
[box type=”bio”] Learning Point of the Article: [/box]
Since this a rare condition, shoulder arthroscopists should be aware of its potential to become abnormally thickened and causing shoulder dysfunction.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 94-97 | Roshan Wade, Swapneel Sunil Shah, Sujith B.S., Kunal A Shah, Aditya Raj. DOI: 10.13107/jocr.2019.v09.i06.1606
Authors: Roshan Wade[1], Swapneel Sunil Shah[1], Sujith B.S.[2], Kunal A Shah[1], Aditya Raj[1]
[1]Department of Orthopedics, Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India,
[2]Department of Orthopedics, Topiwala Medical College and Nair hospital, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Roshan Wade,
Department of Orthopedics, Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India.
E-mail: roshanwade@gmail.com
Abstract
Introduction: Early studies on human embryology reveal a migration of the tendon of long head of biceps from the synovium and fibrous capsule to an intra-articular position [1, 2, 3]. Any hindrance in the normal course of events of development, pathological or otherwise, may result in variations from the normal anatomy.
Case Report: Here, we discuss a case of a rare anatomical variant of the origin of long head of biceps tendon discovered incidentally in a 30-year-old manual laborer. The patient had an insidious onset and gradually progressive right shoulder pain, especially in initiating abduction, with a feeling of instability for 5 months. On examination, apprehension test and anterior drawer test were present and sulcus sign was positive. Partial-thickness supraspinatus tear and fraying of the anteroinferior glenoid labrum were noted in the imaging. After giving a fair trial of conservative management, the patient was posted for an arthroscopic repair of the supraspinatus tear and the anteroinferior glenoid labrum when the anomalous origin of the tendon of long head of biceps was discovered incidentally. This origin was from the inferior surface of the supraspinatus muscle outside the capsule. The tendon was left intact as it was not found to be inflamed or degenerated and was not the source of instability.
Conclusion: Due to the rarity of this anatomical variant, definite conclusions cannot be drawn currently regarding its pathological nature. Shoulder arthroscopists should be aware of its potential to become abnormally thickened and causing shoulder dysfunction.
Keywords: Long head biceps, origin, rare anatomical variant.
Introduction
During the normal inutero growth, the tendon of the long head of biceps develops from the region around the shoulder capsule. Early studies on human embryology reveal a migration of the tendon of long head of biceps from the synovium and fibrous capsule to an intra-articular position [1, 2, 3]. Any hindrance in the normal course of events of development, pathological or otherwise, may result in variations from the normal anatomy. The clinical effects of these aberrant anatomical origins remain mostly unknown. These anatomical variations are mostly discovered incidentally by shoulder arthroscopists and include intra-articular and extra-articular anomalies as well as agenesis. This article aims at describing one such rare anatomical variant of the origin of the tendon of long head of biceps discovered incidentally.
Case Report
A 30-year-old male, right-handed, manual laborer presented with an insidious onset and gradually progressive right shoulder pain with a feeling of instability for 5 months. For these complaints, the patient visited the outpatient department. On examination, the patient was apprehensive of external rotation beyond 60°. The patient had an anterior drawer test and sulcus sign positive (Fig. 1). The patient had pain while initiating abduction. The range of abduction, however, was equal as compared to the opposite side. There was no pain or restriction of range on adduction and internal rotation. The impact maneuvers (Neer and Hawkins) were negative. There was no tenderness on palpation of the bicipital groove. Radiological investigations in the form of radiogram (Fig. 2) and magnetic resonance imaging (Fig. 3) were performed. Partial-thickness supraspinatus tear and fraying of the anteroinferior glenoid labrum were noted in the imaging. The patient was advised conservative line of management with analgesics and physiotherapeutic rehabilitation for a period of 3 months. After the completion of this conservative treatment protocol, the patient presented for follow-up with persistence of pain. The patient was posted for an arthroscopic repair of the supraspinatus tear and the anteroinferior glenoid labrum. During the arthroscopic procedure, a variation in the anatomical origin of the long head of biceps was noted; the origin was on the inferior surface of the supraspinatus (Fig. 4). This tendon of long head of biceps was not found to be inflamed or degenerated and was stable on probing. Arthroscopic repair of the supraspinatus tendon and capsulolabral reinforcement was performed using absorbable anchors. The tendon of long head of the biceps was not operated on. On 1-month follow-up, the pain had significantly decreased and the complaint of instability was also completely resolved. The patient resumed work after 6 months of rehabilitation.
Discussion
The long head of biceps tendon (LHBT) has been described as taking origin from the supraglenoid tubercle, from there LHBT traverses the glenohumeral joint, i.e., intra-articular part and through the intertubercular sulcus, i.e., extra-articular part and later becomes a musculotendinous structure [4]. However, a number of anatomic variations have been reported in literature such as supernumerary heads, bifurcated origin from the supraglenoid tubercle and posterior labrum, capsular origin, aberrant rotator cuff origin, and split tendon from a single origin [5, 6, 7].  The biceps variant observed in our case was originating from the inferior surface of supraspinatus in close proximity to the posterior capsule later coursing along the deltoid. However, the unusual biceps origin did not seem to be the reason for symptomatology of the subject. This finding of ours is consistent with other published reports of asymptomatic aberrant origins of the long head of the biceps [8, 9]. Many authors described LHBT originating from the rotator cuff; however, their precise role in development of various shoulder pathologies is often debated on. Hyman and Warren [10] described an extra-articular origin of the long head of the biceps from the supraspinatus. MacDonald [11] reported a case of long head taking origin from the superior labrum but was also found adherent to the undersurface of the cuff intra-articularly. Kim et al. [12] reported a case of LHBT taking origin from the intra-articular rotator cuff. Lang et al. [13] described a variant in which LHBT originated from the rotator cable and lacked an attachment at the superior labrum, which was also associated with a partial articular-sided rotator cuff tear. Most of the authors quoted above noticed anomalous origin of biceps tendon found incidentally on arthroscopy itself was not pathologic and was left intact. They reported complete resolution of symptoms after the management of concomitant shoulder pathology.
The biceps variant observed in our case was originating from the inferior surface of supraspinatus in close proximity to the posterior capsule later coursing along the deltoid. However, the unusual biceps origin did not seem to be the reason for symptomatology of the subject. This finding of ours is consistent with other published reports of asymptomatic aberrant origins of the long head of the biceps [8, 9]. Many authors described LHBT originating from the rotator cuff; however, their precise role in development of various shoulder pathologies is often debated on. Hyman and Warren [10] described an extra-articular origin of the long head of the biceps from the supraspinatus. MacDonald [11] reported a case of long head taking origin from the superior labrum but was also found adherent to the undersurface of the cuff intra-articularly. Kim et al. [12] reported a case of LHBT taking origin from the intra-articular rotator cuff. Lang et al. [13] described a variant in which LHBT originated from the rotator cable and lacked an attachment at the superior labrum, which was also associated with a partial articular-sided rotator cuff tear. Most of the authors quoted above noticed anomalous origin of biceps tendon found incidentally on arthroscopy itself was not pathologic and was left intact. They reported complete resolution of symptoms after the management of concomitant shoulder pathology.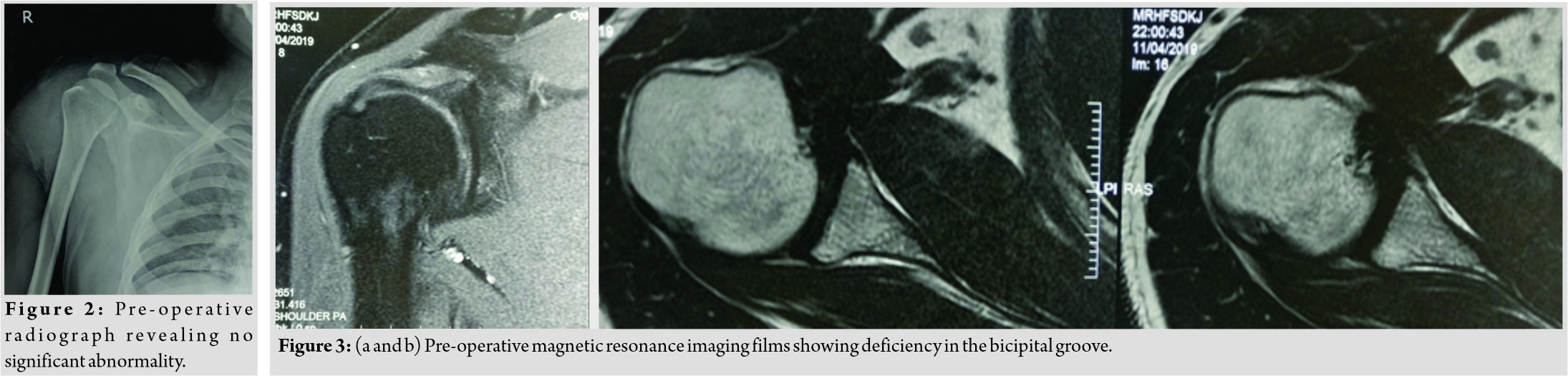
Nevertheless, there are few studies establishing causal relationship between aberrant origins of LHBT and shoulder pathologies. Ogawa and Naniwa [14] hypothesized that the biceps tendon passing through the supraspinatus tendon could contribute to rotator cuff tear. Gramstad et al. [15] in a cadaveric study found that the tension in LHBT increased significantly with humeral rotations in both coronal and sagittal planes. The result of this study substantiates the hypothesis that abnormal origin of LHBT may potentially lead to restriction of range of motion due to alterations in the functional length of tendon. It is difficult to absolutely ascertain that anomalous origin of LHBT leads to restriction of range of motion due to lack of sufficient arthroscopic evidence and lack of studies quoting improvement of range of motion after surgical intervention. Many authors strongly believe that congenital absence of the LHBT is more causally related to the development of shoulder instability and other pathologic conditions rather than developmental anomalies with no clinical consequences. Ghalayini et al. [16] reported a case of woman with bilateral absent long head of the biceps tendon, bilateral shoulder instability, and bilateral congenital limb abnormalities. Glueck et al. [17] described a 25-year-old woman with multidirectional instability associated with an absent LHBT without any other congenital anomalies. These associations reiterate the fact that LHBT acts as a depressor of the humeral head and a dynamic stabilizer of the glenohumeral joint.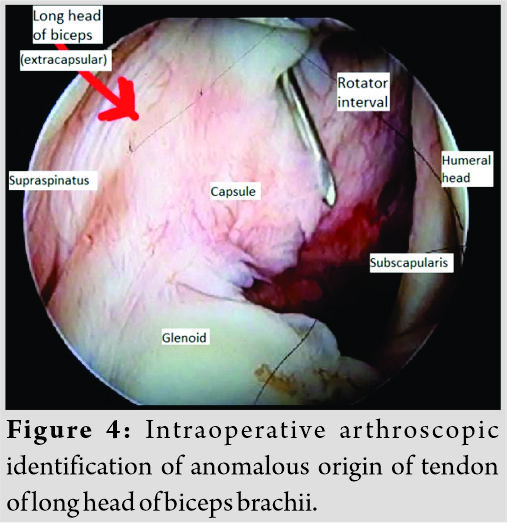
Conclusion
Such aberrant origins are seldom observed in clinical practice and their clinical implication is largely unknown. Some authors mostly in single-case reports have reported to be having causal relationship between aberrant origin of the LHBTs and conditions such asrotator cuff degeneration, instability, impingement, chronic pain, and acromioclavicular arthritis.
Clinical Message
Shoulder arthroscopists should be aware of its potential to become abnormally thickened and causing shoulder dysfunction.
References
1. GardnerE, GrayDJ. Prenatal development of the human shoulder and acromioclavicular joints. Am J Anat1953;92:219-76.
2. Tena-ArreguiJ, Barrio-AsensioC, Puerta-FonolláJ, Murillo-GonzálezJ. Arthroscopic study of the shoulder joint in fetuses.Arthroscopy2005;21:1114-9.
3. Welcker H. Die einwanderung der bicepssehne in das schultergelenk. Nebstnotizen uber ligamentum interarticularehumeri und ligamentum teres femoris. Arch AnatPhysiol1878;1:20-42.
4. Last RJ. The upper limb. In: Anatomy: Regional and Applied. Edinburgh: Churchill Livingstone; 1984. p. 52-125.
5. DemondionX, MaynouC, VanCortenbosch B, KleinK, LeroyX, MestdaghH. Relationship between the tendon of the long head of the biceps brachii muscle and the glenoid labrum.Morphologie2001;85:5-8.
6. Depalma AF, Callery G, Bennett GA. Variational anatomy and degenerative lesions of the shoulder joint. Instr Course Lect1949;6:255-81.
7. VangsnessCT Jr., JorgensonSS, WatsonT, JohnsonDL. The origin of the long head of the biceps from the scapula and glenoid labrum. An anatomical study of 100 shoulders.J Bone Joint Surg Br1994;76:951-4.
8. WittsteinJ, LassiterT Jr., TaylorD. Aberrant origin of the long head of the biceps: A case series.J Shoulder Elbow Surg2012;21:356-60.
9. BanerjeeS, PatelVR. Anomalous biceps origin from the rotator cuff.Indian J Orthop2015;49:105-8.
10. HymanJL, WarrenRF. Extra-articular origin of biceps brachii.Arthroscopy2001;17:E29.
11. MacDonaldPB. Congenital anomaly of the biceps tendon and anatomy within the shoulder joint.Arthroscopy1998;14:741-2.
12. KimKC, RheeKJ, ShinHD. A long head of the biceps tendon confluent with the intra-articular rotator cuff: Arthroscopic and MR arthrographic findings.Arch Orthop Trauma Surg2009;129:311-4.
13. LangJE, VinsonEN, BasamaniaCJ. Anomalous biceps tendon insertion into the rotator cable: A case report.J Surg Orthop Adv2008;17:93-5.
14. OgawaK, NaniwaT. A rare variation of the biceps: A possible cause of degeneration of the rotator cuff.J Shoulder Elbow Surg1998;7:295-7.
15. GramstadGG, SearsBW, MarraG. Variation of tension in the long head of the biceps tendon as a function of limb position with simulated biceps contraction.Int J Shoulder Surg2010;4:8-14.
16. GhalayiniSR, BoardTN, SrinivasanMS. Anatomic variations in the long head of biceps: Contribution to shoulder dysfunction.Arthroscopy2007;23:1012-8.
17. GlueckDA, MairSD, JohnsonDL. Shoulder instability with absence of the long head of the biceps tendon. Arthroscopy2003;19:787-9.
 |
 |
 |
 |
 |
| Dr. Roshan Wade | Dr. Swapneel Sunil Shah | Dr. Sujith B.S. | Dr. Kunal A Shah | Dr. Aditya Raj |
| How to Cite This Article: Wade R, Shah SS, Sujith BS, Shah K, Raj A. A Rare Anatomical Variation in the Origin of the Tendon of Long Head of Biceps in a 30-Year-Old Male: A Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2019 Nov-Dec;9(6): 94-97. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


