
[box type=”bio”] Learning Point of the Article: [/box]
This case report demonstrates a successful treatment outcome for isolated medial dislocation of long head of biceps without an associated rotator cuff tear. This case report also helps review the complex anatomy of the long head of the biceps with relation to the biceps pulley.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 6-10 | Matthew L Vopat, Shang-You Yang, Cole Mc Gregor, K James Kallail, Bradley M Saunders. DOI: 10.13107/jocr.2019.v09.i06.1564
Authors: Matthew L Vopat[1], Shang-You Yang[1],[2], Cole Mc Gregor[1], K James Kallail[1], Bradley M Saunders[1],[3]
[1]Department of Orthopaedic Surgery, University of Kansas School of Medicine-Wichita, Wichita, Kansas.,United States,KS
[2]Department of Biological Sciences, Wichita State University, Wichita, KansasKS .,United States,
[3]Via Christi Clinic, Wichita, KansasKS., United States.
Address of Correspondence:
Dr. Bradley M Saunders,
C/o Dr. Shang-You Yang, Orthopaedic Residency Program, Via Christi St. Francis Hospital, 929 N. St. Francis Street, Wichita, Kansas 67214, United States.
E-mail: syang6@kumc.edu
Abstract
Introduction: Medial dislocation of the long head of the biceps tendon (LHBT) is classically known as a pathognomonic finding for a subscapularis or at least a rotator cuff (RC) injury. However, this case report outlines a young active individual with symptomatic medial dislocation of the long head of the biceps with associated posterior instability, without a corresponding RC injury.
Case Report: An 18-year-old male complained of the left shoulder pain and crepitus after a shoulder injury while playing hockey a year prior. Magnetic resonance imaging demonstrated medial dislocation of the LHBT without subscapularis or supraspinatus tendon injury. The patient complained of instability in the shoulder and exam findings supported posterior instability of the glenohumeral joint. Arthroscopic debridement of the glenohumeral joint with arthroscopic posterior capsulorrhaphy and open biceps tenodesis was performed. The patient regained full and painless range of motion at 2-year follow-up.
Conclusion: Medial dislocation of the LHBT can occur without injury to the subscapularis tendon. Furthermore, a capsulorrhaphy with open biceps tenodesis and closure of the rotator interval may provide a successful outcome for this rare injury pattern.
Keywords: Long head of the biceps tendon, dislocation, biceps pulley.
Introduction
Besides maintaining dynamic stability to the glenohumeral joint, the rotator cuff (RC) plays an important role in stabilizing long head of the biceps tendon(LHBT) [1]. Anatomically, the subscapularis tendon attaches to the lesser tuberosity and lies anterior to the biceps tendon sitting in the bicipital groove. The subscapularis tendon aids in stabilizing the LHBT in the bicipital groove, along with the transverse humeral ligament. Some argue that the transverse humeral ligament is simply an extension of the subscapularis tendon and not a separate anatomic structure [2, 3].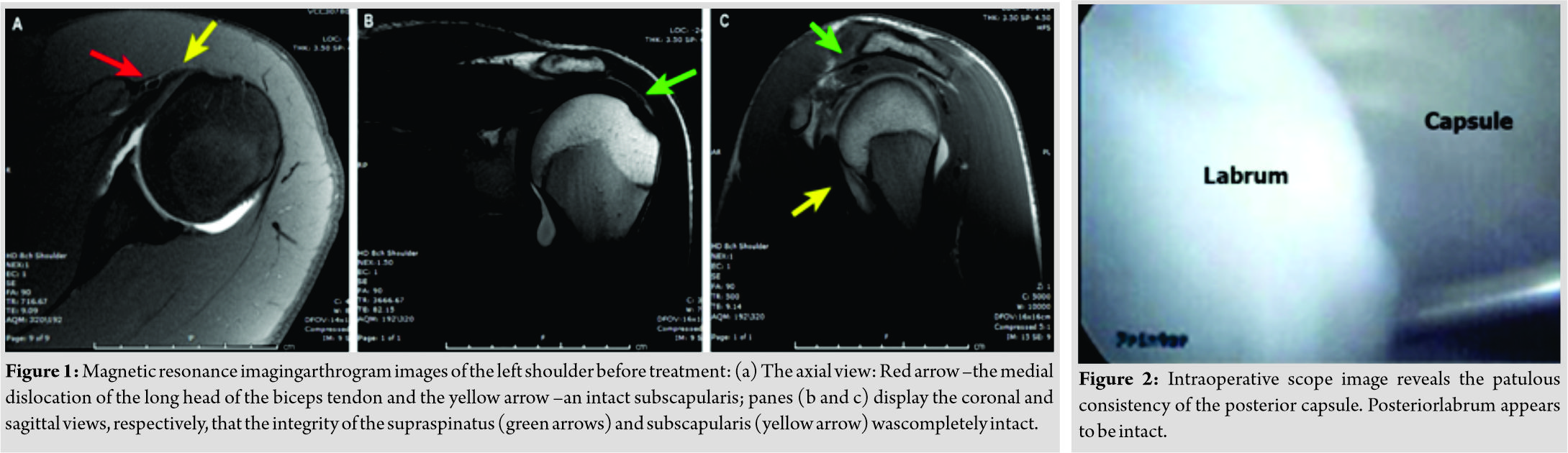
Medial dislocation of the LHBT is a pathognomonic finding for a subscapularis tear or at the very least a RC injury [4, 5, 6, 7, 8]. However, this case report outlines a young active patient suffering from a medial dislocation of the LHBT with associated posterior instability and without corresponding RC injury. Although there have been previous reports of isolated dislocations without associated RC injuries [1, 4, 5, 9], only one other case has been described in association with posterior shoulder instability [4]. Our case further evaluates the pathological relationship between medial LHBT dislocation and posterior shoulder instability and describes a treatment course that resulted in a favorable outcome for this rare pathology.
Case Report
An 18-year-old male presented to clinic with a 1-year history of the left-sided shoulder pain and symptomatic instability. The patient also described an occasional popping sensation in the anterior aspect of the shoulder. The symptoms began after the patient was pushed into a wall while playing hockey which resulted in an anteromedial directed force to the left arm and shoulder. He further described this traumatic episode as a forceful adduction and internal rotation of the left arm. He denied any other trauma or surgeries to the shoulder and had no other relevant past medical history.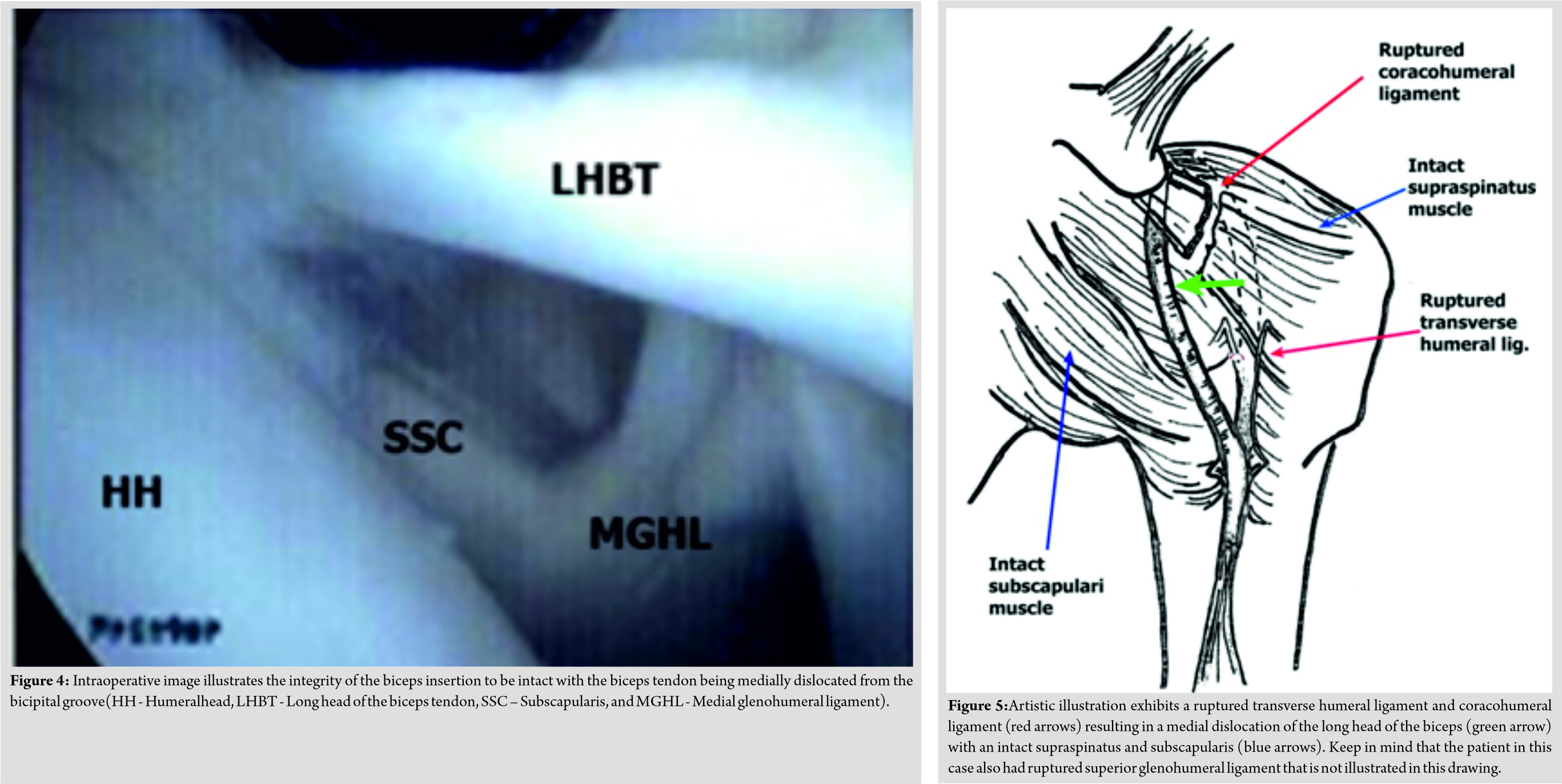
On exam, the patient’s pain was localized to the bicipital groove and the posterior glenohumeral joint line. Speed’s and O’Brien’s tests were positive. The load and shift test demonstrated posterior laxity with translation of the humeral head to the posterior glenoid rim without frank dislocation; which was markedly different when compared to the contralateral shoulder. A passive range of motion (ROM) demonstrated 160of forward flexion overhead bilaterally. The patient’s active internal rotation of the left arm behind the back reached the level of the T10 vertebrae and he had a negative liftoff and belly press tests. With the elbows flexed and arms at the patient’s sides, active external rotation was measured at 65 on the left. The patient demonstrated 5/5 strength in all directions of movement of the left shoulder. Magnetic resonance (MR) arthrogram and MR imaging (MRI) of the left shoulder joint were indicated medial dislocation of the LHBT with intact subscapularis and supraspinatus tendons (Fig. 1). No abnormalities were noted in the osseous structures of the shoulder and the posterior labrum was intact. However, the posterior capsule appeared to be enlarged on MRI studies. The treatment options were discussed with the patient, and the plan was made for open biceps tenodesis and arthroscopic posterior capsulorrhaphy with a possible labral repair if indicated. Pre-operative examination under anesthesia demonstrated posterior subluxation, with posterior laxity noted with the arm flexed forward, internally rotated, and adducted. The load and shift test measured 1+ laxity and a marked difference was noted compared to the contralateral side. Diagnostic arthroscopy was performed using a standard posterior viewing portal and two anterior portals. The posterior capsule was patulous, consistent with pre-operative imaging findings (Fig. 2). An instrument portal was dilated using a cannula in preparation for capsulorrhaphy. Three stitches were used in a pinch and tuck technique starting at the 6:30 position on the glenoid and progressing clockwise in a circumferential manner to the 11:30 region on the glenoid cavity, and the volume of the cavity was reduced (Fig. 3). The integrity of the subscapularis tendon was intact with a medially dislocated LHBT (Fig. 4). After the LHBT was identified, it was prepared for the biceps tenodesis by tagging and releasing in the standard fashion. The left arm was prepped for a standard open deltopectoral approach. On initial inspection, the LHBT was inflamed and was densely adherent to the conjoined tendon. The LHBT was scarred down onto the subscapularis. Further, inspection revealed complete rupture of the coracohumeralligament (CHL) and superior glenohumeral ligaments (SGHLs). The LHBT was dissected away from the subscapularis and the vessels running in the bicipital groove were protected. The proximal 20 mm segment of the LHBT was released and whipstitched to the adjacent distal 50 mm of the tendon. An 8-mm aperture was drilled with an acorn reamer for the swivel lock tenodesis screw at the middle of the bicipital groove. The swivel lock screw and whipstitch were then advanced into the humerus. When the tension and contour of the biceps were determined to be acceptable, the rescue stitches were passed back through the tendon and sutured to the subscapularis and supraspinatus to repair and close the rotator interval. The passive ROM was stable with no concerning findings. The wound was irrigated with normal saline and closed. A sterile dressing was placed overall incisions and the patient was placed in a sling with an abduction pillow to maintain neutral position of the shoulder. The patient tolerated the procedure with no complications. The patient was last seen at a 28-month follow-up and reported no pain or crepitus and full ROM in the left shoulder and elbow. On examination, the surgical site was well-healed,and gross motor and sensory function were intact. The posterior laxity noted preoperatively was not present and there was no sign of instability in the shoulder. Active ROM was improved in all planes in comparison with those measured at the pre-operative clinic visit. Overall, the patient reported functional improvement and had no limitations due to the shoulder. The patient was seeking medical clearance to join the military and was cleared for full duty.
Discussion
The majority of literature on the topic of medial dislocation of the LHBT asserts that damage to the RC is a frequent, if not requisite, component of dislocation [2, 5, 6, 7, 8]. However, this case as well as the case outlined by Gambill et al. [4] suggests that dislocation of the LHBT is possible with an intact RC and may relate to posterior instability in the glenohumeral joint. Literature supports the existence of isolated biceps tendon dislocations, but the relationship between posterior laxity and LHBT dislocation has not been explored [5, 10]. In addition to its role in moving the shoulder, the RC serves an important stabilizer of the LHBT [1]. The superior transverse humeral ligament, SGHL, and the CHL provide added ligamentous support to the area and serve to form a sling that secures the LHBT in between the greater and lesser tubercles of the humerus in an area called the intertubercular sulcus or bicipital groove. The subscapularis aids in maintaining the LHBT in the bicipital groove between the greater and lesser tubercles of the humerus by inserting onto the lesser tuberosity of the humerus. The transverse ligament is thought to be simply an extension of the subscapularis tendon and some authors contend that the transverse humeral ligament may not exist at all [2, 3,6, 7]. Interestingly, in ourcase the transverse ligament, SGHL, and CHL were all injured and had an associated medial dislocation of the LHBT without associated RC injury, which further demonstrates the importance of the ligamentous support that these structures provide for the LHBT stability (Fig. 5) [9, 11, 12, 13, 14]. The purpose of the LHBT is still under investigation. Some authors suggest that the LHBT serves to depress the humeral head; others report that the LHBT supports the glenohumeral joint, especially in the unstable shoulder [9,11]. In the case outlined by Gambill et al. [4], a medial dislocation of the LHBT was noted with intact subscapularis, supraspinatus, and infraspinatus in addition to post-traumatic posterior laxity from a previous injury. This reported case was similar to ours in several regards: Both patients reported symptoms beginning after a forceful adduction injury, both had posterior glenohumeral instability noted on examination and intraoperatively, both had injured transverse ligament, SGHL, and CHL with no corresponding RC tendon injury, and both had successful relief of symptoms with biceps tenodesis. However, debate still continues on whether biceps tenotomy or biceps tenodesis is superior in treating LHBT dislocation [14, 15, 16, 17, 18].In a comprehensive review by Ribeiro et al. [14], they were unable to determine a superior treatment modality [8, 10, 11, 12,15]. The results of our case and the case reported by Gambill et al. [4] suggested that a biceps tenodesis and rotator closure were an acceptable treatment for this rare condition that can provide patients with not only symptomatic relief but also improvement in functional status. However, both patients were young and active making them ideal candidates for tenodesis [8, 10, 13, 14].Another interesting aspect of this case was that an open procedure was performed for the rotator closure and biceps tenodesis due to surgeon preference; and literature has not demonstrated superior results between open andarthroscopic tenodesis [19, 20]. Despite similar presentations with posterior laxity on the exam, there was a difference between our case and the Gambill et al. case in the extent of damage to the posterior capsule. The patient in the Gambill et al. [4] case had a posterior labral tear while our patient had an intact labrum, but a capacious posterior capsule. Hence, they proceeded to provide the posterior repair with their patient with a suture and anchor repair of the posterior labrum, and we performed a posterior capulorrhaphy. Nevertheless, both patients were seen 2 years postoperatively and reported no problems with shoulder instability. Both patients reported full functional recovery, with our patient being cleared for active military duty. The case presented by Gambill et al. [4] and our case suggested that posterior instability may be associated with medial dislocation of the LHBT. Nevertheless, more studies are needed to assess the role of posterior glenohumeral instability and capsular laxity in the pathogenesis of medial dislocation of the LHBT. Furthermore, additional studies need to investigate the optimal operative treatment of posterior laxity with concomitant medial dislocation of the LHBT; however, these two cases suggested that addressing the posterior laxity operatively and performing a biceps tenodesis with a rotator interval closure is onemodality for successful treatment of this injury pattern in the young active patient.
Conclusion
This case demonstrated that the medial dislocation of the LHBT can occur without injury to the subscapularis tendon. Furthermore, a capsulorrhaphy with open biceps tenodesis and closure of the rotator interval may provide a successful outcome for this rare injury pattern.
Clinical Message
This case report demonstrates a successful treatment outcome for isolated medial dislocation of long head of biceps without an associated rotator cuff tear. This case report also helps illustrate the complex anatomy of the long head of the biceps with relation to the biceps pulley, so a provider can help understand this rare pathology.
References
1. Ditsios K, Agathangelidis F, Boutsiadis A, Karataglis D, Papadopoulos P. Long head of the biceps pathology combined with rotator cuff tears. Adv Orthop2012;2012:405472.
2. MacDonald K, Bridger J, Cash C, Parkin I. Transverse humeral ligament: Does it exist? Clin Anat2007;20:663-7.
3. Gleason PD, Beall DP, Sanders TG, Bond JL, Ly JQ, Holland LL, et al. The transverse humeral ligament: A separate anatomical structure or a continuation of the osseous attachment of the rotator cuff? Am J Sports Med 2006;34:72-7.
4. Gambill ML, Mologne TS, Provencher MT. Dislocation of the long head of the biceps tendon with intact subscapularis and supraspinatus tendons. J Shoulder Elbow Surg 2006;15:e20-2.
5. Walch G, Nové-Josserand L, Boileau P, Levigne C. Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 1998;7:100-8.
6. Lafosse L, Reiland Y, Baier GP, Toussaint B, Jost B. Anterior and posterior instability of the long head of the biceps tendon in rotator cuff tears: A new classification based on arthroscopic observations. Arthroscopy 2007;23:73-80.
7. Rokito AS, Bilgen OF, Zuckerman JD, Cuomo F. Medial dislocation of the long head of the biceps tendon. Magnetic resonance imaging evaluation. Am J Orthop (Belle Mead NJ) 1996;25:314, 318-23.
8. Kang Y, Lee JW, Ahn JM, Lee E, Kang HS. Instability of the long head of the biceps tendon in patients with rotator cuff tear: Evaluation on magnetic resonance arthrography of the shoulder with arthroscopic correlation. Skeletal Radiol2017;46:1335-42.
9. Khazzam M, George MS, Churchill RS, Kuhn JE. Disorders of the long head of biceps tendon. J Shoulder Elbow Surg 2012;21:136-45.
10. Schaeffeler C, Waldt S, Holzapfel K, Kirchhoff C, Jungmann PM, Wolf P, et al. Lesions of the biceps pulley: Diagnostic accuracy of MR arthrography of the shoulder and evaluation of previously described and new diagnostic signs. Radiology 2012;264:504-13.
11. Bennett WF. Arthroscopic repair of anterosuperior (supraspinatus/subscapularis) rotator cuff tears: A prospective cohort with 2- to 4-year follow-up. Classification of biceps subluxation/instability. Arthroscopy 2003;19:21-33.
12. Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML. Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-40.
13. Frank RM, Taylor D, Verma NN, Romeo AA, Mologne TS, Provencher MT, et al. The rotator interval of the shoulder: Implications in the treatment of shoulder instability. Orthop J Sports Med 2015;3:2325967115621494.
14. Ribeiro FR, Ursolino AP, Ramos VF, Takesian FH, Tenor Júnior AC, Costa MP, et al.Disorders of the long head of the biceps: Tenotomy versus tenodesis. Rev Bras Ortop2017;52:291-7.
15. Gill TJ, McIrvin E, Mair SD, Hawkins RJ. Results of biceps tenotomy for treatment of pathology of the long head of the biceps brachii. J Shoulder Elbow Surg 2001;10:247-9.
16. Osbahr DC, Diamond AB, Speer KP. The cosmetic appearance of the biceps muscle after long-head tenotomy versus tenodesis. Arthroscopy 2002;18:483-7.
17. The B, Brutty M, Wang A, Campbell PT, Halliday MJ, Ackland TR, et al. Long-term functional results and isokinetic strength evaluation after arthroscopic tenotomy of the long head of biceps tendon. Int J Shoulder Surg 2014;8:76-80.
18. Friedman JL, FitzPatrick JL, Rylander LS, Bennett C, Vidal AF, McCarty EC, et al. Biceps tenotomy versus tenodesis in active patients younger than 55 years: Is there a difference in strength and outcomes? Orthop J Sports Med 2015;3:2325967115570848.
19. Johannsen AM, Macalena JA, Carson EW, Tompkins M. Anatomic and radiographic comparison of arthroscopic suprapectoral and open subpectoral biceps tenodesis sites. Am J Sports Med 2013;41:2919-24.
20. Werner BC, Evans CL, Holzgrefe RE, Tuman JM, Hart JM, Carson EW, et al. Arthroscopic suprapectoral and open subpectoral biceps tenodesis: A comparison of minimum 2-year clinical outcomes. Am J Sports Med 2014;42:2583-90.
 |
 |
 |
 |
 |
| Dr. Matthew L Vopat | Dr. Shang-You Yang | Dr. Cole Mc Gregor | Dr. K James Kallail | Dr. Bradley M Saunders |
| How to Cite This Article: Vopat M L, Yang S, Mc Gregor C, Kallail K J, Saunders BM. Medial Dislocation of the Long Head of the Biceps without Concomitant Subscapularis Tear: A Case Report. Journal of Orthopaedic Case Reports 2019 Nov-Dec; 9(6): 6-10. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


