
[box type=”bio”] Learning Point of the Article: [/box]
Crushed infected dead autologous bone can be used as a salvage procedure to treat infected pseudarthrosis caused by resistant bacteria.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 74-77 | Martin Reichelt, Sebastian Gehmert, Andreas Krieg, Andrej M Nowakowski. DOI: 10.13107/jocr.2019.v09.i06.1596
Authors: Martin Reichelt[1], Sebastian Gehmert[2], Andreas Krieg[2], Andrej M Nowakowski[3],[4]
[1]Department of Orthopaedic, University Hospital Basel, Spitalstrasse 21, 4031 Basel, Switzer-land,
[2]Department of Orthopaedic, University Children’s Hospital Basel, Spitalstrasse 33, 4056 Basel, Switzerland,
[3]Department of Orthopaedic, SpitalUster, Brunnenstrasse 42, 8610 Uster, Switzerland,
[4]Department of Orthopaedic, University of Basel, Klingelbergstrasse 61, 4056 Basel, Switzerland.
Address of Correspondence:
Dr. Andrej M Nowakowski,
SpitalUster, Brunnenstrasse 42, 8610 Uster, Switzerland.
E-mail: andrej.nowakowski@spitaluster.ch
Abstract
Introduction: Osteomyelitis with multiresistant bacteria in non-union following fracture treated with osteosynthesis requires complete removal of infected sequestrum and dead bone. For consecutive bone defects, it is frequently necessary to bridge with a fixator external. The treatment is not only challenging due to reduced bone stock but also characterized by decreased bioavailability of antibiotics.
Case Report: We report a two-step-surgery approach to preserve the bone stock using autologous cancellous bone in a bacterial infected non-union for subsequently leg length reconstruction. The 24-year-old male patient from Belarus was admitted to our department with persistent wound secretion and subsequent osteomyelitis of the right femur 3 years after initial surgery, several revisions, and several different antibiotic therapies. Biopsy revealed methicillin-resistant and borderline oxacillin-resistant Staphylococcus aureus. Firstly, the Ilizarov ring fixator was removed and a vigorous debridement was performed by refreshing the pseudarthrosis, removing of sequestrum, and dead bone. Finally, an AO fixator external was applied for 10 weeks combined with appropriate antibiotic treatment followed by 5 weeks antibiotic-free window. The bone defect was stabilized by a long gamma trochanteric nail after removal of the AO fixateurexterne. A wide resection of the fragments was performed and the resected bone tissue was crushed and placed adjacent to the nail. Noteworthy, the biopsies of both re-section sides revealed same germs as detected in initial biopsies. Thus, antibiotics were administered for additional 3 months. Frequent radiographic and clinical controls showed a remodeling of the femur during a period of 3 years and no signs of infection. Subsequently, we restored leg length of 4 cm using a fully implantable motorized lengthening nail. In the end, the patient achieved full weight-bearing with unlimited range of motion in hip and knee. No further germ could be revealed in biopsies.
Conclusion: In this case report, we used autologous bone from the infected side, crushed, and placed it adjacent to an intramedullary nail. Crushed bone tissue might improve bioavailability of antibiotics when dealing with multiresistant bacteria in non-union healed fracture side. Furthermore, this approach was able to provide new bone formation in a limb resulting in full weight-bearing.
Keywords: Osteomyelitis, infected pseudarthrosis, femur shaft fracture, crushed bone, antibiotic availability.
Introduction
Open bone fractures may pose a risk for osteomyelitis but also might occur after surgical treatment of closed fractures with osteosynthesis material. Osteomyelitis can affect almost all bone tissue with a variety of microbial or fungal pathogens. Thus, identification of the pathogen by bone samples is required to determine the corresponding treatment regimen. However, osteomyelitis caused by a multiresistant germ, (e.g.,Staphylococcus aureus) represents a major challenge since therapeutic options are limited. Bone tissue injury provokes a release of osteoinductive substances (e.g., bone morphogenetic proteins [BMP] 2 and BMP 7) into the cellular matrix, which can stimulate the regeneration of bone tissue [1]. Autologous bone graft not only provides osteoinductive tissue but also facilitates the release of viable, undifferentiated mesenchymal cells, monocytes, precursor cells of osteoclasts, and osteoblasts. These cells have an impact on stimulating bone growth and mediating neoangiogenesis in the affected tissue [2, 3]. The osteoinductive potential of autologous bone graft itself depends on the harvest technique, the presence of systemic disease and the age of the patient. However, the origin of the autologous bone material does not seem to be an important factor in respect of the osteoinductive-potential. For this reason, crushed bone tissue has been studied for their suitability for bone defects resulting from a variety of traumas [4, 5, 6]. We report a successful leg length reconstruction with autologous bone grafts in a patient who had osteomyelitis caused by multiresistant pathogens along with a non-union of a femur fracture after a car accident. To date, the patient is free of infection and able to walk without limitation.
Case Report
A 24-year-old patient was admitted to our department due to a car accident with multiple injuries, including femur fractures of both sides which were treated with plate osteosynthesis in Belarus. No complication was apparent on the left side. However, a persistent wound secretion with subsequent osteomyelitis was present on the right side 3 years after initial surgery even after adequate surgical debridement and antibiotic regime. Biopsy revealed methicillin-resistant and borderline oxacillin-resistant S. aureus (BORSA). X-rays confirmed osteomyelitis with a sequestrum, a fistula, and significantly reduced bone stock. The patient presented with an Ilizarov ring fixator in situ in our department for the 1st time in 2012. The Ilizarov ring fixator was implanted in Belarus in 2011. The patient preferred an exceptional salvage procedure to preserve the limb since amputation was not an option (Fig. 1). Therefore, we suggested a two-step-surgery approach to treat the osteomyelitis before performing the definitive osteosynthesis. The Ilizarov ring fixator was removed and a vigorous debridement was performed by refreshing the pseudarthrosis, removing the sequestrum, and dead bone. Finally, an AO fixator external was implanted after several efficient debridements (Fig. 2a and b). 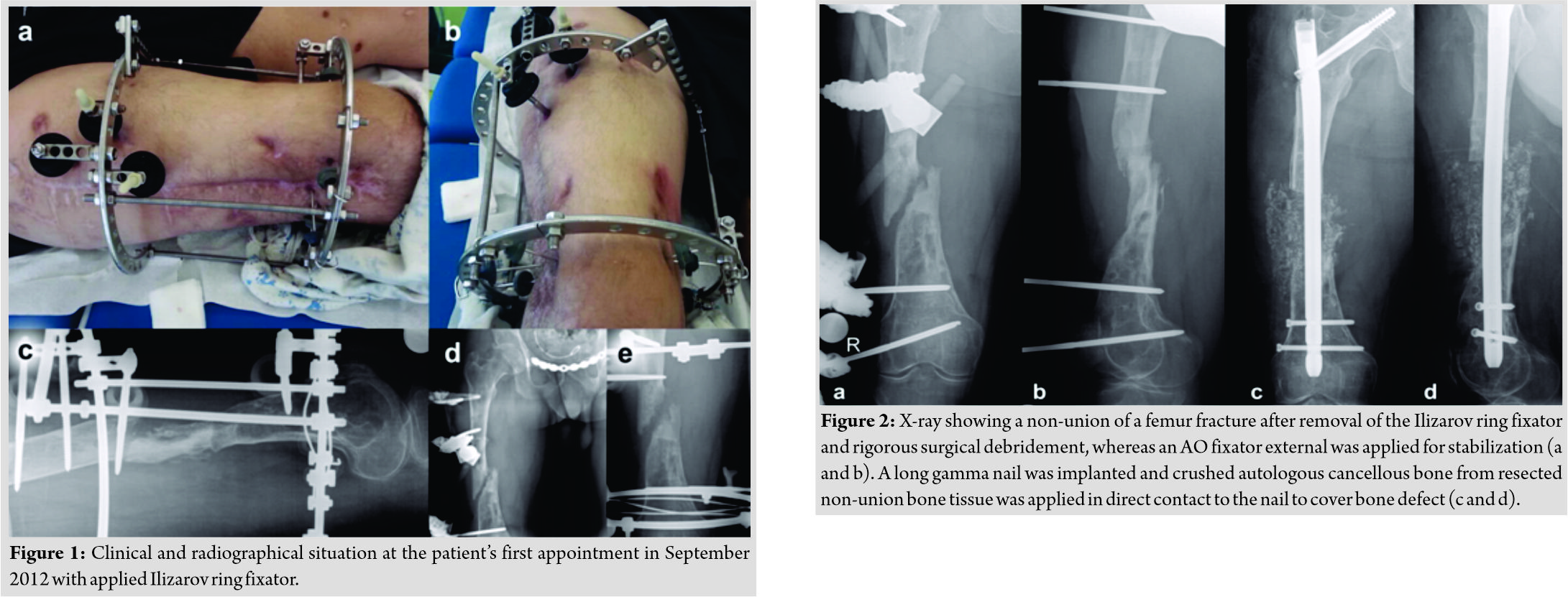 An antibiotic therapy was established with vancomycin (20 mg/kg/d) for 4 weeks followed by clindamycin (1800 mg/d) and co-trimoxazole forte (sulfamethoxazole 2400 mg/d/trimethoprim 640 mg/d) for 6 weeks. Ciprofloxacin (1500 mg/d) was additional given for the first 2 weeks during the treatment with clindamycin. The AO fixator external was removed after 10 weeks of antibiotic treatment and surgery was performed after an additional antibiotic-free window of 5 weeks. We decided to perform a definitive treatment without intraoperative local antibiotic carrier application since the laboratory blood test revealed no elevated infection parameters. Moreover, no signs of persistent infection were found during the operation. The bone defect was stabilized by a long gamma trochanteric nail (Stryker, UK). A wide resection of the non-union tissue was performed which was crushed and placed beside the nail to bridge the defect zone (Fig. 2c and d). Surprisingly, biopsies of the proximal and distal non-union side revealed the same bacteria and resistogram when compared to the initial biopsies taken before the rigorous debridement procedures (Table 1). However, reimplantation of crushed bone tissue from the infected side did not result in a relapse of osteomyelitis. The most likely bacteria load was reduced and the local effect of antibiotics was improved by crushed bone even when used from non-union infected side. Antibiotic therapy was established with vancomycin (20 mg/kg/d) for 2 weeks followed by co-trimoxazole forte (sulfamethoxazole 2400 mg/d/trimethoprim 640 mg/d) for 10 weeks. Neoangiogenesis proceeds much faster in small autologous fragments as in large dimensioned bone stock. Therefore, the blood supply increased around the affected area along with the bioavailability of antibiotics. Frequent radiographic and clinical controls showed remodeling of the femur during a period of 3 years with partial weight-bearing and no signs of infection (Fig. 3). Due to the bone spanning with cancellous bone and the increase soft tissue tension by an infected, shortened, and for 3 years not loaded leg, we decided to restore the leg length of 4 cm in a further step. The long gamma trochanteric nail (Stryker, UK) was removed after 2 years of no signs of in-fection and limb lengthening procedure was carried out by implanting a fully implantable mo-torized lengthening nail (Fitbone®, Wittenstein, Germany). In addition, a varus supracondylar femur osteotomy was performed to correct for biomechanical alignment (Fig. 4a and b).
An antibiotic therapy was established with vancomycin (20 mg/kg/d) for 4 weeks followed by clindamycin (1800 mg/d) and co-trimoxazole forte (sulfamethoxazole 2400 mg/d/trimethoprim 640 mg/d) for 6 weeks. Ciprofloxacin (1500 mg/d) was additional given for the first 2 weeks during the treatment with clindamycin. The AO fixator external was removed after 10 weeks of antibiotic treatment and surgery was performed after an additional antibiotic-free window of 5 weeks. We decided to perform a definitive treatment without intraoperative local antibiotic carrier application since the laboratory blood test revealed no elevated infection parameters. Moreover, no signs of persistent infection were found during the operation. The bone defect was stabilized by a long gamma trochanteric nail (Stryker, UK). A wide resection of the non-union tissue was performed which was crushed and placed beside the nail to bridge the defect zone (Fig. 2c and d). Surprisingly, biopsies of the proximal and distal non-union side revealed the same bacteria and resistogram when compared to the initial biopsies taken before the rigorous debridement procedures (Table 1). However, reimplantation of crushed bone tissue from the infected side did not result in a relapse of osteomyelitis. The most likely bacteria load was reduced and the local effect of antibiotics was improved by crushed bone even when used from non-union infected side. Antibiotic therapy was established with vancomycin (20 mg/kg/d) for 2 weeks followed by co-trimoxazole forte (sulfamethoxazole 2400 mg/d/trimethoprim 640 mg/d) for 10 weeks. Neoangiogenesis proceeds much faster in small autologous fragments as in large dimensioned bone stock. Therefore, the blood supply increased around the affected area along with the bioavailability of antibiotics. Frequent radiographic and clinical controls showed remodeling of the femur during a period of 3 years with partial weight-bearing and no signs of infection (Fig. 3). Due to the bone spanning with cancellous bone and the increase soft tissue tension by an infected, shortened, and for 3 years not loaded leg, we decided to restore the leg length of 4 cm in a further step. The long gamma trochanteric nail (Stryker, UK) was removed after 2 years of no signs of in-fection and limb lengthening procedure was carried out by implanting a fully implantable mo-torized lengthening nail (Fitbone®, Wittenstein, Germany). In addition, a varus supracondylar femur osteotomy was performed to correct for biomechanical alignment (Fig. 4a and b).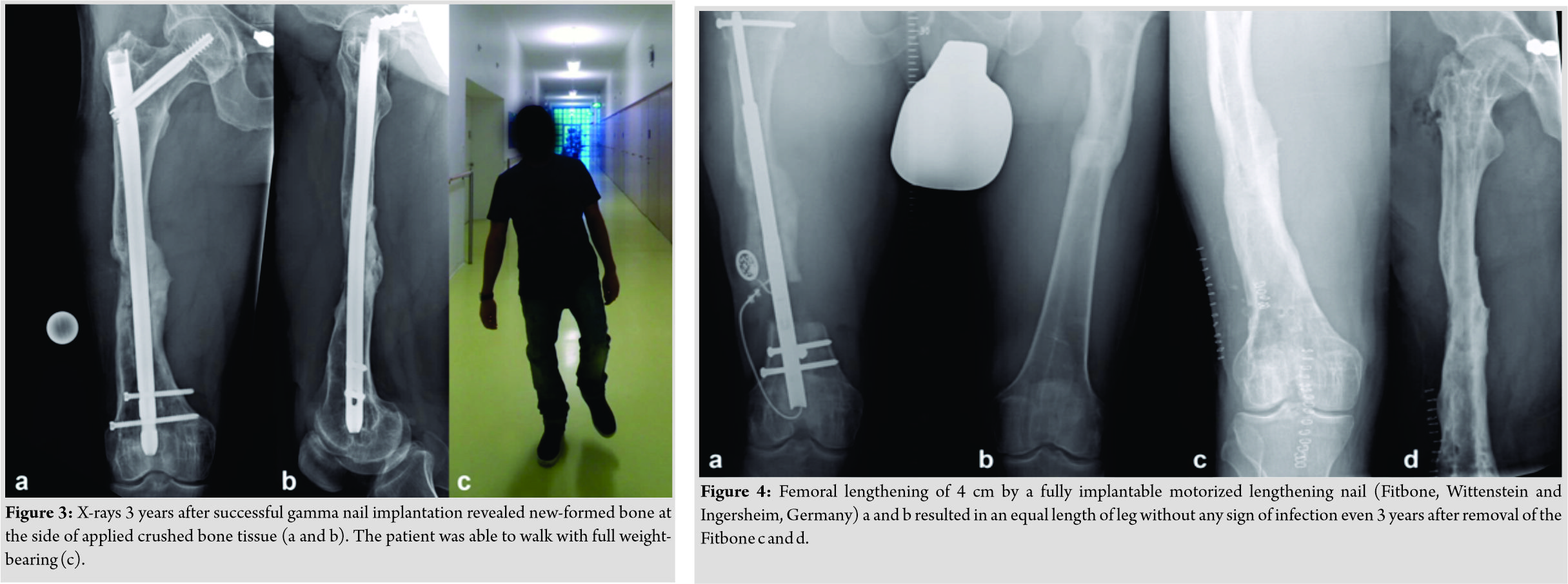 The fully implantable motorized lengthening nail (Fitbone®) was removed after successful limb lengthening and final bone biopsies revealed no infection (Fig. 4c and d). Due to the long period of rest and partial loading, the knee and hip joint was severely re-stricted in the range of motion (ROM) and the bone showed osteopenia in the radiological control. After intensive physiotherapeutic treatment, the patient achieved an unrestricted ROM with his indolent hip and knee joints.
The fully implantable motorized lengthening nail (Fitbone®) was removed after successful limb lengthening and final bone biopsies revealed no infection (Fig. 4c and d). Due to the long period of rest and partial loading, the knee and hip joint was severely re-stricted in the range of motion (ROM) and the bone showed osteopenia in the radiological control. After intensive physiotherapeutic treatment, the patient achieved an unrestricted ROM with his indolent hip and knee joints.
Discussion
The case report describes a treatment option of an infected non-union, which was supported by crushed cancellous bone fragments, although continuously treatment of the osteomyelitis was not successful. We did not use BMP or bone graft substitutes, given the fact that blood test revealed normal range of infection parameters and crushed bone tissue is reported to release BMP [7]. We assume that the grinded bone tissue improved local antibiotic availability and provoked a reduction of the bacterial load. However, the bone remodeled due to autologous crushed cancellous bone support and limb length discrepancy was corrected by a motorized intramedullary nail. Most likely, osteoinductive substances (e.g., BMP 2, BMP 7) were released in a sufficient amount by vigorous debridement, reaming for long gamma trochanteric nail (Stryker, UK), and autologous bone grafting. In addition, osteoprogenitor cells were released using the resected non-union tissue. Thus, osteogenic, osteoinductive, and osteoconductive properties were provided at the side which were needed without the risk of immunogenicity [1]. However, autologous bone graft is limited in quantity and associated with donor-side morbidity. A rigorous antibiotic treatment and iterative surgical debridement reduced bacteria load in the harvested tissue resulting in bone healing even when biopsies revealed bacteria in harvested and applied bone tissue. Motsitsi described a healing rate of osteomyelitis up to 84.4% by Ilizarov ring fixator. However, literature about intramedullary treatment in osteomyelitis is rare [8]. We suggest that bone healing was possible due to the release of osteoinductive proteins along with improved availability of antibiotics by crushed autologous bone. Thus, reimplantation of crushed and extracorporeal eradicated sequestrum might be a valuable option for a salvage procedure when autologous donor bone is limited.
Conclusion
This case report is about a 24-year-old patient who suffered a double femoral fracture as a result of a car accident and was also diagnosed with osteomyelitis caused by methicillin-resistant and BORSA. Treatment of the fracture was possible by application of autologous comminuted cancellous bone of the patient even when bacteria were detected which caused the osteomyelitis. To our knowledge, apart from the field of dentistry, no similar case report exists regarding the treatment of bone defect with infected autologous bone tissue, especially with multiresistant bacteria. Although no comparable cases are present in literature, the described application of crushed infected autologous bone tissue should be taken into account for future medical developments in bone regeneration and salvage procedures.
Clinical Message
Bone tissue healing may be facilitated by crushed autologous fragments even when used from osteomyelitis since the bioavailability of antibiotics is improved for grinded bone tissue. Crushed autologous bone tissue might be a feasible salvage procedure especially when several previous attempts have failed to treat a non-union associated with osteomyelitis.
References
1. Barradas AM, Yuan H, van Blitterswijk CA, Habibovic P. Osteoinductive biomate-rials: Current knowledge of properties, experimental models and biological mechan-isms. Eur Cell Mater 2011;21:407-29.
2. Slotte C, Lundgren D, Burgos PM. Placement of autogeneic bone chips or bovine bone mineral in guided bone augmentation: A rabbit skull study. Int J Oral Maxillofa-cImplants 2003;18:795-806.
3. Schlegel KA, Fichtner G, Schultze-Mosgau S, Wiltfang J. Histologic findings in sinus augmentation with autogenous bone chips versus a bovine bone substitute. Int J Oral Maxillofac Implants 2003;18:53-8.
4. Valentini P, Abensur DJ. Maxillary sinus grafting with anorganic bovine bone: A clin-ical report of long-term results. Int J Oral Maxillofac Implants 2003;18:556-60.
5. Gutwald R, Haberstroh J, Kuschnierz J, Kister C, Lysek DA, Maglione M, et al. Me-senchymal stem cells and inorganic bovine bone mineral in sinus augmentation: Com-parison with augmentation by autologous bone in adult sheep. Br J Oral Maxillofac Surg 2010;48:285-90.
6. Gomes KU, Carlini JL, Biron C, Rapoport A, Dedivitis RA. Use of allogeneic bone graft in maxillary reconstruction for installation of dental implants. J Oral Maxillofac Surg 2008;66:2335-8.
7. Bostrom MP, Lane JM, Berberian WS, Missri AA, Tomin E, Weiland A, et al. Immu-nolocalization and expression of bone morphogenetic proteins 2 and 4 in fracture heal-ing. J OrthopRes 1995;13:357-67.
8. Bauer T, Klouche S, Grimaud O, Lortat-Jacob A, Hardy P. Treatment of infected non-unions of the femur and tibia in a French referral center for complex bone and joint in-fections: Outcomes of 55 patients after 2 to 11 years. Re Chir Orthop Trauma-tol2018;104:89-97.
 |
 |
 |
 |
| Dr. Martin Reichelt | Dr. Sebastian Gehmert | Dr. Andreas Krieg | Dr. Andrej M Nowakowski |
| How to Cite This Article: Reichelt M, Gehmert S, Krieg A, Nowakowski A M. Bone Crushing in Infected Pseudarthrosis – An Extraordinary Way to Treat Osteomyelitis Caused by Resistant Bacteria. Journal of Orthopaedic Case Reports 2019 Nov-Dec;9(6): 74-77. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


