level typical for aneurysmal bone cyst (ABC) as a differential diagnosis [2]. The macroscopic appearance is usually soft, fleshy, and light brown colour. On histologic examination, giant cells are seen uniformly distributed within a bland mononuclear round to oval stromal cell background. The detection of giant cells is not specific for the diagnosis of GCT [9]. Giant cells can also be found in ABC, chondroblastoma, brown tumors of hyperparathyroidism, non-ossifying fibroma, and giant cell granuloma [9, 10, 11]. Various treatment modalities of GCT of bone in the hand have been described such as curettage alone, curettage with or without different adjuvants, followed by packing the cavity with bone graft or methylmethacrylate bone cement; wide margin resection and reconstruction; amputation; and disarticulation [2]. According to the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology for bone cancer recommendations, for localized GCT of bone, if the tumor is resectable, excision of tumor is the primary option. If the tumor is resectable with unacceptable morbidity or unresectable, the options include serial embolization (primarily for tumors of the pelvis), denosumab, interferon, pegylated interferon, and/or radiotherapy [12]. In Stage 1 or 2 of GCT of bone, the standard treatment traditionally has been intralesional excision/curettage and autograft reconstruction by packing the cavity with morselized bone graft. Intralesional excision, however, carries the risk of leaving microscopic disease regardless of precised procedure. The reported incidence of local relapse with this technique is almost 40–60%. Chemicals such as phenol or cytotoxic agents like clorpactin have been instilled in the tumor bed to decrease the relapse. On the other hand, cryosurgery technique using liquid nitrogen to extend the curettage has a high incidence of local wound and bone complications. Cases in which the tumor bed is packed with methylmethacrylate have shown to decrease the relapse rate by generating local hyperthermia, which again induces necrosis of any neoplastic tissue left behind; also, the polymerization of methylmethacrylate may produce a local chemical cytotoxic effect. However, there is a risk of degeneration of the articular cartilage by placing the cement in the subchondral region. There are a limited studies and outcomes with the use of CO2 laser for cauterizing the tumor bed [3]. In Stage 3 GCT of bone, enblocresection of the involved region of bone is the recommended treatment to avoid recurrence. The reconstructive methods include: Prosthetic replacements, bony grafts placement sharvested from non-vascularized or vascularized fibula and from the iliac crest [2]. However, a high recurrence rate has been reported even after en bloc resection. In such cases, amputation of the entire X-ray of the hand is preferred. Rarely, in cases, when surgery is not feasible, radiotherapy could also be an alternative option [2]. GCT of bone could rarely metastasize in up to 10% of patients [13]. Most commonly, the metastases occur after repetitive local recurrences [2].
Conclusion
GCT of the hand is a rare tumor with isolated involvement of MCs, even rarer. Prognosis, treatment, and results directly depend on an early diagnosis and adequate therapy. Various treatment modalities have been described in literature, starting from the finger salvaging by different reconstruction techniques to Ray amputation. Reconstruction of the defect using non-vascularized fibular strut graft, fixed with 2.5 mm mini reconstruction plate, along with reconstruction of the collateral ligaments of the MCP joint is a viable option which preserves an aesthetically acceptable and functional hand but requires long-term follow-up for chances of recurrence.
Clinical Message
GCT of the MC bone is an extremely rare entity. Due to its higher propensity for recurrence and aggressive behavior, early diagnosis using CT and MRI helps in choosing a proper line of the management and is the key for any salvage options. Of the various reconstructive modalities, our method of tumor excision, along with reconstruction with non-vascularized fibular strut graft fixed with mini recon plate, offers a viable option to preserve a functionally and esthetically acceptable hand, especially in a young female.
References
1. Tarun PK, Harshavardan JK, Vijayaraghavan V. Giant cell tumour of mertacarpal an illustrative case report. IOSR J Dent Med Sci 2016;15:1-7.
2. Matev B, Georgiev H, Georgiev GP. Giant cell tumour of fourth mertacarpal: Case report and literature review. J Radiother Med Oncol 2012;17:73-7.
3. Shahid M, Varshney M, Maheshwari V, Mubeen A, Gaur K, Siddiqui M, et al. Giant cell tumour of first metacarpal bone. BMJ Case Rep 2011;2011:bcr0120113687.
4. Al Lahham S, Al Hetmi T, Sharkawy M. Management of giant cell tumor occupying the 5th metacarpal bone in 6 years old child. Qatar Med J 2013;2013:38-41.
5. Saikia KC, Bhuyan SK, Ahmed F, Chanda D. Giant cell tumor of the metacarpal bones. Indian J Orthop2011;45:475-8.
6. Sahu S. Reconstruction of metacarpal bone giant cell tumor by metatarsal bone. Int J Res Orthop2016;2:32-5.
7. Kim Y, Nizami S, Goto H, Lee FY. Modern interpretation of giant cell tumor of bone: Predominantly osteoclastogenic stromal tumor. Clin Orthop Surg 2012;4:107-16.
8. Werner M. Giant cell tumour of bone: Morphological, biological and histogenetical aspects. Int Orthop2006;30:484-9.
9. McEnery KW, Raymond AK. Giant cell tumor of the fourth metacarpal. AJR Am J Roentgenol1999;172:1092.
10. Kulenovic E. Giant cell tumor. Appl Radiol2008;37:37-9.
11. Unni KK, Inwards CY. Dahlin’s Bone Tumours. Philadelphia, PA: Lippincott Williams and Wilkins; 2010. p. 310-6, 333-40, 352-3, 364-8.
12. NCCN. Bone Cancer NCCN Guidelines (Version 1.2015). Available from: http://www.nccn.org. [Last accessed on 2014 Oct 02].
13. Davila JA, Amrami KK, Sundaram M, Adkins MC, Unni KK. Chondroblastoma of the hands and feet. Skeletal Radiol2004;33:582-7.
 |
 |
 |
 |
| Dr. Ashok Kumar Gachhayat | Dr. Sanjeev Patnaik | Dr. Akshaya Kumar Sahoo | Dr. R R Karthik |
| How to Cite This Article: Gachhayat A K, Patnaik S, Sahoo A K, Karthik R R. Giant Cell Tumor of Third Metacarpal: A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2019 Nov-Dec;9(6): 11-14. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


