
[box type=”bio”] Learning Point of the Article: [/box]
Arm Board Technique allows unhindered access to the elbow, makes fracture reduction and wire fixation much easier and it’s easier to obtain a true lateral radiographic image, as well as to assess stability post-fixation, obviates the need for a surgical assistant, allows converting the closed reduction to open reduction in difficult situations and is also safe for the radiographic equipment.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 98-101 | Vivek M Sodhai, Sandeep A Patwardhan, Samuel O Alao, Ashok K Shyam, Askhar Haphiz. DOI: 10.13107/jocr.2019.v09.i06.1608
Authors: Vivek M Sodhai[1], Sandeep A Patwardhan[1], Samuel O Alao[2], Ashok K Shyam[1],[3], Askhar Haphiz[1]
[1]Department of Paediatric Orthopaedics, Sancheti Institute for Orthopaedics and Rehabilitation, Pune, Maharashtra, India,
[2]Department of Orthopaedics, Paediatric Orthopaedic Unit, Trauma and Surgical Centre, University of Medical Sciences Teaching Hospital, Ondo, Nigeria,
[3]Department of Research, Indian Orthopaedic Research Group, Thane (W), Maharashtra, India.
Address of Correspondence:
Dr. Vivek M Sodhai,
Department of Paediatric Orthopaedics, Sancheti Institute for Orthopaedics and Rehabilitation, 16, Shivaji Nagar, Pune – 411005, Maharashtra, India.
E-mail: vivek.sodhai89@gmail.com
Abstract
Introduction: Closed reduction percutaneous pinning (CRPP) is the current standard of treatment for displaced supracondylar fractures of humerus in children. This technical note describes a simple method of CRPP using a radiolucent arm board and simpler handling of the C-arm. This technique is a simple method and easy to reproduce, can be adapted to any standard operating table, and gives predictable results.
Keywords: Arm board technique, closed reduction percutaneous pinning, pediatric supracondylar humeral fractures.
Introduction
Supracondylar humeral fracture (SCH) is the most common elbow fracture in children [1], 97–99% of these fractures are of the extension type [2] and have been further classified by Gartland [3] into four types, namely, Type 1 (undisplaced), Type 2 (displaced with an intact posterior cortex), Type 3 (completely displaced, posteromedially or posterolaterally), and Type 4 (associated with circumferential periosteal disruption and multidirectional instability). At present, the standard of care for the management of Types 2 and 3 displaced fractures is closed reduction percutaneous pinning (CRPP) [4, 5]. Various authors have described various techniques for CRPP of these fractures [6, 7, 8, 9, 10, 11]. Based on the aforementioned perceived shortcomings of the existing techniques described in textbooks and journal articles, the senior author devised a simple and unique method of positioning the elbow/arm which makes fracture reduction and pinning easier and faster. A surgical assistant is not required and the technique has been used successfully for over 10 years.
The Technique (Video 1)
| https://www.youtube.com/watch?v=vskVt6oOlIY&t=5s |
Positioning
Under general anesthesia and supine position, the patient is positioned supine with the affected limb abducted to 90°. The arm is positioned on a specially fabricated, length adjustable radiolucent arm board. The board is adjusted to support the arm proximal to the fracture site. The elbow and the distal part of the limb are completely free to ease fracture reduction and pinning. The proximal arm is fixed to the board with a broad hypoallergenic adhesive tape to stabilize the proximal fragment, i.e., proximal to the fracture site (Fig. 1). The distal fragment is kept free for the ease of reduction and pinning. The image intensifier is positioned parallel to the foot end of the table on the same side as the injured limb and surgeon while the monitor is positioned on the contralateral side opposite the surgeon for easy visualization of the images (Fig. 2).
Reduction
The elbow is extended and the C-arm is used to check if the fracture is out to length (Fig. 3). To achieve reduction, the surgeon grasps the forearm, applies gentle longitudinal traction and by giving pressure with the thumb, the flexion of the distal fragment is done (Fig. 4a and b). There is no need for assisted countertraction because the proximal limb segment is immobilized to the board. Varus and valgus malalignment, mediolateral translation, as well as rotational displacements are corrected; the elbow is then flexed to 120° (Fig. 4c).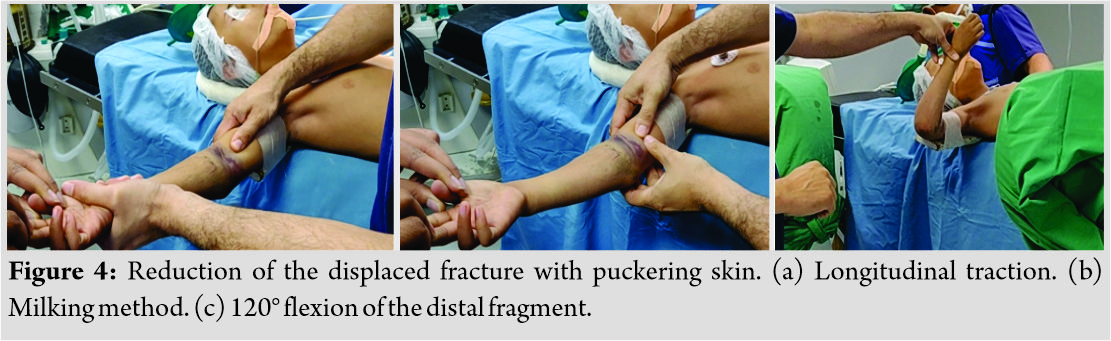 The acceptability of reduction is confirmed with the C-arm in anteroposterior and lateral views by rotating the C-arm 180° without moving the limb (Fig. 5). The limb is held in this position, prepared, and draped with pediatric O-sheet (Fig. 6).
The acceptability of reduction is confirmed with the C-arm in anteroposterior and lateral views by rotating the C-arm 180° without moving the limb (Fig. 5). The limb is held in this position, prepared, and draped with pediatric O-sheet (Fig. 6).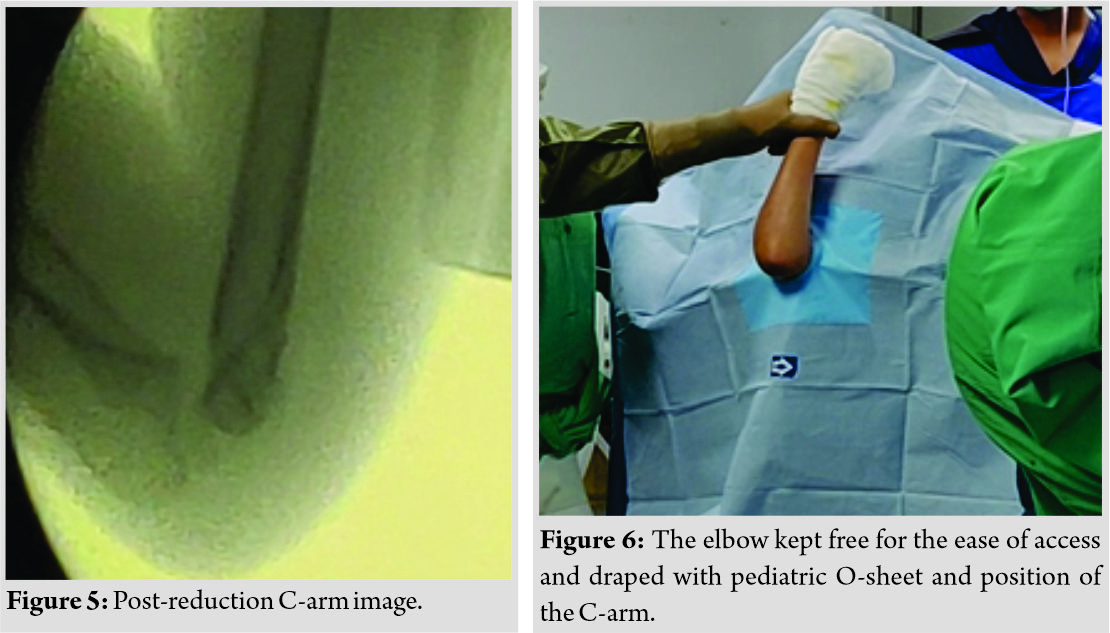
Pinning
Following draping, the acceptability of reduction is confirmed with the C-arm and if need be the reduction maneuver is repeated. The first lateral pin (1.6mm Kirchner wire for a smaller child; 2.0mm for a bigger child) is the olecranon fossa pin with tetracortical purchase passing from the lateral condyle across the olecranon fossa to engage the medial cortex (Fig. 7a and b).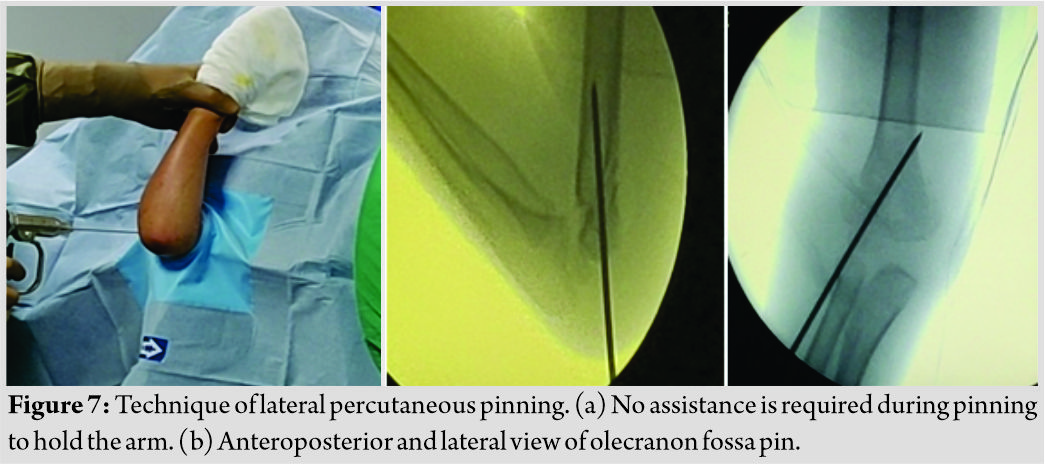 After the first pin, C-arm is rotated 180° to visualize the fixation in anteroposterior, medial, and lateral oblique views (Fig. 8). The second lateral pin is the lateral pillar pin which is placed parallel to or divergent from the first pin and is bicortical (Fig. 9).
After the first pin, C-arm is rotated 180° to visualize the fixation in anteroposterior, medial, and lateral oblique views (Fig. 8). The second lateral pin is the lateral pillar pin which is placed parallel to or divergent from the first pin and is bicortical (Fig. 9).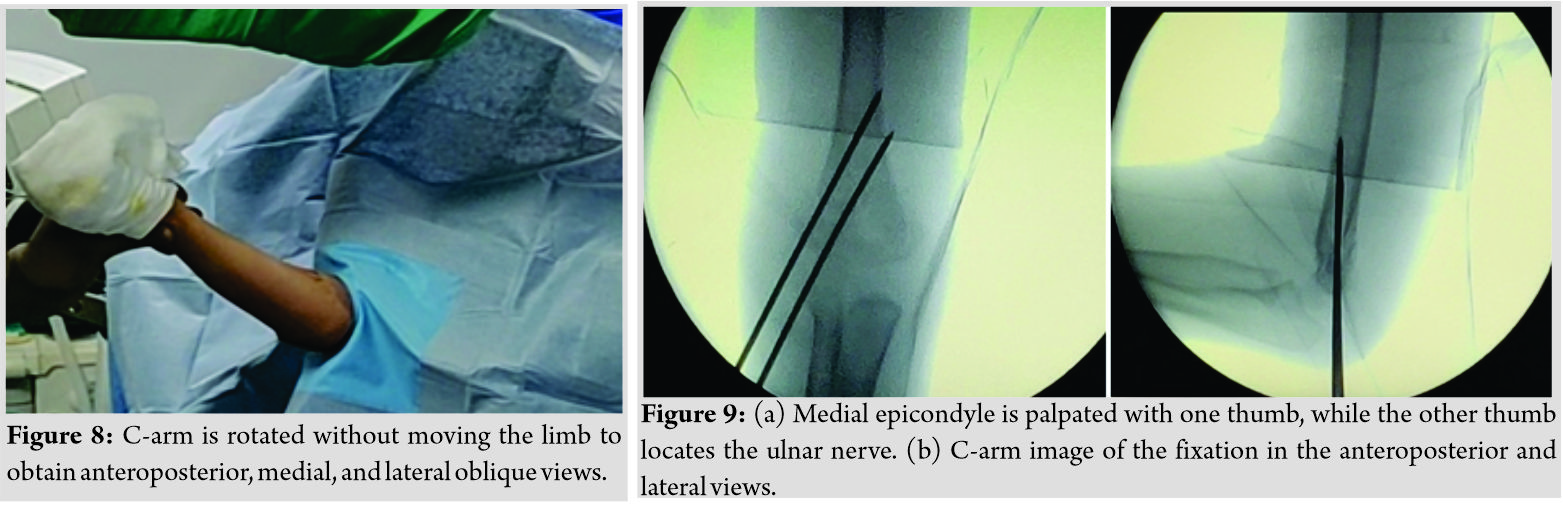 After the second pin, the laxity of the adhesive tape allows checking the stability of the fracture with imaging by gently rotating the shoulder externally and internally (Fig. 10a and b). If the stability is unsatisfactory as occurs usually in comminuted fractures, a third K-wire is then added parallel to the first two pins laterally or in a cross fashion medially.
After the second pin, the laxity of the adhesive tape allows checking the stability of the fracture with imaging by gently rotating the shoulder externally and internally (Fig. 10a and b). If the stability is unsatisfactory as occurs usually in comminuted fractures, a third K-wire is then added parallel to the first two pins laterally or in a cross fashion medially.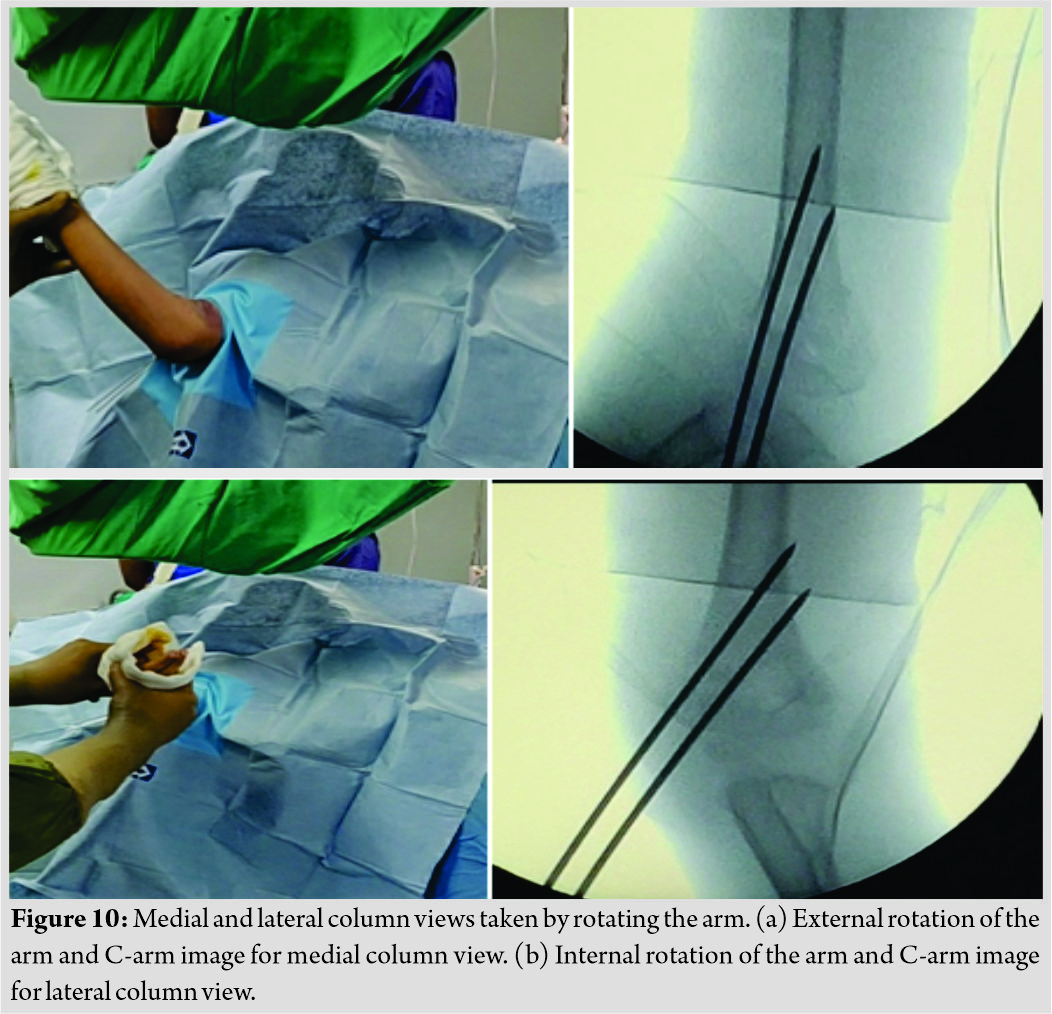
Percutaneous medial pinning (Video 2)
| https://www.youtube.com/watch?v=Fogk2LTV-Is&t=1s |
A medial pin may be indicated in cases of medial oblique fractures where there is a larger medial fragment or in cases of rotational instability. For medial entry pins, the medial epicondyle is palpated; the ulnar nerve is palpated by gently rolling it between the finger and the bone (Fig. 11a). By pushing it posteriorly with the thumb and with the elbow in slightly extended position, the pin is driven from the medial epicondyle in an anteromedial to posterolateral direction to engage the lateral cortex (Fig. 11b and c). The wires are bent to about 100° and cut about 2cm from the skin.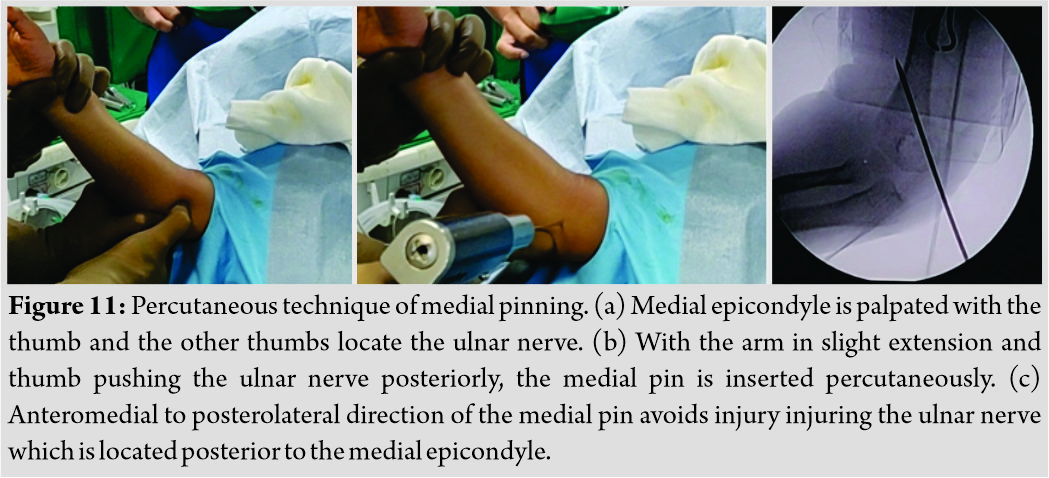
Application of above-elbow cast
Sterile gauze and iodine ointment are applied around the wires; cast padding is applied from the axilla to the metacarpophalangeal joints followed by above-elbow fiberglass cast with the forearm in neutral rotation and the elbow in 90° of flexion. The circulation of the hand is assessed to be adequate by ensuring that the hand is pink and warm with a good capillary refill. The cast is slit on the operation table if there is considerable pre-operative swelling.
Post-operative Care
The child is nursed in the recovery for about an hour until he recovers from anesthesia. The pulse oximeter probe is attached to the thumb of the operated limb to ensure satisfactory perfusion. Post-operative radiographs are then taken. The child is admitted overnight for pain control and regular assessment of the neurocirculatory status of the hand before discharge home the following day. At 3 weeks postoperatively, check radiographs are done. Usually, by then, the fracture would have healed. The cast and pins are removed without anesthesia in the outpatient department. For the older child, pin and cast removal are done at 4 weeks. Active elbow range of motion exercises are then commenced.
Discussion
Several conventional techniques of CRPP are employed by different surgeons for SCH fractures. Mubarak and Davids recommended positioning a bed sheet wrapped around the patient’s torso with which the anesthetist provides counter traction when the surgeon applies traction during fracture reduction [6]. The disadvantage of this is that the airway may be compromised while the anesthetist is distracted by the countertraction. In another technique described by Tolo et al., the surgeon applies traction and his assistant provides countertraction by pushing against the patient’s axilla [7]. Here, a surgical assistant is mandatory. Some surgeons use the receiver arm of the image intensifier as the table to set the injured arm on (i.e.,“elbow on the tube”) [8]. However, this practice prevents rotation of the fluoroscopy unit for lateral images; thus, the limb has to be rotated to take lateral film which may lead to loss of reduction by the maneuvering. The receiver may also be inadvertently damaged by sharp objects, fluids, and power instruments. Jayakumar and Ramachandran used a standard radiolucent arm board with a small folded towel under the child’s elbow (i.e.,“elbow on the table”) during pinning [9]. However, the board often gets in the way and makes manipulation and drilling of the Kirschner wire difficult by not providing enough clearance for the posterior elbow. Guler et al. reported a shorter duration of anesthesia in supine position as compared to prone while fixing SCH fractures [10]. The conventional technique was utilized in the positioning of the patient and required an additional surgical assistant for reducing the fracture. Vuillermin et al. positioned the affected arm on the fluoroscopic detector or hand table for fixing the SCH fractures [11]. Our technique employs a low-tech, locally fabricated radiolucent arm board on which the arm is stabilized with hypoallergenic adhesive tape obviating the need for an additional assistant to give countertraction. The technique allows us to easily move the C-arm to visualize the fracture fixation in anteroposterior, lateral, medial, and lateral oblique views. The technique also allows converting the procedure to open reduction by sliding the arm board to support the forearm and unhindered anterior approach to the elbow.
Conclusion
Our technique employs a low-tech, locally fabricated radiolucent arm board that can be adapted to any standard operating table. It is a novel and innovative method that has been used by the senior author for over 10 years with excellent results. It is safe, effective and can be easily replicated by orthopedic surgeons involved in managing pediatric fractures.
Clinical Message
Arm board technique allows unhindered access to the elbow, makes fracture reduction and wire fixation much easier. It is easier to obtain a true lateral radiographic image, as well as to assess stability post-fixation, obviates the need for a surgical assistant, allows converting the closed reduction to open reduction in difficult situations, and is also safe for the radiographic equipment.
References
1. Beaty JHKJ. Supracondylar fractures of the distal humerus. In: Beaty JH, Kasser JR, editors. Rockwood and Wilkins’ Fractures in Children. 6th ed. Philadelphia: Lippincott Williams and Wilkins; 2006. p. 543-89.
2. Cheng JC, Lam TP, Maffulli N. Epidemiological features of supracondylar fractures of the humerus in Chinese children. J PediatrOrthop B 2001;10:63-7.
3. Gartland JJ. Management of supracondylar fractures of the humerus in children. Surg GynecolObstet1959;109:145-54.
4. Skaggs DL, Sankar WN, Albrektson J, Vaishnav S, Choi PD, Kay RM. How safe is the operative treatment of gartland Type 2 supracondylar humerus fractures in children? J PediatrOrthop2008;28:139-41.
5. Skaggs DL, Cluck MW, Mostofi A, Flynn JM, Kay RM. Lateral-entry pin fixation in the management of supracondylar fractures in children. J Bone Joint Surg Am 2004;86:702-7.
6. Mubarak SJ, Davids JR. Closed reduction and percutaneous pinning of supracondylar fractures of the distal humerus in the child. In: Morey BF, editor. The Elbow. Philadelphia, PA: Lippincott Williams and Wilkins; 2014. p. 54-65.
7. Tolo VT, Skaggs DLet al. Master Techniques in Orthopaedic Surgery: PaediatricOrthopaedics. Philadelphia: Lippincott; 2007. p. 1-15.
8. Slongo T, Schmid T, Wilkins K, Joeris A. Lateral external fixationa new surgical technique for displaced unreducible supracondylar humeral fractures in children. J Bone Joint Surg Am 2008;90:1690-7.
9. Jayakumar P, Ramachandran M. Elbow Injuries in Children. In: Bentley G, editors. European Surgical Orthopaedics and Traumatology. Berlin, Heidelberg: Springer; 2014.
10. Guler O, Mutlu S, Isyar M, Mutlu H, Cerci H, Mahirogullari M. Prone versus supine position during surgery for supracondylar humeral fractures. J Orthop Surg (Hong Kong) 2016;24:167-9.
11. Vuillermin C, May C, Kasser J. Closed reduction and percutaneous pinning of pediatric supracondylar humeral fractures. JBJS Essent Surg Tech 2018;8:e10.
 |
 |
 |
 |
 |
| Dr. Vivek M Sodhai | Dr. Sandeep A Patwardhan | Dr. Samuel O Alao | Dr. Ashok K Shyam | Dr. Askhar Haphiz |
| How to Cite This Article: Sodhai VM, Patwardhan SA, Alao SO, Shyam AK, Haphiz A. Arm Board Technique for Closed Reduction Percutaneous Pinning of Displaced Supracondylar Fractures of Humerus in Children: Technical Note. Journal of Orthopaedic Case Reports 2019 Nov-Dec;9(6): 98-101. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


