
[box type=”bio”] Learning Point of the Article: [/box]
Despite rare and temporary, transient idiopathic osteoporosis is present in a small number of pregnant women and diagnosis is important in order to choose the correct treatment and avoid complications such as fractures, before or during childbirth.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 54-57 | Frederico Paiva, Nuno Simões, David Pereira, Nuno Borralho. DOI: 10.13107/jocr.2019.v09.i06.1586
Authors: Frederico Paiva[1], Nuno Simões[1], David Pereira[1], Nuno Borralho[1]
[1]Department of Orthopedics and Traumatology, Centro Hospitalar de Tondela-Viseu, E.P.E., Portugal.
Address of Correspondence:
Dr. Frederico Paiva,
Department of Orthopedics, Centro Hospitalar de Tondela-Viseu, E.P.E., Av. Rei Dom Duarte, 3504-509 Viseu, Portugal.
E-mail: fredpaiva87@hotmail.com
Abstract
Introduction: Idiopathic Transient Osteoporosis (ITO) is a rare entity that may occur during pregnancy, usually manifesting in the third trimester and is considered a diagnosis of exclusion. When present in the hip, it is usually characterized by joint pain, claudicating gait, and osteoporosis of the femoral head with preservation of the joint space. These early clinical and radiological signs may be confused with those of aseptic necrosis, infection, or bone tumors, making it important to exclude these differential diagnoses. Complete resolution of this condition is usually prolonged and may take anywhere from 6 months to 1 or 2 years.
Case Report: This article presents the case of a 48-year-old Caucasian pregnant woman who presented a non-traumatic left hip pain. After the exclusion of infectious and tumoral diseases, a diagnosis of a less probable transient idiopathic osteoporosis was suspected. Magnetic resonance imaging images after childbirth supported this diagnosis. She recovered clinically and imagiologically with no complications 2 years after delivery.
Conclusion: Rarely, hip pain during pregnancy can occur due to transient osteoporotic injuries in the proximal femur. It is more frequent during the third trimester and although it resolves spontaneously in the following months after childbirth, we should always be aware of these less likely diagnoses.
Keywords: Hip pain, pregnancy, transient osteoporosis.
Introduction
The cause for the occurrence of a decrease in bone density in pregnant women remains to be fully determined. It is believed that the increased load on the joints by the additional weight of the baby, increased calcium requirements, and hormonal changes that occur during pregnancy may have a cumulative effect on its appearance [1, 2, 3]. This finding is more often found in the proximal femur but may affect other anatomical locations such as the acetabulum, knees, astragalus, and even vertebral bodies [1, 4]. Radiography may show signs of decreased bone density in later phases, but magnetic resonance imaging (MRI) is the examination of choice to achieve a more accurate diagnosis [5, 6].
Case Report
This is a case of a caucasian 48-year-old woman, nulliparous, in the third trimester of pregnancy, who presented a nontraumatic progressive left hip pain. She had no relevant medical history, referred no usual medication (before or during pregnancy time), and no smoking or drinking habits. She recurred to the Emergency Room(ER) of São Teotónio’s Hospital – Viseu, in April 2012, with left thigh pain with a mechanical rhythm that began at the 8th month of gestation, with progressive exacerbation and no history of trauma, denied fever, or weight loss. Physical examination showed hip pain with flexion greater than 120° and with internal rotation, with no other complaints. There were no motor or sensory deficits in the limbs. The radiograph revealed an apparent area of hypotransparency of the femoral head (Fig. 1a) and the ultrasound showed presence of moderate joint effusion. She also performed blood tests with thyroid function and inflammatory markers which were normal. She was discharged and advised to initiate conservative treatment with no weight-bearing of the limb through gait with support of crutches and painkillers. She was kept under surveillance and continued her treatment as an outpatient. During surveillance a full rheumatoid and calcium metabolic profile was studied with no abnormal results. The delivery, considering the high risk of proximal femur fractures in these cases, was performed by C-section, electively, in May 2012, at 43 weeks of gestation and without complications. In the 2–3 weeks after childbirth, the patient remained symptomatic and repeated X-ray showing a small lithic zone (2 cm × 2 cm) circumscribed to the internal femoral head (Fig. 1b) and to attain further characterization of the lesion an MRI was performed (Fig. 2).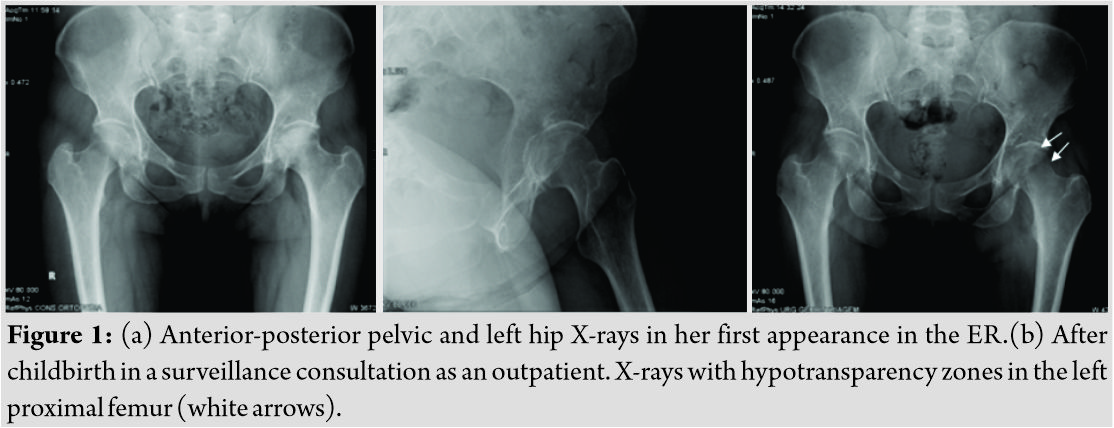 This examination reported a hyposignal zone in T1 and hypersignal in T2 of the femoral head and metaphyseal-diaphyseal transition of the left femur with a size of 3 cm ×4 cm and still free intra-articular fluid. A dual-energy X-ray absorptiometry (DEXA) evaluation was also performed in follow-up with her General Practitioner with femoral neck and lumbar spine T values of -2.8 and -2.1, respectively. After the exclusion of more probable diagnoses, the presence of transient pregnancy-related osteoporosis was considered more likely to be present, with vigilance and conservative treatment maintained.
This examination reported a hyposignal zone in T1 and hypersignal in T2 of the femoral head and metaphyseal-diaphyseal transition of the left femur with a size of 3 cm ×4 cm and still free intra-articular fluid. A dual-energy X-ray absorptiometry (DEXA) evaluation was also performed in follow-up with her General Practitioner with femoral neck and lumbar spine T values of -2.8 and -2.1, respectively. After the exclusion of more probable diagnoses, the presence of transient pregnancy-related osteoporosis was considered more likely to be present, with vigilance and conservative treatment maintained.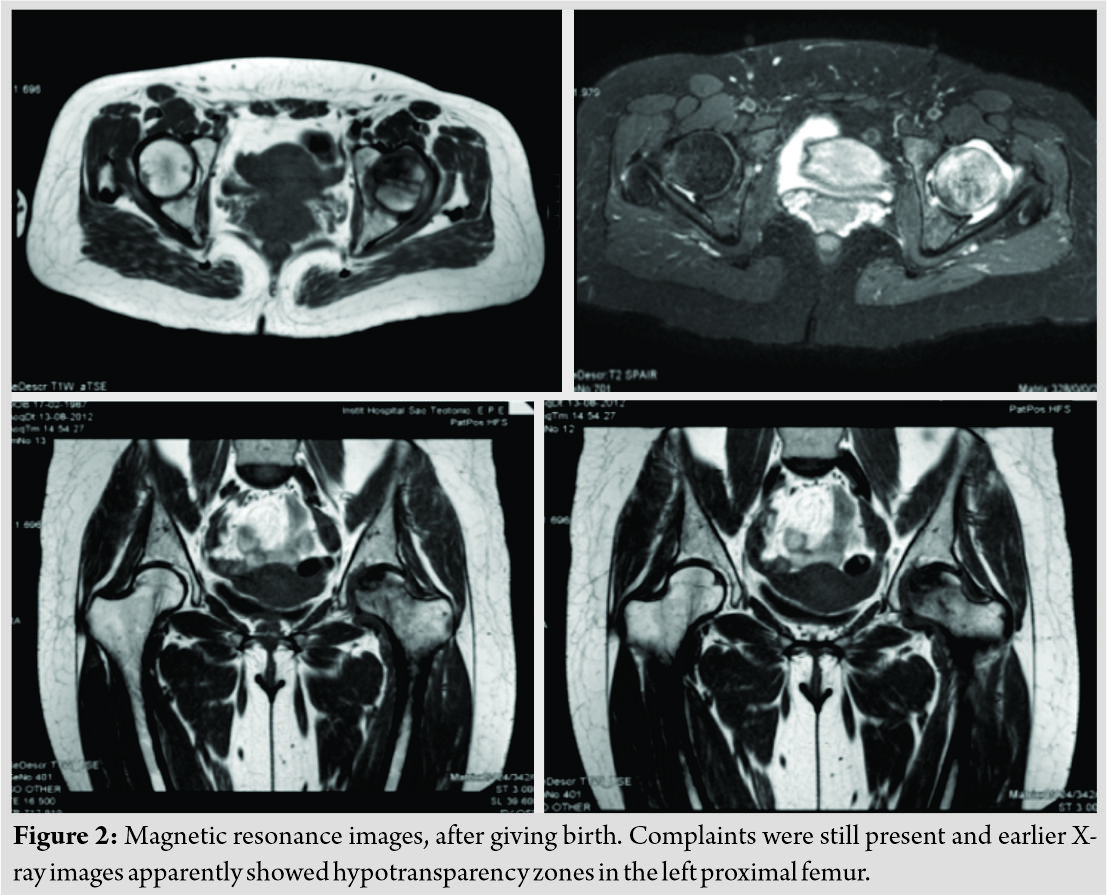
In February 2014 (20 months after childbirth), she presented a considerable improvement of the complaints, with good mobility/function of the left hip joint, with no need for walking aid, and with a second MRI revealing reduction of intra-articular free fluid and downsizing of the extensive signal change that affected almost the entire left femoral head, which had a size of 1 cm ×2 cm (Fig. 3). She maintained follow-up in our outpatient consultation with complete resolution of the initial clinical presentation in April 2014.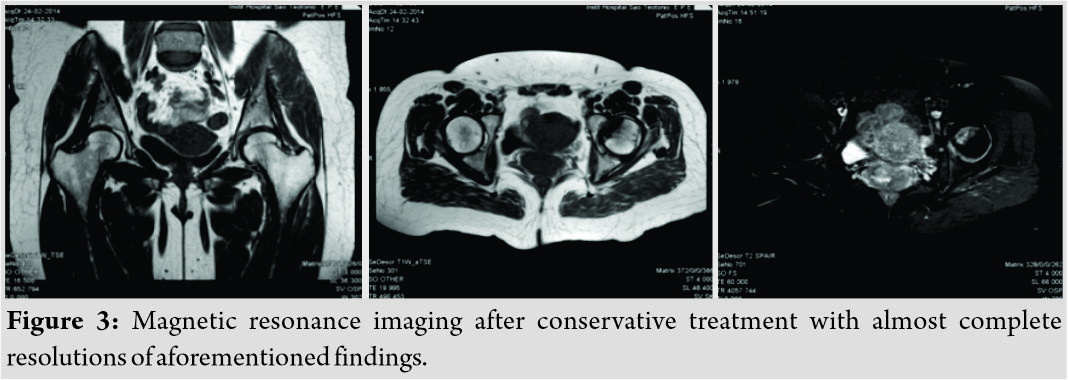
Discussion
Transient idiopathic osteoporosis is a pathology that affects mainly pregnant women, postpartum, or middle-aged men and is characterized by three phases with specific clinical and imaging characteristics. In Phase 1, the patient presents with hip pain and limitations in gait and may even limp. Radiography usually shows no changes and MRI reveals diffuse bone edema. In Phase 2, pain complaints deteriorate and imaging tests show areas of hypotransparency on radiography with joint space maintenance and presence of hyposignal lesions in T1 and hypersignal T2 in MRI, without femoral head collapse. In Phase 3, the complaints subside and MRI reveals a progressive improvement of the bone lesions in the following months [5, 7, 8, 9, 10]. In its early stages, it can be confused with other entities whose diagnosis depends on invasive examinations and, therefore, being aware of the initial symptoms and their progression can spare the patient from unnecessary procedures or therapies [11]. Among the main differential diagnoses are osteomyelitis, inflammatory/septic arthritis, neoplasias, stress fractures, and avascular necrosis. One of the complaints that help differentiate this pathology from osteonecrosis is the sudden onset of pain and improvement of these with rest, unlike the second case, in which the onset of pain is insidious and these do not improve with rest. At present, the suspicion of (ITO) in pregnancy it is the most sensitive and specific examination. In the images obtained, in addition to the aforementioned changes, the presence of diffuse medullary edema at a later stage and the absence of subchondral collapse helps to differentiate this pathology from avascular necrosis [5, 6, 12]. Laboratory tests do not usually have relevant changes. Although rare, fracture is possible and cases of bilateral hip fractures have been described more than once [13, 14, 15]. It may occur before or even during delivery without associated trauma. C-section is, in an attempt to lessen this probability, the best choice for childbirth. The initial treatment advised in cases of idiopathic osteoporosis includes rest, non-weight-bearing, and physiotherapy associated with analgesic or nonsteroidal anti-inflammatory drugs. The inclusion of a diet richer in calcium and the prescription of adjuvants such as Vitamin D and bisphosphonates have been shown to decrease complaints and accelerate the healing process [16, 17, 18]. Conservative treatment in the absence of a fracture reveals optimal results, and full resolution of the complaints is the usual outcome, usually 9 months to 1 year postpartum [19].
Conclusion
Hip pain can occur with relative frequency during pregnancy, especially in late phases and usually due to mechanical factors. Nonetheless, complete workouts and definitive diagnosis should be made if the symptoms continue. If the exclusion of more probable pathologies is made including osteonecrosis, septic arthritis, or even tumoral lesions, other less likely entities should be suspected such as transient osteoporosis. Idiopathic transient osteoporosisis a rare entity and although there is no clear evidence on its etiology, reports such as this describing its manifestation may contribute to the diagnostic sensitization and stimulate its study and the complete elucidation of its origin, evolution, and treatment.
Clinical Message
As in other orthopedic entities, when a certain patient presents with complaints, all diagnosis should be suspected, obviously with an order of probability. Pregnant women can likely present multiple pain disorders due to mechanical and hormonal factors, being hip pain one of them. As with nonpregnant women, multiple diagnoses can be considered, including more severe or emergent ones such as infectious articular disease, tumoral bone lesions, or avascular osteonecrosis. If these more frequent diagnoses are excluded, surveillance should always be maintained for a minimal amount of time to observe the degree of improvement with conservative treatment. If the complaints remain, other diagnosis and complementary workouts can be considered in pregnant women. MRI is the best examination to characterize the less likely diagnosis of transient idiopathic osteoporosis since it also shows distinct signs that in conjunction with clinical symptoms make the diagnostic suspension more accurate. The treatment consists of conservative measures with rest, painkillers, and partial/non-weight-bearing as tolerated. If the suspension is strong, C-section should be considered at childbirth since proximal femur fractures have been described during delivery.
References
1. Pallavi P, Padma S, Vanitha Anna Selvi D. Transient osteoporosis of hip and lumbar spine in pregnancy. J Obstet Gynaecol India 2012;62:8-9.
2. Mirza R, Ishaq S, Amjad H. Transient osteoporosis of the hip. J Pak Med Assoc 2012;62:196-8.
3. Scapinelli AC, Candiotto S, Scapinelli R. Reflex decalcifying algodystrophy of the hip in pregnancy (so-called transient osteoporosis). Review of the literature and four case reports. J Obstet Gynaecol 1997;17:134-8.
4. Swezey RL. Transient osteoporosis of the hip, foot and knee. Arthritis Rheum 1970;13:858-68.
5. Szwedowski D, Nitek Z, Walecki J. Evaluation of transient osteoporosis of the hip in magnetic resonance imaging. Pol J Radiol 2014;79:36-8.
6. Bloem JL. Transient osteoporosis of the hip: MR imaging. Radiology 1988;167:753-5.
7. Kumar R, House R. Idiopathic transient osteoporosis of the hip in pregnancy. Tex Med 1983;79:33-4.
8. Goldman GA, Friedman S, Hod M, Ovadia J. Idiopathic transient osteoporosis of the hip in pregnancy. Int J Gynaecol Obstet 1994;46:317-20.
9. Funk JL, Shoback DM, Genant HK. Transient osteoporosis of the hip in pregnancy: Natural history of changes in bone mineral density. Clin Endocrinol (Oxf) 1995;43:373-82.
10. Vaishya R, Agarwal AK, Kumar V, Vijay V, Vaish A. Transient osteoporosis of the hip: A Mysterious cause of hip pain in adults. Indian J Orthop 2017;51:455-60.
11. Marcucci G, Brandi ML. Rare causes of osteoporosis. Clin Cases Miner Bone Metab 2015;12:151-6.
12. Balakrishnan A, Schemitsch EH, Pearce D, McKee MD. Distinguishing transient osteoporosis of the hip from avascular necrosis. Can J Surg 2003;46:187-92.
13. Lidder S, Lang KJ, Lee HJ, Masterson S, Kankate RK. Bilateral hip fractures associated with transient osteoporosis of pregnancy. J R Army Med Corps 2011;157:176-8.
14. Bircher C, Afors K, Bircher M. Transient osteoporosis of the hip in pregnancy resulting in bilateral fracture of the neck of the femur. Int J Gynaecol Obstet 2012;116:176-7.
15. Sahan I, De Deken J, Anagnostakos K. Bilateral femoral neck fracture in a postpartum woman: Beware of the risk factors. Case Rep Orthop 2019;2019:4.
16. Schapira D, Braun Moscovici Y, Gutierrez G, Nahir AM. Severe transient osteoporosis of the hip during pregnancy. Successful treatment with intravenous biphosphonates. Clin Exp Rheumatol 2003;21:107-10.
17. Arayssi TK, Tawbi HA, Usta IM, Hourani MH. Calcitonin in the treatment of transient osteoporosis of the hip. Semin Arthritis Rheum 2003;32:388-97.
18. Agarwala S, Vijayvargiya M. Single dose therapy of zoledronic acid for the treatment of transient osteoporosis of hip. Ann Rehabil Med 2019;43:314-20.
19. Siva S, Roach V. Transient osteoporosis of the hip in pregnancy. Aust N Z J Obstet Gynaecol 1997;37:261-6.
 |
 |
 |
 |
| Dr. Frederico Paiva | Dr. Nuno Simões | Dr. David Pereira | Dr. Nuno Borralho |
| How to Cite This Article: Paiva F, Simões N, Pereira D, Borralho N. Idiopathic Transient Osteoporosis during Pregnancy – Report of a Clinical Case. Journal of Orthopaedic Case Reports 2019 Nov-Dec; 9(6): 54-57. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


