
[box type=”bio”] Learning Point of the Article: [/box]
In small children, with odontoid synchondrosis fractures associated with significant displacement and angulation, posterior C1-C2 fusion is a better option providing more stability. Furthermore, one can expect significant remodeling of the fracture within this population.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 62-64 | Narendra Reddy Medagam, Charanjit Singh Dhillon, Chetan Shashikant Pophale, Nilay Prafulsinh Chhasatia, Anandkumar Khatavi. DOI: 10.13107/jocr.2019.v09.i06.1590
Authors: Narendra Reddy Medagam[1], Charanjit Singh Dhillon[1], Chetan Shashikant Pophale[1], NilayPrafulsinh Chhasatia[1], Anandkumar Khatavi[1]
[1]Department of Spine Surgery, MIOT Hospital, Chennai, Tamil Nadu, India.
Address of Correspondence:
Dr. Narendra Reddy Medagam,
Department of Spine Surgery, MIOT Hospital, Manapakkam, Chennai, Tamil Nadu – 600089, India.
E-mail: medagam007@gmail.com
Abstract
Introduction: Cervical spine injuries in the children are unusual, and an incidence rate of 1.5–3% of all the spinal fractures has been reported. The cartilaginous end plate between the dens and the body of the axis usually ossifies at the age of 5–7 years. This anatomical characteristic has been attributed to odontoid synchondrosis fractures in young children. However, odontoid process fractures are rare in children and only few cases have been reported in literature.
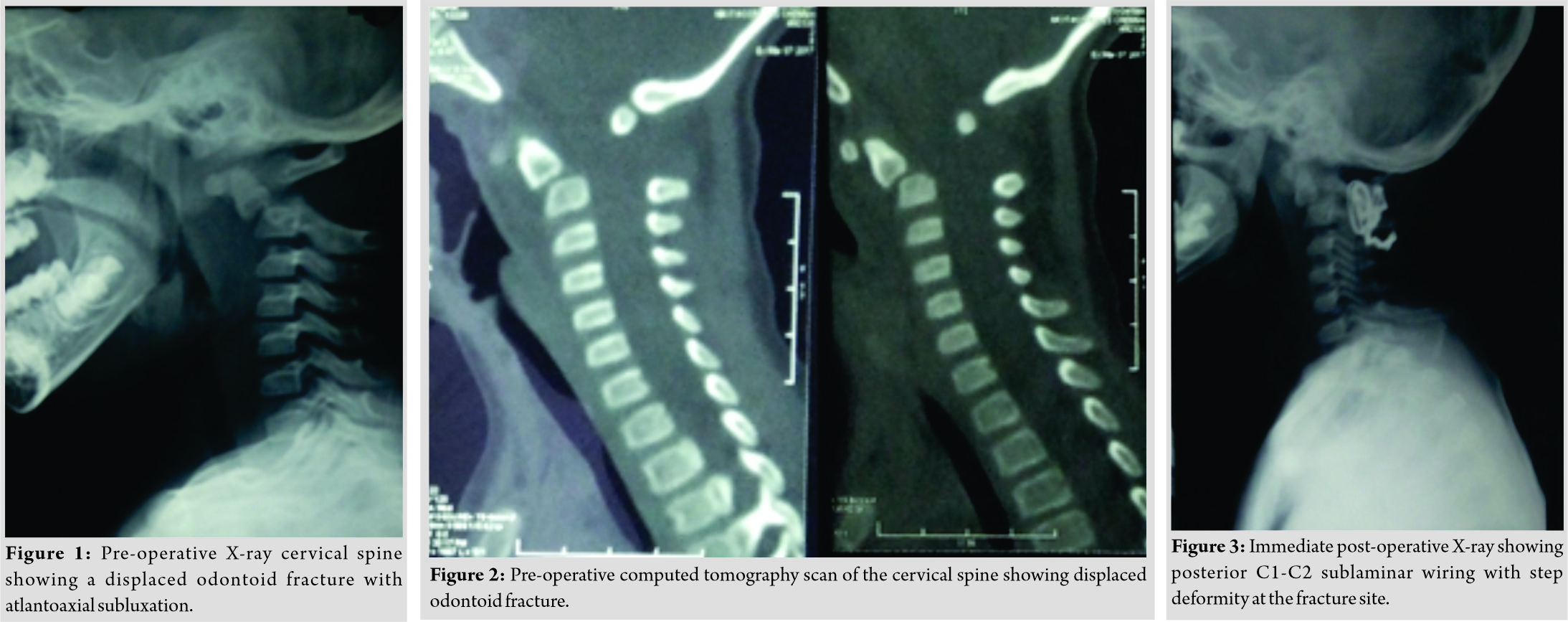
Case Report: We report a case of a displaced odontoid synchondrosis fracture in a 2-year-old girl with anterior subluxation of C1 over C2 vertebra. This was treated with a posterior atlantoaxial fusion using sublaminar wiring. Immediate post-operative radiography showed partial reduction of the displaced odontoid fragment on C2 body with residual step deformity with angulation at the fracture site. Follow-up at 1 year showed excellent remodeling.
Conclusion: Synchondrosis fractures of the odontoid are rare and usually found in children under 7 years of age. Most of these patients can be treated by external immobilization alone. However, in small children with significant displacement and angulation, posterior C1-C2 fusion is a better option providing more stability. Furthermore, one can expect significant remodeling of the fracture within this population.
Keywords: Preschool child, odontoid synchondrosis fracture, remodeling.
Introduction
Cervical spine injuries in the children are unusual, and an incidence rate of 1.5–3% of all the spinal fractures has been reported [1, 2]. The cartilaginous end plate between the dens and the body of the axis usually ossifies at the age of 5–7 years. This anatomical characteristic has been attributed to odontoid synchondrosis fractures in young children [3, 4, 5]. However, odontoid process fractures are rare in children and only few cases have been reported in theliterature [3, 6]. We report a case of a displaced odontoid synchondrosis fracture in a 2-year-old girl with anterior subluxation of C1 over C2 vertebra. This was treated with a posterior atlantoaxial fusion using sublaminar wiring. Immediate post-operative radiography showed partial reduction of the displaced odontoid fragment on C2 body with residual step deformity with angulation at the fracture site. Follow-up at 1 year showed excellent remodeling.
Case Report
A 2-year-old female child was brought to our tertiary care center with alleged history of road traffic accident followed by complaint of inability to hold the neck upright. She had to support her chin with her wrists. Examination revealed restricted neck range of movements with tenderness at the craniocervical junction. Her neurological examination was normal with normal tone maintained in all the four extremities. Radiographs (Fig. 1) and computed tomography (CT) scan of the cervical spine (Fig. 2) revealed a displaced fracture of the odontoid synchondrosis with anterior subluxation of C1 over C2 vertebra.The patient was immobilized with a Philadelphia collar. In view of significant displacement of the odontoid with associated atlantoaxial subluxation, adecision was taken to perform reduction and posterior atlantoaxial fusion using sublaminar wiring. The procedure was performed through a posterior approach. Sublaminar wires were passed under C1 posterior arch and C2 lamina, and reduction was done under fluoroscopy guidance. A small diameter mesh cage filled with hydroxyapatite crystals was placed between the C1 posterior arch and the C2 lamina to maintain C1-C2 vertebral alignment and aid fusion. Surgery was carried out without any complications and postoperatively, she was maintained in Philadelphia collar for a period of 8 weeks. The post-operative period was uneventful. Her immediate post-operative radiography revealed a step deformity with angulation at the fracture site (Fig. 3).
At a 1-year follow-up, CT scan of the cervical spine revealed excellent remodeling at the fracture site with bony posterior fusion at C1-C2 (Fig. 4). She had terminal limitation of rotations of the neck, but sagittal alignment was satisfactory.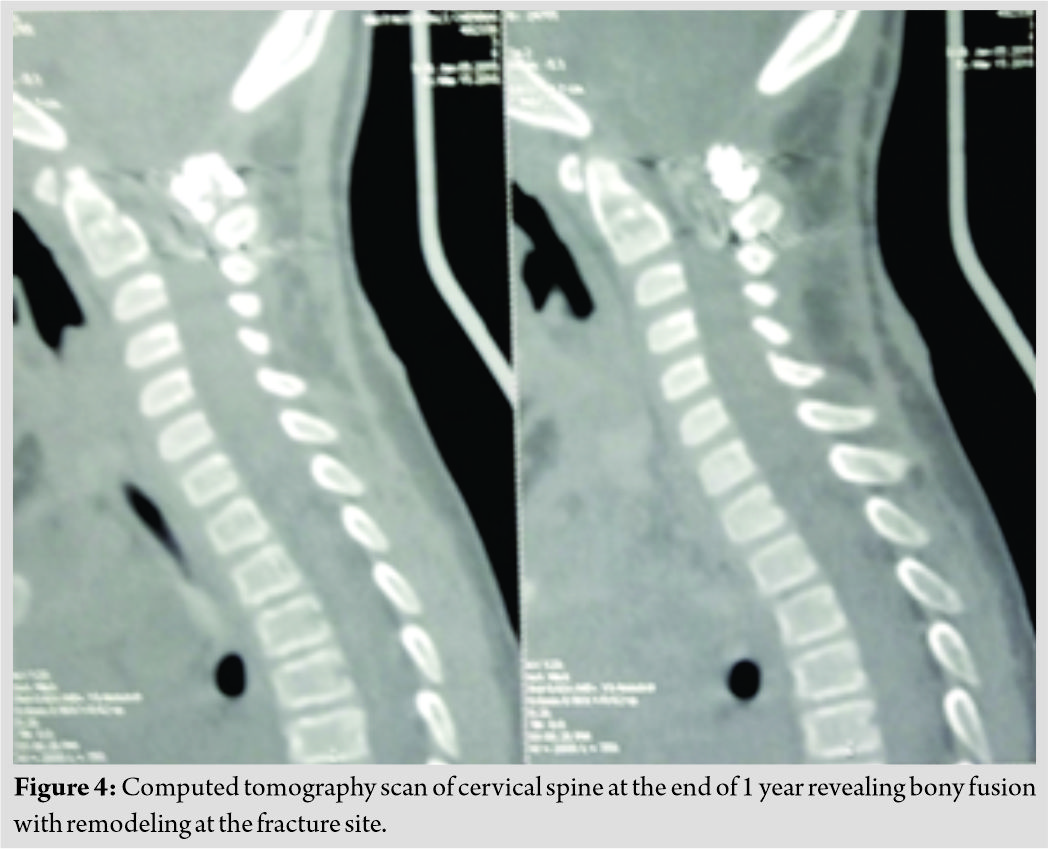
Discussion
Odontoid process fractures in the pediatric population are a rare entity, and the literature is sparse, with only a few cases reported [3, 6]. It is unusual to have bony injuries below the age of 8 years due to relative elasticity of the growing spine [7]. The axis is the most commonly involved vertebra in children and odontoid synchondrosis fractures are usually seen in patients <7 years of age [8]. The management of such fractures in the pediatric population remains unclear. The current recommendations on the management of such an injury include high degree of suspicion focusing on symptoms, lateral cervical spine radiographs, and sagittal CT scan sections. Reduction and immobilization in an external orthosis or surgical stabilization for unstable cases have been reported. Fulkerson et al. in their case series reported a higher failure rate of certain odontoid fractures with external immobilization alone [9]. They considered a significant displacement of the odontoid of 11–100%, angulation of>30°, and clinical evidence of upper cervical spinal cord injury as indications for surgical intervention [9]. In our patient, there was significant displacement of the odontoid (approximately 70%) with C1-C2 subluxation which was associated with >30° angulation approaching the current consensus for the surgical fixation. There was a step deformity in her immediate post-operative radiograph which remodeled well by the end of 1 year. Excellent remodeling potential of the pediatric cervical spine has been reported by Bhagat et al. following in situ fusion in similar fractures in children[10].
Conclusion
Synchondrosis fractures of odontoid are rare and usually found in children under 7 years of age. Most of these patients can be treated by external immobilization alone. However, in small children with significant displacement and angulation, posterior C1-C2 fusion is a better option providing more stability. Furthermore, one can expect significant remodeling of the fracture within this population.
Clinical Message
In small children with odontoid synchondrosis fracture associated significant displacement and angulation, posterior C1-C2 fusion is a better option providing more stability. Furthermore, one can expect significant remodeling of the fracture within this population.
References
1. Patel JC, Tepas JJ 3rd, Mollitt DL, Pieper P. Pediatric cervical spine injuries: Defining the disease. J Pediatr Surg 2001;36:373-6.
2. Warner WC Jr., Hedequist DJ, Beaty JH, Kasser J, editors. Cervical spine injuries in children. In: Rockwood and Wilkins’ Fractures in Children. Philadelphia, PA, USA: Lippincott Williams and Wilkins; 2006. p. 775-814.
3. Sherk HH, Nicholson JT, Chung SM. Fractures of the odontoid process in young children. J Bone Joint Surg Am 1978;60:921-4.
4. Ogden JA. Radiology of postnatal skeletal development. XII. The second cervical vertebra. Skeletal Radiol 1984;12:169-77.
5. Griffiths SC. Fracture of odontoid process in children. J Pediatr Surg1972;7:680-3.
6. Garton HJ, Park P, Papadopoulos SM. Fracture dislocation of the neurocentral synchondroses of the axis. Case illustration. J Neurosurg 2002;96 Suppl 3:350.
7. Blauth M, Schmidt U, Otte D, Krettek C. Fractures of the odontoid process in small children: Biomechanical analysis and report of three cases. Eur Spine J 1996;5:63-70.
8. d’Amato C. Paediatric spinal trauma: Injuries in very young children. Clin Orthopaed Related Res 2005;432:34-40.
9. Fulkerson DH, Hwang SW, Patel AJ, Jea A. Open reduction and internal fixation for angulated, unstable odontoid synchondrosis fractures in children: A safe alternative to halo fixation? J NeurosurgPediatr 2012;9:35-41.
10. Bhagat S, Brown J, Johnston R. Remodelling potential of paediatric cervical spine after Type II odontoid peg fracture. Br J Neurosurg 2006;20:426-8.
 |
 |
 |
 |
 |
| Dr. Narendra Reddy Medagam | Dr. Charanjit Singh Dhillon | Dr. Chetan Shashikant Pophale | Dr. NilayPrafulsinh Chhasatia | Dr. Anandkumar Khatavi |
| How to Cite This Article: Medagam N R, Dhillon C S, Pophale C S, Chhasatia N P, Khatavi A. Preschool Child with Displaced Odontoid Synchondrosis Fracture Treated by Surgical Management Showing Excellent Remodeling. Journal of Orthopaedic Case Reports 2019 Nov-Dec;9(6): 62-64. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


