
[box type=”bio”] Learning Point of the Article: [/box]
Press fit unicortical non vascularized fibular graft with a stable fixation is a good treatment modality for monostotic fibrous dysplasia.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 19-22 | Swapnil M Keny, Dhiraj V Sonawane, Bipul K Garg, Shrikant P Savant. DOI: 10.13107/jocr.2019.v09.i06.1570
Authors: Swapnil M Keny[1], Dhiraj V Sonawane[1], Bipul K Garg[1], Shrikant P Savant[1]
[1]Department of Orthopaedic Surgery, Sir J.J. Group of Hospitals and Grant Medical College, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Bipul K Garg,
Department of Orthopaedic Surgery, Sir J.J. Group of Hospitals and Grant Medical College, Mumbai – 400 008, Maharashtra, India.
E-mail: garg.bipul@gmail.com
Abstract
Introduction: Fibrous Dysplasia is a relatively rare Musculoskeletal disorders in which there is a defect in remodelling of immature bone to mature lamellar bone. Fibrous Dysplasia was first described by Von Recklinghausen in 1891, but it was Lichtenstein who labelled it polyostotic Fibrous Dysplasia in 1938. Union of Pathological Fractures in a bone affected by Fibrous Dysplasia poses a difficult set of Challenges for treating Physicians.
Case Report: We Report a 24 year-old female patient with a Pathological Fracture of the Tibia in a Monostotic Anterior Cortical Fibrous Dysplasia Hybrid Fixation with a UnicorticalOsteoperisoteal Non Vascularized Fibula Graft with a follow up until the union of fracture site on computed tomography scan and complete integration of unicorticalosteoperiosteal fibular graft .
Conclusion: We provide additional and independent evidence that removal of the diseased cortex which were parts of the proximal and distal fragment and reconstruction of the defect in the cortex with a press- fitunicortical Non vascularized osteoperiosteal fibular strut graft with a hybrid fixation is a good treatment modality for monostotic fibrous dysplasia. Hybrid fixation includes retrograde intramedullary transarticular rodding extending across the subtalar and ankle joint into the tibia and augmentation of the primary fixation with a mono-planar rail Fixation in compression mode.
Keywords: Fibrous dysplasia, non – vascularized, osteoperiosteal fibular strut grafting, monostotic.
Introduction
Fibrous Dysplasia was first described by Von Recklinghausen in 1891, but it was Lichtenstein who labelled it polyostotic Fibrous Dysplasia in 1938 [1]. Fibrous Dysplasia is a benign developmental anomaly of the cortex or the corticomedullary region of a bone ,characterized by failure in the remodeling of primitive bone to mature lamellar bone and a failure of the bone to realign in response to mechanical stress [2]. Failure of maturation leaves a mass of immature isolated trabeculae, enmeshed in dysplastic fibrous tissue that is turning over constantly but never completing the remodeling process. In addition, the immature matrix does not mineralize normally [2]. Thus a combination of a lack of stress-bearing alignment and insufficient mineralization results in delayed and poor fracture healing in these bones . It accounts for about 5-7% of all benign bone tumors [2]. The lesions of fibrous dysplasia develop during skeletal growth and have a variable natural evolution. Clinical presentation may occur at any age, with the majority of lesions being detected by the age of 30 years [2]. The disease has no gender predilection. Common sites of skeletal involvement are long bones, ribs, craniofacial bones, and pelvis . The Lesions may affect a single bone (monostotic) or may involve multiple bones (polyostotic) and may be associated with other conditions like McCune Albright Disease and Mazabraud Disease [3]. The surgical treatment for complications associated with this condition is a challenge for surgeons due to the inherent deformities, poor bone quality, delay in healing time and choice of optimum implants. There are no clear surgical guidelines established for the management of pathological fractures in these patients. Various surgical treatment modalities have been reported based on the age of the patient, the location and type of lesion, conventional surgical procedures such as curettage or en bloc resection with cortical bone grafting in monostotic lesions and osteotomies with internal fixation [1] are advocated to correct deformities in polyostotic lesions [4] Bone grafting may be indicated in select adult patients with monostotic disease [5]. Dicaprio and Enneking have reported that cortical strut grafting was effective in strengthening the bone in proximal femur [6].
Case Report
A 24 year old Female presented to our centre with the left sided mid-shaft tibia fracture following a trivial trauma. The patient had previous history of fracture in the same limb 14 years ago which was treated conservatively. On clinical examination, there was anterior bowing of the left leg with pain and mobility at the fracture site. The Radiographs showed multiple, multiloculated cystic lesions with ground glass diffuse rarefaction on the anteromedial cortex of midshaft tibia, with a transverse fracture line through the lesion. This was Suggestive of a pathological fracture in a predominantly anterior corticomedullary Fibrous Dysplasia (Fig. 1). A Radiological Skeletal Survey did not reveal involvement of any other bones. (Fig. 2)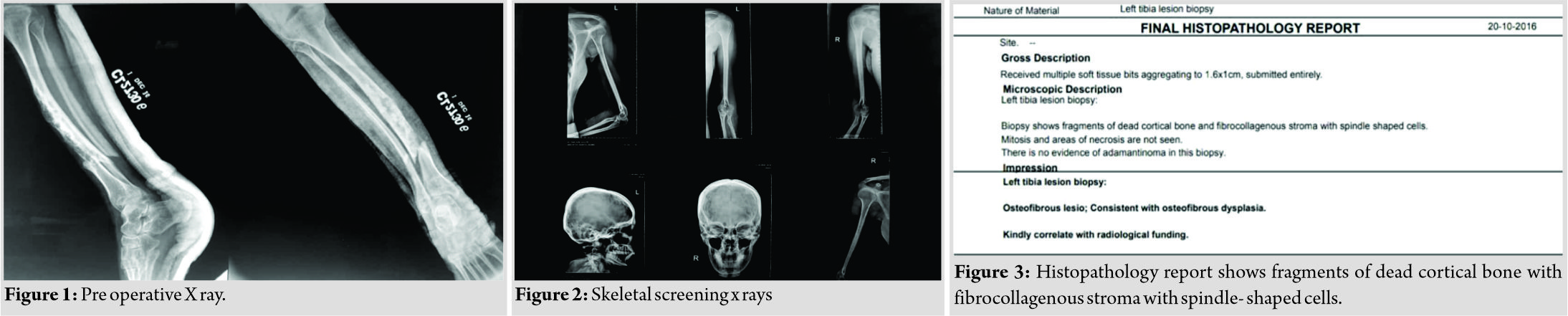
Histopathological biopsy showed fragments of dead cortical bone and fibrocollagenous stroma with spindle shaped cells confirming an osteofibrous Dysplasia (Fig. 3). The patient was managed with removal of the diseased anterior cortex which were parts of the proximal and distalfragments, reconstruction of the defect in the anterior cortex with a press-fit unicortical nonvascularized osteoperiosteal fibular strut graft with a retrograde intramedullary (IM) transarticular rodding- extending across the subtalar and ankle joint into the tibia. Augmentation of the primary fixation was done with a monoplanar Rail Fixation in Compression Mode (Fig. 4).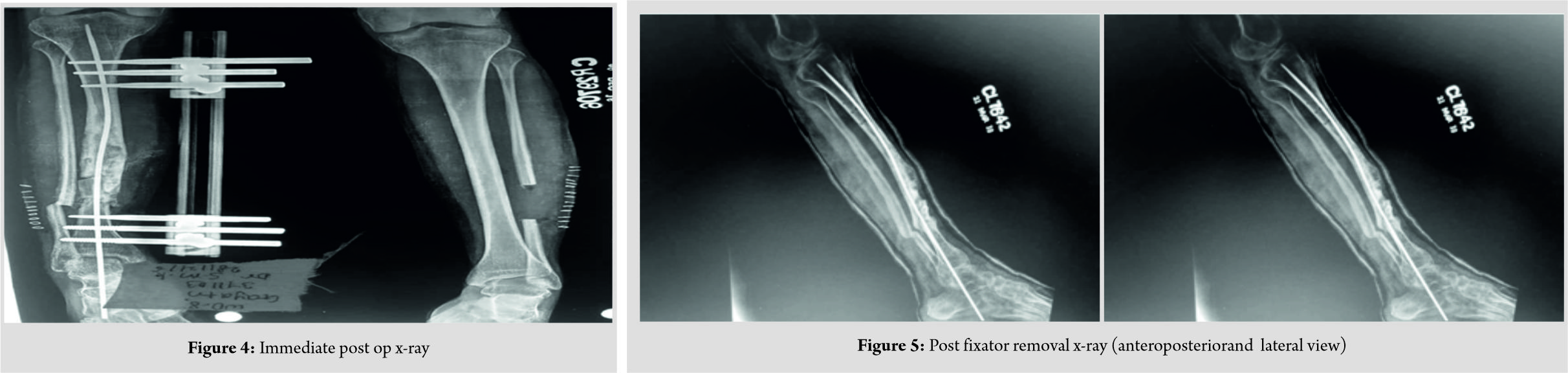 Union was assessed on periodic x-rays (Fig. 5) and confirmed on a computed tomography scan (Fig. 6) when a Bridging Trabecular Pattern was seen across the fracture site and there was evidence of Radiological Fusion of the Proximal and Distal Ends of the Osteoperiosteal Graft with the Anterior Cortical Edges of the Bone. The Fracture Healing time was 22 months and the time in Fixator was 26 Months. The Rod was Left in situ to augment Structural integrity. The patient was mobilized with walker assisted toe-touch weight bearing using a clamp shell-typenon-Articulated Orthosis extending from below knee to the foot.
Union was assessed on periodic x-rays (Fig. 5) and confirmed on a computed tomography scan (Fig. 6) when a Bridging Trabecular Pattern was seen across the fracture site and there was evidence of Radiological Fusion of the Proximal and Distal Ends of the Osteoperiosteal Graft with the Anterior Cortical Edges of the Bone. The Fracture Healing time was 22 months and the time in Fixator was 26 Months. The Rod was Left in situ to augment Structural integrity. The patient was mobilized with walker assisted toe-touch weight bearing using a clamp shell-typenon-Articulated Orthosis extending from below knee to the foot.
Discussion
Osteofibrous dysplasia is a developmental Anomaly of the bone with varied involvement and manifestations. It is monostotic in 70-80% of cases and polyostotic in 20-30% [3]. The average age of presentation is before the age of 30 years 3. We have reported a rare case of Monostoticlesion Corticomedullary lesion with pathological fracture after skeletal maturity which was managed by Excision of the Diseased Bone Involving the Fracture site, IMnailing, reconstruction of the Anterior Defect with a Cortical Non vascularized Osteoperiosteal Fibular Strut graft and Augmentation of the Construct with a Monoplanar Rail Fixator in Compression Mode. Non vascularized Fibula Strut Grafting has been Widely Reported as a method of reconstruction of bones after excision of benign and malignant Tumours [5]. Apart from Providing Immediate Structural Strength to the bone-implant Construct, a Fibular graft Also Provides the Necessary length for required for complex reconstructions. The use of non-vascularized fibula grafts originated at the beginning of the 20thcentury and was the gold standard for biological reconstructions for more than 60 years. Advantages of this method compared to the use of vascularized auto-grafts consist of the remodeling capacity at the donor site, an easier operative technique and a shorter operative time. The integration of avascular grafts could be attributed to a periosteal hypertrophy leading to the new bone formation around the graft and eventual bony integration of the graft in some cases [7]. The other modes are vascularized fibular grafting. Vascularized grafts are harvested using a posterolateral approach with preservation of the periosteum. Hypertrophy of vascularized fibular grafts as described in literature varies from 37% to 90% [5]. Hypertrophy was more prevalent in the presence of mechanical loading and was achieved earlier in younger patients and in grafts that were not internally fixed with a nail or a plate [5]. Recurrence of the dysplastic lesions if autogenous cancellous bone grafts were used led to treatment with cortical fibular grafts [2]. Cortical bone Grafting has been reported as a superior alternative to cancellous grafts and bone substitutes in Fibrous Dysplasia[6]. On the other hand, vascularized bone grafts also provide a safe and reliable means of ensuring good continuity of bone with little risk of recurrence and failure [2]. In the Reported case , the diseased Lesion involved the Anterior cortex of the tibia which needed an Extraperiosteal Resection of the Diseased Bone to Freshen the Edges of the Fracture Edges . Hence an osteoperiostealnon vascularized Free fibular graft from the Contralateral Limb was used to Reconstruct the Anterior Cortex with the Superior and inferior edges of the graft wedged between the proximal and Distal fragments in the form of a press fit. Since the Medullary Canal at the Fracture site was narrow, 4 mm Elastic Titanium Rod was Inserted Retrograde from the Calcaneum across the Subtalar and Tibio-Talar Joints akin to a fixation for Congenital Tibial Pseudarthrosis. This Rod traversed the Medullary canal, Posterior to the Fibular Strut Graft. This Fixation was further Augmented with a Rail Type of External Fixator in compression Mode to Keep the Fibular Graft Aligned to the Fracture Site. The new bone formed after fractures and corrective osteotomies is dysplastic, thus recurrent fractures and deformity should be expected. In virtually all cases, the cortex of the femur and tibia is severely compromised, and therefore the use of typical plate and screw devices is discouraged, unless screws can be placed outside the FD lesions obtaining purchase in normal cortical bone [4]. When screws are used, augmentation with external devices (cast or brace) may be indicated . The use of (IM) devices is strongly suggested for all lower extremity fractures and reconstructions [4]. Such Types of Augmented Constructs are Described in the management of Pathological Bones in Osteofibrous Dysplasia and Congenital Tibial pseudarthrosis where there is a Fracture and the IM Fixation devices needs to be kept for a prolonged Period of time. Though the Fracture Had healed and the Fibula had integrated with the Cortices of the Tibia, a part of the Medial Cortex which was involved in the disease but was not a part of the fracture fragments was left intact. Hence the Intramedullary Rod was left insitu and the patient was Mobilized using a Non-Articulatedbelow-knee Ankle Spanning Orthosis.
Conclusion
Fibrous Dysplasia often presents with a wide range of clinical symptoms and sometimes with an unpredictable clinical course requiring multiple surgical as well as non-surgical interventions. We provide additional and independent evidence that removal of the diseased cortex which was parts of the proximal and Distal Fragment and reconstruction of the defect in the cortex with a press-fitunicorticalNon vascularized Osteoperiosteal fibular strut graft with hybrid fixation is a good treatment modality for monostsotic fibrous dysplasia. Hybrid fixation includes- a retrogradeI Mtransarticular rodding extending across the subtalar and ankle joint into the Tibia and augmentation of the primary fixation with a monoplanarrail Fixation in compression mode.
Clinical Message
Removal of the diseased cortex which were parts of the proximal and distal fragment, reconstruction of the defect in the cortex with a press-fit unicortical non – vascularized osteoperiosteal fibular strut graft with a hybrid fixation, is a good treatment modality for monostotic fibrous dysplasia.
References
1. Zhang X, Shang X, Wang Y, He R, Shi G. Intramedullary nailing for fibrous dysplasia of lower limbs. Oncol Lett 2012;4:524-8.
2. DiCaprio MR, Enneking WF. Fibrous dysplasia. pathophysiology, evaluation, and treatment. J Bone Joint Surg Am 2005;87:1848-64.
3. Muthusamy S, Subhawong T, Conway SA, Temple HT. Locally aggressive fibrous dysplasia mimicking malignancy: A report of four cases and review of the literature. Clin OrthopRelat Res 2015;473:742-50.
4. Ippolito E, Lindaman L, Wientroub S, Leet A, Stanton RP, Springfield D. The Surgical Management of Fibrous Dysplasia of Bone. Orphanet J Rare Dis 2012;7 Suppl 1:S1.
5. Krieg AH, Hefti F. Reconstruction with non-vascularised fibular grafts after resection of bone tumours. J Bone Joint Surg Br 2007;89:215-21.
6. Vipan K, Badole CM, Wandile K. Management of a case of fibrous dysplasia with pathological fracture of proximal femur. J Mahatma Gandhi Inst Med Sci 2013;18:52-4.
7. Lenze U, Kasal S, Hefti F, Krieg AH. Non-vascularised fibula grafts for reconstruction of segmental and hemicortical bone defects following meta-/diaphyseal tumour resection at the extremities. BMC Musculoskelet Disord2017;18:289.
 |
 |
 |
 |
| Dr. Swapnil M Keny | Dr. Dhiraj V Sonawane | Dr. Bipul K Garg | Dr. Shrikant P Savant |
| How to Cite This Article: Keny S M, Sonawane D V, Garg B K, Savant S P. Pathological Fracture of the Tibia in a Monostotic Anterior Cortical Fibrous Dysplasia: Hybrid Fixation with Unicortical Osteoperiosteal Non-Vascularized Fibula Graft – A Case Report. Journal of Orthopaedic Case Reports 2019 Nov-Dec;9(6): 19-22. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


