
[box type=”bio”] Learning Point of the Article: [/box]
Anterior dislocation of hip is a rare entity and surgeons should be quite vigilant to diagnose anterior dislocation of hip joint and immediate reduction should be planned. One should also be vigilant regarding associated fractures and appropriate follow up to rule out risks of AVN of femur head.
Case Report | Volume 10 | Issue 1 | JOCR January – February 2020 | Page 62-65 | Jagdeep Singh, Sorabh Garg, Anshul Dahuja, Kapil Bansal. DOI: 10.13107/jocr.2020.v10.i01.1638
Authors: Jagdeep Singh[1], Sorabh Garg[1], Anshul Dahuja[1], Kapil Bansal[1]
[1]Department of Orthopaedics, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India.
Address of Correspondence:
Dr. Sorabh Garg,
Department of Orthopaedics, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India.
E-mail: sorgag@gmail.com
Abstract
Introduction: Anterior dislocation of the hip joint is a rare presentation accounting for around 15% of all hip dislocations. Obturator (inferior) type traumatic anterior hip dislocation in adult is rare of all types of hip dislocation. Here, we described a case with same description. It can occur as a result of a high-energy trauma in circumstances such as a motor vehicle accident or a fall from a significant height. A delay in relocation of more than 6 h has been associated with a high risk of avascular necrosis of the femoral head.
Case Report: We reported the case of a 70-year-old man who suffered an anterior dislocation of his hip joint who was brought to the emergency room with a history of fall from the bicycle hit by a motorcyclist from his back. After examined clinically and radiologically, the patient was diagnosed with obturator type of anterior right hip dislocation. Closed reduction under short general anesthesia was planned.
Conclusion: Inferior hip dislocations are very rarely seen injuries with severe high-energy trauma. The reduction must be done as soon as possible because it involves the functional prognosis of the hip by the risk of necrosis of the femoral head and subsequent osteoarthritis requiring long-term monitoring.
Keywords: Femoral head, hip dislocation, obturator injury.
Introduction
Traumatic hip dislocation is serious injuries that are associated with significant long-term morbidity, most notably avascular necrosis (AVN) and post-traumatic osteoarthritis [1]. Given the inherent stability of the hip due to its osseous, labral, ligamentous, and muscular anatomy, dislocations require significant force and are typically associated with fractures of the acetabulum or femoral head [2]. They typically occur in young patients in the setting of high-energy trauma and are increasing in incidence, predominantly due to motor vehicle crashes, which cause between 62% and 93% of all hip dislocations [3]. In contrast, fractures of the femoral neck are more common in older patients [4], unless there is a concomitant systemic disease in younger patients [5]. Traumatic hip dislocation can be divided into posterior, anterior, and inferior types. Posterior accounting for 85–90% of cases, anterior comprising 10–15%, and inferior comprising 2–5%. Obturator (inferior) type traumatic anterior hip dislocation in adult is rare of all types of hip dislocation. In the present case, reported to the hospital plane radiograph revealed obturator type of anterior right hip dislocation; on the basis of limb presentation and radiological findings, closed reduction was carried out under low duration general anesthesia and followed up after 6 weeks.
Case Report
We reported the case of a 75-year-old male who was brought to emergency room with a history of fall from the bicycle hit by a motorcyclist from back. After examined clinically and radiologically, the patient was diagnosed with obturator type of anterior right hip dislocation. Clinically, the patient was found to have apparent limb lengthening and hip flexion and external rotation. Plane radiographic examination (Fig.1) revealed the right anterior hip dislocation on the basis of these findings closed reduction under short general anesthesia was planned within 8 h.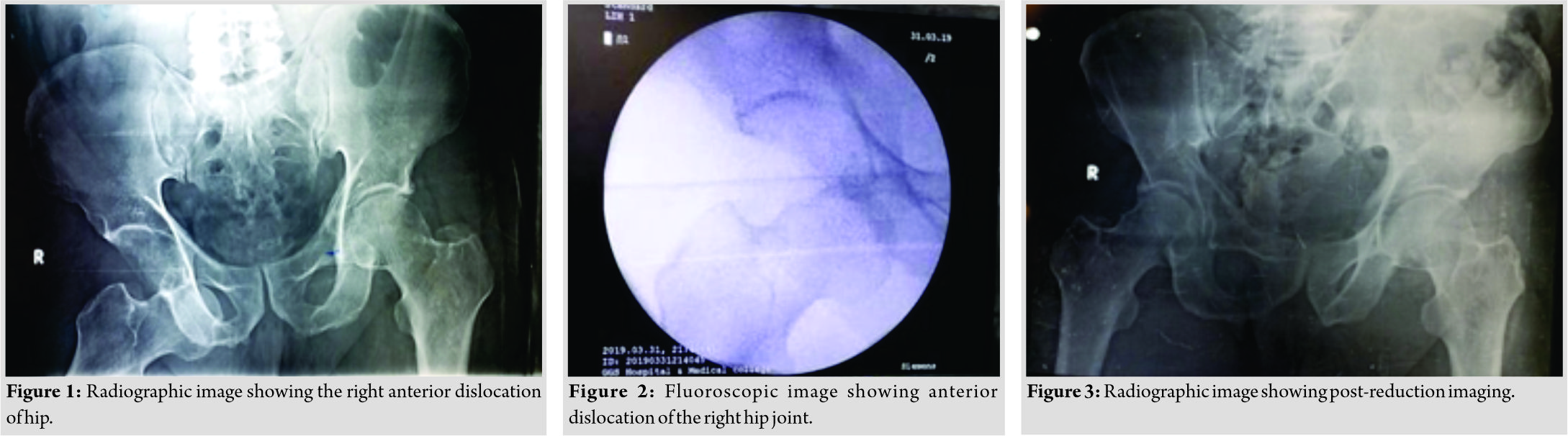
In the operation theater, the patient was put in a supine position under the effect of anesthesia and muscle relaxant. The pelvis was fixed by an orthopedic surgeon and applied a lateral traction force to inside of the thigh while another surgeon performed a longitudinal axial traction of the right leg and hip is slightly flexed till the femoral head was relocated into the acetabulum, which was checked by fluoroscopy (Fig. 2); it is referred to as Allis maneuver. At that moment, the hip was flexed and internally rotated and the fluoroscopic examination showed accurately relocated hip. Following reduction, the patient was transferred to orthopedic ward with limb in abduction and was examined carefully for any neurovascular injuries. X-ray taken 1 day after the reduction revealed a congruent right hip and no fracture signs (Fig. 3). The patient had an uneventful post-operative course and was immobilized for 3 weeks with progressive weight-bearing for 6 weeks. At 6–8 months follow-up, the patient is out of any complaints with a full range of motion of the right hip. X-ray in two planes shows a congruent right hip without signs of AVN or osteoarthritis and the patient is still under follow-up and advised follow-up after every 6months to rule out AVN/ osteoarthritis.
Discussion
The posterior dislocation of the hip is by far the most common type with a reported ratio of anterior to posterior dislocations ranging from 1:10 to 1:19 [3, 6]. Traumatic anterior dislocations, which account for 10–15% of all hip dislocations, are rarely reported in literature. After extensive research of literature, it has been found a paucity of data availability in context to anteroinferior dislocation of hip. An inferior hip dislocation is a rare type of hip dislocation that is not widely reported in literature. Only 12 cases are reported in British literature [7]. Anterior hip dislocation occurs when the knee strikes a dashboard with the thigh abducted or due to fall from a considerable height or from a blow to the back while in a squatting position [3, 6]. Anterior dislocations are of two main types depending on the amount of hip flexion at the time of impact: Superior, where the femoral head is displaced into the iliac or pubic region and inferior, where the femoral head lies in the obturator region. Out of these anteroinferior type is one of the rare presentations that have been reported here. Anterior hip dislocations can be associated with femoral neurovascular injury [8], femoral head fractures [9], and acetabular fractures. The initial treatment for a patient with hip dislocation is gentle and prompt reduction within 6 h and preferably under general anesthesia to prevent and minimize complications [10]. Appropriate management includes prompt reduction of any hip dislocation is imperative. According to literature, methods used for anterior hip dislocation reduction include closed and open methods of reduction. Closed methods for reduction of an anteriorly dislocated hip include various maneuvers which are Allis maneuver, Captain Morgan technique, reverse Bigelow’s technique, and Stimson maneuver. Multiple attempts may result in failure and prompt open reduction. Indications for open reduction include a non-concentric reduction (indicating a retained loose body or significant soft tissue injury preventing proper reduction), associated acetabular or femoral head fracture that will require an open repair, femoral neck fracture, and adislocation that is not reducible by closed reduction techniques [11]. An important complication following traumatic dislocation of the hip is prolonged and irreversible ischemia of the head of the femur, leading to osteonecrosis in 10–30% or more of cases, particularly if the dislocation is accompanied by severe bone destruction. Rapid identification and reduction arecritical, as prolonged dislocation increases the risk of developing AVN of the femoral head, and post-traumatic osteoarthritis is a common complication, even in the absence of associated fractures. Traumatic hip injuries have high morbidity and mortality rates due to multiple organ damage, primarily of the extremities, chest, and abdomen [12, 13, 14]. In another study conducted by Beebe et al. stated that osteoarthritis, osteonecrosis, heterotopic ossification, and sciatic nerve palsy could be the complications [15]. In our case luckily, the situation was not life threatening; in otherwise, it could lead to additional vital organ injuries sustained in the severe high-energy trauma. Identification and timely management of hip dislocation are highly dependent on imaging, both at presentation and after attempted reduction. It is imperative for the radiologist to understand imaging features that guide the management of hip dislocation to ensure timely identification, characterization, and communication of clinically relevant results. Accordingly, evaluation of hip dislocation requires not only radiographic detection of subtle findings of dislocation and urgent communication to the treating physician but also the inference of potential associated secondary osseous and softtissue injuries that could place the patient at risk for early osteoarthritis [16].
Conclusion
Anteroinferior type of hip dislocations isvery rarely seen injuries with severe high-energy trauma and also paucity of data availability in context to this rare presentation makes reporting such a case necessary to know the risks and benefits involved. Concomitant extremity fractures with additional vital organ injuries may lead to a life-threatening condition. The reduction must be done as soon as possible because it involves the functional prognosis of the hip by the risk of necrosis of the femoral head and subsequent osteoarthritis requiring long-term monitoring.
Clinical Message
Traumatic anterior hip dislocations are all around once in a while observed high-energy trauma. A detailed evaluation of emergency presentation, a multidisciplinary approach, and early assessment with the quick use of imaging modalities could be lifesaving for such patients.
References
1. Brooks RA, Ribbans WJ. Diagnosis and imaging studies of traumatic hip dislocations in the adult. Clin OrthopRelat Res 2000;377:15-23.
2. Calisir C, Fishman EK, Carrino JA, Fayad LM. Fracture-dislocation of the hip: What does volumetric computed tomography add to detection, characterization, and planning treatment? J Comput Assist Tomogr2010;34:615-20.
3. Sahin V, Karakaş ES, Aksu S, Atlihan D, Turk CY, Halici M. Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-9.
4. Barnes R, Brown JT, Garden RS, Nicoll EA. Subcapital fractures of the femur: A prospective review. J Bone Joint Surg Br 1976;58:2-24.
5. Swiontkowski MF, Winquist RA, Hansen ST Jr. Fractures of the femoral neck in patients between the ages of twelve and forty-nine years. J Bone Joint Surg Am 1984;66:837-46.
6. Amihood S. Anterior dislocation of the hip. Injury 1975;7:107-10.
7. Ismael S, Vora J, Thomas P. Adult traumatic inferior hip dislocation: Rare case ended with open reduction. J Orthop Case Rep 2017;7:101-4.
8. Schwartz DL, Haller JA Jr. Open anterior hip dislocation with femoral vessel transection in a child. J Trauma 1974;14:1054-9.
9. Jacob JR, Rao JP, Ciccarelli C. Traumatic dislocation and fracture dislocation of the hip. A long term follow-up study. Clin OrthopRelat Res 1987;214:249-63.
10. Hani R, Kharmaz M, Berrada MS. Traumatic obturator dislocation of the hip joint: A case report and review of the literature. Pan Afr Med J 2015;21:55.
11. Graber M, Johnson DE. Anterior Hip (Femur) Dislocation. Treasure Island, Florida: StatPearls Publishing;2019.
12. Dreinhofer KE, Schwarzkopf SR, Haas NP, Tscherne H. Isolated traumatic dislocation of the hip. Long-term results in 50 patients. J Bone Joint Surg Br 1994;76:6-12.
13. Lamberti PM, Rabin SI. Open anterior-inferior hip dislocation. J Orthop Trauma 2003;17:65-6.
14. Maruoka A, Naka N, Saito M, Toma Y. Pubic-type dislocation of the hip combined with fracture of the ipsilateral greater trochanter. A case report. Arch Orthop Trauma Surg 1993;112:299-301.
15. Beebe MJ, Bauer JM, Mir HR. Treatment of hip dislocations and associated injuries: Current state of care. Orthop Clin North Am 2016;47:527-49.
16. Mandell JC, Marshall RA, Weaver MJ, Harris MB, Sodickson AD, Khurana B. Traumatic hip dislocation: What the orthopedic surgeon wants to know. Radiographics2017;37:2181-201.
 |
 |
 |
 |
| Dr. Jagdeep Singh | Dr. Sorabh Garg | Dr. Sorabh Garg | Dr. Kapil Bansal |
| How to Cite This Article: Singh J, Garg S, Dahuja A, Bansal K. Traumatic Anterior Hip Dislocation in Elderly Male: An Atypical Case Report. Journal of Orthopaedic Case Reports 2020 Jan-Feb;10(1): 62-65. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


