
[box type=”bio”] Learning Point of the Article: [/box]
Large segmental bone defects associated with soft tissue loss pose reconstructive challenges when treating open fractures, but the staged induced membrane technique, combined with appropriate soft tissue coverage, is a reliable method of limb salvage in a healthy patient.
Case Report | Volume 10 | Issue 1 | JOCR January – February 2020 | Page 58-61 | Porter F Young, Phillip Pirgousis, Jonathan R Helms. DOI: 10.13107/jocr.2020.v10.i01.1636
Authors: Porter F Young[1], Phillip Pirgousis[2], Jonathan R Helms[1]
[1]Department of Orthopaedic Surgery and Rehabilitation, University of Florida, Jacksonville, Florida,
[2]Department of Otorhinolaryngology/Head and Neck Surgery, Mayo Clinic Florida, Jacksonville, Florida.
Address of Correspondence:
Dr. Porter F Young,
655 West 8th Street, Jacksonville, 32209 Florida..
E-mail: porter.young@jax.ufl.edu
Abstract
Introduction: Introduction: Gustilo-Anderson type IIIB open fractures are severe injuries associated with multiple complications and threaten the viability of the limb. In addition, large segmental bone defects pose reconstructive challenges when treating open fractures and outcomes can be unpredictable. This case report highlights a good outcome in a patient with a type IIIB open tibia fracture with segmental bone loss that was successfully treated with a staged induced membrane technique and latissimus dorsi free flap.
Case Report: A 17-year-old female sustained a Gustilo-Anderson type IIIB open tibia fracture with segmental bone loss after a motor vehicle collision. While amputation seemed inevitable, her extremity was able to be salvaged using the staged induced membrane technique and free flap coverage. She made an exceptional recovery and at 24-month follow-up, her short form-12 scores and foot and ankle outcome scores were close to the average for a healthy adult.
Conclusion: Our patient’s outcome represents the benefits of a shared decision-making process with a multidisciplinary approach and highlights the benefit of limb salvage in a healthy patient.
Keywords: Trauma, limb salvage, open fracture, induced membrane technique, free tissue flap.
Introduction
Gustilo-Anderson type IIIB open fractures are severe injuries associated with multiple complications and threaten the viability of the limb [1]. The decision for salvage versus amputation is a difficult one with no strong evidence favoring either treatment method. It should be a shared decision-making process involving the patient, family, and the multidisciplinary team treating the patient. In addition, large segmental bone defects pose reconstructive challenges when treating open fractures and outcomes can be unpredictable. This case report highlights a good outcome in a patient with a type IIIB open tibia fracture with segmental bone loss that was successfully treated with a staged induced membrane technique and latissimus dorsi free flap. It will include a review of the literature on outcomes of type III open tibia fractures with associated segmental bone defects to assist with future decision-making in similar scenarios.
Case Report
A 17-year-old female presented to our trauma bay after a motor vehicle collision. She was intubated in the field for a Glasgow Coma Score of 3 and hemodynamic instability. Non-orthopedic injuries included a subdural hematoma, liver and kidney lacerations, facial fractures, and pulmonary contusions. Her orthopedic injuries were a vertical shear pelvic ring injury, an open left Lisfranc injury, and a type IIIB open right tibia fracture with segmental bone loss. The right tibia fracture was grossly contaminated and had a 90cm × 7cm circumferential soft tissue defect (Fig. 1). After appropriate resuscitation, antibiotics, and splinting, she was taken emergently to the operating room for debridement and irrigation of her open fractures.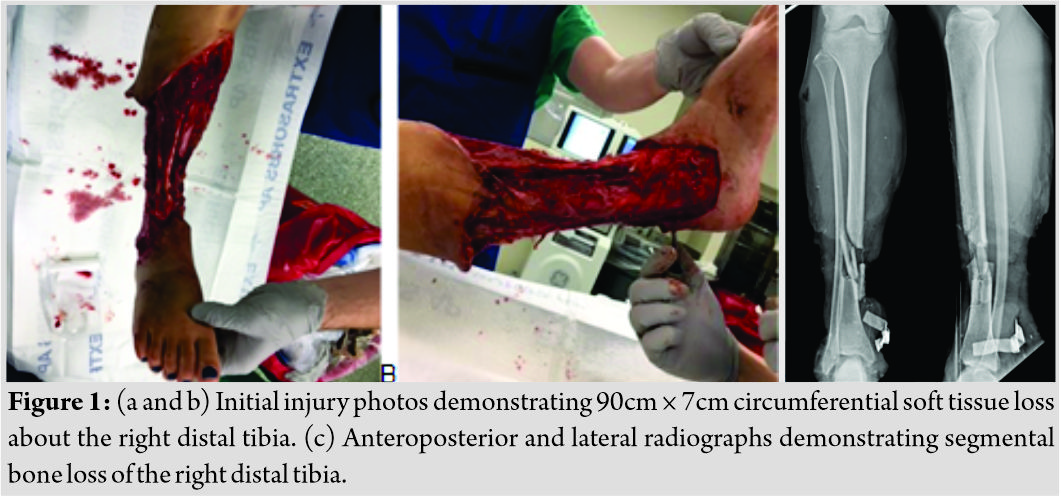
She returned to the operating room on post-injury day 2 and underwent management of her pelvic ring injury. In addition, an antibiotic intramedullary nail was placed into the right tibia, along with an antibiotic cement spacer into the 4 cm bone void (Fig. 2). The oral and maxillofacial microvascular surgery service performed a latissimus dorsi free flap on post-injury day 5. Her free flap was complicated by a pseudomonas aeruginosa infection that was successfully eradicated with intravenous piperacillin-tazobactam. The patient underwent removal of the antibiotic nail and spacer with placement of a tibial nail at the 6-week mark (Synthes North America, West Chester, PA). Autograft was harvested from the ipsilateral femur using a Reamer-Irrigator-Aspirator (RIA; Synthes, West Chester, PA) and placed into the segmental defect along with allograft chips.
Postoperatively, the patient had difficulty with a knee flexion contracture and equinus contracture. She was advanced to 50% weight-bearing at 3 months postoperatively and then weight-bearing as tolerated at 6 months postoperatively. At 10 months, she was able to graduate high school. At 2 years, her knee flexion contracture resolved and she was able to run short distances (Fig. 3). Her equinus contracture persisted but was not severe enough to warrant any intervention. At 24 months, her foot and ankle outcome score was 87 and Shoe Comfort Scale score was 60 (normative values 45 and 45, respectively). Her SF-12 Health Survey physical score was 50.03, which is 0.03 higher than the United States average. Her SF-12 Health Survey mental score was 60.21, which is 10.21 points higher than the United States average. Verbal consent for this case report was received from the patient at the time of her final follow-up.
Discussion
The management of Gustilo-Anderson type IIIB open tibia fractures with bone loss can be challenging due to prolonged recovery time, wound infections, poor patient outcomes, and delayed amputation [1, 2]. The lower extremity assessment project (LEAP) was a multicenter study that provided a foundation for outcomes of lower extremity fractures. It consisted of 601 patients with severe lower extremity fractures that underwent either limb salvage or amputation. Both treatment options were associated with poor functional outcomes. At 7-year follow-up, only 34% of patients achieved functional scores similar to age-matched controls in the general population and only 58% were able to return to work. However, they concluded that outcomes were more influenced by the patient’s medical comorbidities, social, economic, and personal resources rather than the decision to salvage or amputate [3]. Interestingly, Chung et al. performed a cost–utility analysis based on the LEAP data and determined limb salvage to be more costeffective than amputation, independent of prosthetic needs in type IIIB and IIIC open tibia fractures [4]. Reconstruction options for segmental bone loss include synthetic calcium-based fillers, vascularized bone transfer, large cancellous autograft transfer, or intercalary bone transport with distraction osteogenesis [2]. The induced membrane technique, originally developed by Masquelet, is a two-stage procedure that involves the creation of a bioactive membrane around a temporary polymethylmethacrylate (PMMA) cement spacer. Once the membrane is mature, usually in 4–8 weeks, the spacer is removed and the defect is filled with cancellous autograft [5]. If more volume is required to fill the defect, cancellous allograft or demineralized bone matrix can be added for up to 25% of the final graft composition without increased rates of non-unions or complications [6, 7]. The induced membrane prevents graft resorption and secretes growth factors that stimulate graft incorporation [2]. It can be used for up to 25cm defects and reported rates of union at 1 year range from 85% to 100% [8,9]. Mean time to full weight-bearing was 4 months in patients treated with intramedullary nailing, but 8.5 months in patients treated with external fixation [5, 6, 10]. The most common complication encountered is infection with a reported incidence of 0–42%. This is often attributed to inadequate initial debridement before PMMA spacer placement [7, 8, 10].Vascularized bone transfer with a free vascularized fibula graft (FVFG) is versatile option for segmental bone defects 5–20cm in length [11, 12]. The FVFG is supplied by the peroneal artery and can include fascia, muscle, and a skin paddle of up to 20 cm× 10cm, making it a versatile option for bone defects with associated soft tissue loss [11]. Advantages of the FVFG compared to the induced membrane technique include it is a single-stage procedure, decreased infection risk, shorter reconstruction time (average 6–9 months), and potential earlier weight-bearing depending on the form of stabilization utilized [11, 12]. Disadvantages include availability of microsurgical specialists who can perform the technique, up to 35% incidence of stress fractures in the 1stpost-operative year and 30% rate of donor site morbidity with muscle weakness being the most common complication [11, 13]. FVFG may have expedited our patient’s weight-bearing and possibly avoided the equinus and knee flexion contractures. However, we have more experience using the staged induced membrane technique; thus, we felt that it gave the patient the most predictable outcome. Furthermore, we did not think the size of her defect warranted the associated risks of an FVFG. In any open fracture, it is often the soft tissue envelope that most strongly correlates with outcome. Rotational flaps are classically utilized for defects of the proximal two-thirds of the tibia, while free flaps are the mainstay for coverage of the distal tibia [14]. The latissimus dorsi muscle flap is a commonly utilized free tissue transfer for large lower extremity defects. Muscle flaps are rich in vascularity, aiding delivery of nutrients to the injured tissue, and fighting infection. Survival rates for free flaps are 85–96% and complications include partial graft loss (15%), partial flap necrosis (12%), infection (10%), and vascular compromise (8%) [15]. The main disadvantage of free flaps in the lower extremity is the increased rates of flap necrosis when compared to other regions of the body [15]. However, Pollak et al. found a higher rate of wound complications in rotational flaps (44%) compared to free flaps (23%) in tibia fractures with severe underlying osseous injury (ASIF/OTA typeC fractures). The most common wound complication encountered was infection (21%) [14].
Conclusion
Limb salvage of type IIIB tibia fractures with segmental bone loss is associated with frequent complications and overall poor function when compared to age-matched, healthy controls [3]. The patient in our case had an exceptional outcome with 24-month follow-up. Her latissimus flap and tibia healed well despite a superficial wound infection. Her short form-12 scores were above average and her foot and ankle outcome scores were slightly below average for a healthy US adult. She has returned to school and performs daily activities with few issues. Our patient’s outcome represents the benefits of a shared decision-making process with a multidisciplinary approach and highlights the benefit of limb salvage in a healthy patient.
Clinical Message
Limb salvage with the staged induced membrane technique is a reliable technique for restoring function in type III open tibia fractures.
References
1. GustiloRB, MendozaRM, WilliamsDN. Problems in the management of Type III (severe) open fractures: A new classification of Type III open fractures.J Trauma1984;24:742-6.
2. TaylorBC, FrenchBG, FowlerTT, RussellJ, PokaA. Induced membrane technique for reconstruction to manage bone loss.J Am AcadOrthop Surg2012;20:142-50.
3. MacKenzieEJ, BosseMJ. Factors influencing outcome following limb-threatening lower limb trauma: Lessons learned from the lower extremity assessment project (LEAP).J Am AcadOrthop Surg2006;14:S205-10.
4. ChungKC, Saddawi-KonefkaD, HaaseSC, KaulG. A cost-utility analysis of amputation versus salvage for gustilo Type IIIB and IIIC open tibial fractures.PlastReconstr Surg2009;124:1965-73.
5. MasqueletAC, FitoussiF, BegueT, MullerGP. Reconstruction of the long bones by the induced membrane and spongy autograft.Ann ChirPlastEsthet2000;45:346-53.
6. MasqueletAC. Muscle reconstruction in reconstructive surgery: Soft tissue repair and long bone reconstruction.Langenbecks Arch Surg2003;388:344-6.
7. MasqueletAC, BegueT. The concept of induced membrane for reconstruction of long bone defects.Orthop Clin North Am2010;41:27-37.
8. StaffordPR, NorrisBL. Reamer-irrigator-aspirator bone graft and bi masquelet technique for segmental bone defect nonunions: A review of 25 cases.Injury2010;41 Suppl 2:S72-7.
9. McCallTA, BrokawDS, JelenBA, ScheidDK, ScharfenbergerAV, MaarDC, et al. Treatment of large segmental bone defects with reamer-irrigator-aspirator bone graft: Technique and case series.Orthop Clin North Am2010;41:63-73.
10. ApardT, BigorreN, CronierP, DuteilleF, BizotP, MassinP. Two-stage reconstruction of post-traumatic segmental tibia bone loss with nailing.OrthopTraumatol Surg Res2010;96:549-53.
11. MalizosKN, ZalavrasCG, SoucacosPN, BerisAE, UrbaniakJR. Free vascularized fibular grafts for reconstruction of skeletal defects.J Am AcadOrthop Surg2004;12:360-9.
12. MauffreyC, BarlowBT, SmithW. Management of segmental bone defects.J Am AcadOrthop Surg2015;23:143-53.
13. ZhenP, HuYY, LuoZJ, LiuXY, LuH, LiXS. One-stage treatment and reconstruction of gustilo Type III open tibial shaft fractures with a vascularized fibular osteoseptocutaneous flap graft.J Orthop Trauma2010;24:745-51.
14. PollakAN, McCarthyML, BurgessAR. Short-term wound complications after application of flaps for coverage of traumatic soft-tissue defects about the tibia. The lower extremity assessment project (LEAP) study group.J Bone Joint Surg Am2000;82:1681-91.
15. KangMJ, ChungCH, ChangYJ, KimKH. Reconstruction of the lower extremity using free flaps.Arch Plast Surg2013;40:575-83.
 |
 |
 |
| Dr. Porter F Young | Dr. Phillip Pirgousis | Dr. Jonathan R Helms |
| How to Cite This Article: Young PF, Pirgousis P, Helms JR. Maximizing outcomes in a Gustilo-Anderson type IIIB open tibia fracture with segmental bone loss: A case report and review of the literature. Journal of Orthopaedic Case Reports 2020 Jan-Feb;10(1): 58-61. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


