
[box type=”bio”] Learning Point of the Article: [/box]
Most cases of gout can be successfully managed using medical therapy, surgical excision of tophi is acceptable in some cases and can promote wound healing and pain relief.
Case Report | Volume 10 | Issue 1 | JOCR January – February 2020 | Page 66-69 | Siddhartha Sinha, Raju Rijal, Jitendra Shah, Pashupati Chaudhary. DOI: 10.13107/jocr.2020.v10.i01.1640
Authors: Siddhartha Sinha[1], Raju Rijal[2], Jitendra Shah[2], Pashupati Chaudhary[2]
[1]Department of Orthopedics, Lady Hardinge Medical College, New Delhi, India,
[2]Department of Orthopaedics, B.P. Koirala Institute of Health Sciences, Dharan, Nepal,
Address of Correspondence:
Dr. Siddhartha Sinha,
Department of Orthopedics, Lady Hardinge Medical College, New Delhi, India.
E-mail: siddharthasinha87@gmail.com
Abstract
Introduction: Gout is a disease of deposition of monosodium urate crystal in the body which commonly presents as an acute arthritis of the peripheral joints but can have varied presentation. It is mostly managed by dietary modifications and drugs, but surgery is rarely required for the management of urate crystals.
Case Report: We present a case of a 66-year-old male who intermittently presented to the outpatient with multiple tophi which was managed with lifestyle changes and medically; initially, the patient eventually required surgical excision for tophi in fingers and heel which improved the pain and morbidity of the patient.
Conclusion: Gout can be managed by lifestyle changes, medically by drugs, and in extreme cases surgically and requires the utmost compliance by the patient. Such surgical intervention is rare with the advent of uricosuric medication now.
Keywords: Gout, surgical management of gout, hyperuricemia, tophi, urate.
Introduction
Hyperuricemia defined as uric acid of greater than 6.8mg/dL is relatively common in the human population with many regional variations [1]. Most patients have asymptomatic hyperuricemia but when the concentration of uric acid exceeds the body threshold monosodium urate crystals precipitate in the cooler areas of the body leading to gout [1]. The presentation of gout varies from an acute arthritis manifested as severe pain and inflammation around the affected joint called podagra to a chronic erosive arthritis which is characterized by joint erosion, deposition of uric acid crystals in the joint called tophi. Classically, the pain begins in the great toe, especially in the morning following a night of binge drinking or eating meat. Most patients are successfully managed by medication and lifestyle changes, surgical intervention although rare is also useful facet to the management of patients with advanced uncontrolled disease.
Case Report
The patient, a 66-year-old male, who had a long-standing history of gout under medications presented to the outpatient department with complaints of a mass on his left heel which became painful and ruptured 2 days earlier causing pain, swelling, and some bleeding. He had a history of painful masses over the multiple areas of hands, feet, elbows, and knees which progressed in size over the past 16 years. On presentation, the patient was not able to carry out the basic activities of daily living due to severe deformities of the hands and feet including holding a spoon or hairbrush due to tophi (Fig. 1).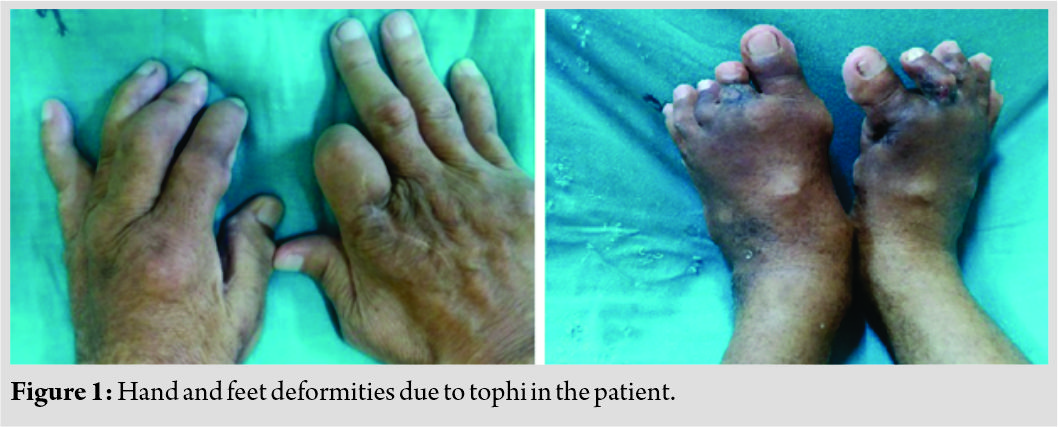
His medical history revealed that the patient had initially developed non-specific pain around the right ankle 16 years ago which was mild, dull without radiation, shifting and he was able to carry out his daily activities without discomfort which were treated with medications at a local practitioner. He has had similar episodic pains over the past 16 years. In October 2012, he developed tophi over the base of the right thumb which got infected and also led to acute kidney injury which was managed with three rounds of hemodialysis along with daily dressing of the wound with betadine and normal saline for lack of availability of better options. After this episode, allopurinol was prescribed. He underwent tophi excision in the left index finger (Fig. 2), olecranon, and right toe in July 2014. He has not required dialysis since.
The patient had a history of hypertension for the past 16 years who was prescribed amlodipine. On presentation, blood pressure was within normal limits. He consumed a non-vegetarian diet and reports a regular intake of alcohol. He was prescribed febuxostat to control his hyperuricemia. His father and two siblings had similar pains and swelling around the joints, for which they were taking medications.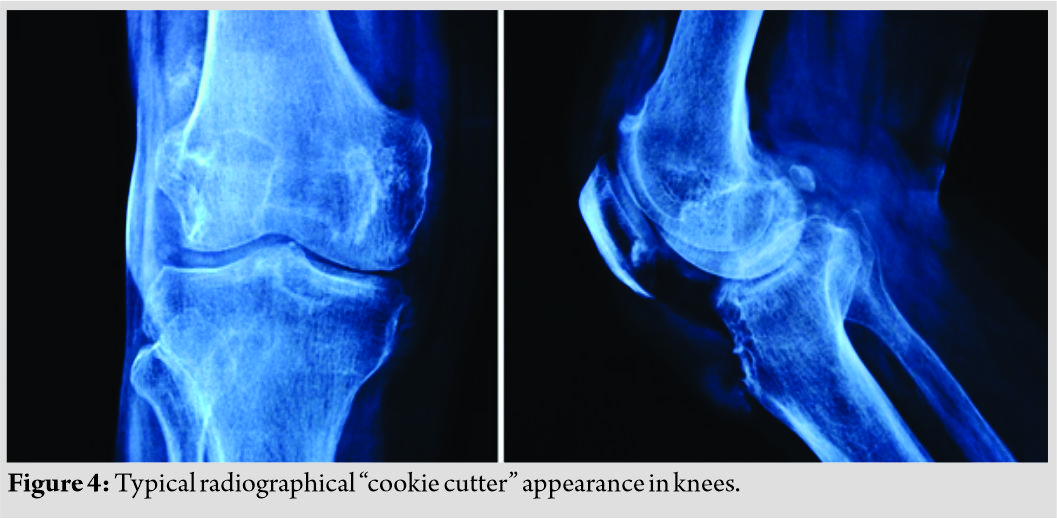
On physical examination, flexion deformities of the metacarpophalangeal joints (Fig. 1), and proximal and distal interphalangeal joints of all fingers and toes were noted along with tophi. Active and passive range of motion was painful and restricted in hands and toes. Local temperature was not raised. Ulcerated tophi seen on the heel of the left foot. Tophi also noted on the helix of both ears (Fig. 3), elbows, and heel.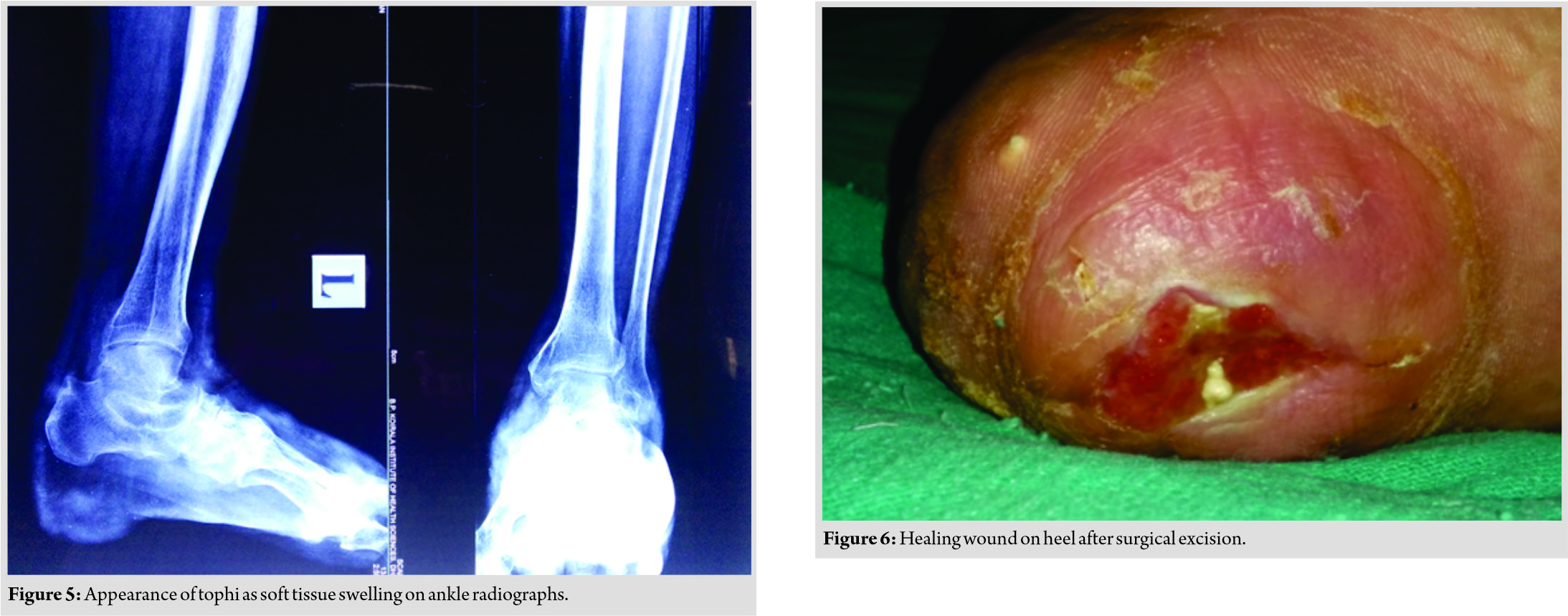
Laboratory work-up revealed a total leukocyte count of 6400/mm3, serum uric acid of 10.4mg/dL, urea 56mg/dL, and creatinine of 1.7mg/dL. X-ray of hands showed evidence of asymmetrical joint narrowing and typical calcified tophi and bone erosions sclerosis and the “cookie cutter/rat bitten” appearance of bones (Fig. 4 and 5) [2]. A diagnosis of chronic tophaceous gout with ruptured tophi was made and the patient underwent wound debridement for the heel tophus. Incision was made over the site of swelling, skin subcutaneous tissue resected, and the tophus excised and dressing done. Febuxostat was continued and dressing was done till the wound healed (Fig. 6).
Discussion
With the patient in focus for the discussion, we observed from the patients past and current records that the patient presented to us in October 2012, November 2012, July 2014, November 2014, and then May 2016. In all his follow-ups, he had a uric acid level of more than 6.0 which is associated with decreased risk of recurrence and tophi [3] (Graph 1). Comparing the X-rays of the patient over the years, it is obvious on how the progression of disease had affected his joint and functioning (Fig. 7). Gout is a preventable disease which can be a financial personal and social load on the patient as well as their attendants. While a majority of population has hyperuricemia, only a percentage has gout.
Old age, male sex, postmenopausal women, and patients undergoing some forms of chemotherapy are at higher risk of developing gout, as well as those who consumed meat, seafood, and alcohol. Low-fat dairy products, ascorbic acid, and wine consumption appeared to be protective for the development of gout [4, 5]. Commonly, gout can present as an acute arthritis commonly of the first metatarsophalangeal joint or as chronic tophaceous gout when the disease has been present for a long duration with poor control as seen in this patient. Overtime, uncontrolled gout can lead to polyarticular attacks and tophi deposition in soft tissues and joints [6]. Common locations of tophi include helix of the ears, fingers, toes, wrists, knees, and olecranon bursa, Tophi have been rarely reported on the sclerae, sub conjunctivally [7], and cardiac valves [8]. They have also been implicated in fractures [9], tendon and ligament ruptures, carpal tunnel syndrome and nerve compression symptoms[10]. Cooler temperatures on the periphery of the body and the serum concentration being near to the saturation level all aid in the formation and deposition of crystals in the typical sites. In any case of acute arthritis, the joint must be aspirated and the fluid sent for microscopy, biochemistry, and cultures. Fluid aspirated from a joint in an acute exacerbation of gout typically shows negatively birefringent needle-shaped monosodium urate crystals [4] which can differentiate it from calcium pyrophosphate crystals which are rhomboid and positively birefringent. Joint biochemistry can also indicate if any infective pathology is present as evidenced by a grossly purulent aspirate and decreased glucose and increased proteins. This holds especially true for large joints. Other tests to be sent include a complete blood count, serum uric acid, and plain radiography. Treatment for gout has four aspects: (a) Treating the acute attack, (b) prophylaxis for acute flares, (c) lowering the excess urate stores, and (d) surgical treatments for ruptured tophi, deformities, joint destruction and pain [1, 10]. Acute attacks are commonly treated using various combinations of nonsteroidal anti-inflammatory drugs, colchicine, oral, and/or topical steroids. Newer treatments include corticotropin, interleukin (IL)-1 antagonists (anakinra), human recombinant IL-1 receptor antagonist, and monoclonal antibody against IL-1β (canakinumab) [4]. While these treatments are giving promising results in refractory cases, most of these are out of reach for most patients due to cost and supply restrictions in most developing countries. Common pitfalls are initiating uric acid-lowering therapy during an acute phase. This can cause sudden changes in uric acid levels, leading to increase the severity and duration of symptoms rather than alleviating them. Avoiding aspirin as an analgesic is also wise since it competes with uric acid for excretion in the renal tubules. The goal of uricosuric treatment is to maintain serum uric acid levels below 6mg/dL which has been shown to decrease acute attacks and tophi formation [3]. Allopurinol and febuxostat are competitive and non-competitive inhibitors of the enzyme xanthine oxidase. Probenecid inhibits renal absorption of urate. Uricases (rasburicase and pegloticase) are new drugs which catalyze the oxidation of uric acid to allantoin which is soluble and is excreted easily. They are associated with anaphylaxis and infusion reactions [1]. Lenisurad is a selective uric acid reabsorption inhibitor which inhibits the urate transporter 1(-1) [1]. The efficacy and safety of these new drugs is still under investigation but their applications appear promising.
Surgical treatment is rarely indicated and reserved for those patients with sepsis or infection of ulcerated tophi as well as joint deformities, pain, and destruction of affected joints. The surgical options vary from a simple enucleation to amputation of the limb in case of infected ulcerations not amenable to treatment [10].
Conclusion
Gout is a preventable disease which can be a financial personal and social load on the patient as well as their attendants. The disease had rendered this patient near non-functional and he had to undergo enucleation and excision procedures which are now considered rare. Educating the patient about the disease, lifestyle changes, progression, addressing any cultural misconceptions, importance of follow-up, as well as a psychological evaluation can decrease morbidity as well as the need to see such advanced presentations of a treatable disease.
Clinical Message
Many patients in the general population have asymptomatic hyperuricemia which may not need treatment. With the onset of clinical symptoms, gout can be managed with medications alone in a majority of cases. Simple surgical excision of the tophi is an acceptable management to bring about rapid relief and promote healing of the wound.
References
1. Rothschild BM, Miller A, Francis M. Gout and Pseudogout. Website Medscape; 2014.
2. Talbott JH, Altman RD, editors. Gouty Arthritis Masquerading as Rheumatoid Arthritis or Vice Versa. Seminars in Arthritis and Rheumatism. New York: Elsevier; 1978.
3. LeeSJ, TerkeltaubRA, KavanaughA. Recent developments in diet and gout.CurrOpinRheumatol2006;18:193-8.
4. Roddy E, Doherty M. Gout epidemiology of gout. Arthritis Res Ther2010;12:223.
5. SarmaP, DasD, DekaP, DekaAC. Subconjunctival urate crystals: A case report.Cornea2010;29:830-2.
6. PatelGK, DaviesWL, PricePP, HardingKG. Ulcerated tophaceous gout.Int Wound J2010;7:423-7.
7. NguyenC, EaHK, PalazzoE, LiotéF. Tophaceous gout: An unusual cause of multiple fractures.Scand J Rheumatol2010;39:93-6.
8. TranA, PrenticeD, ChanM. Tophaceous gout of the odontoid process causing glossopharyngeal, vagus, and hypoglossal nerve palsies.Int J Rheum Dis2011;14:105-8.
9. SonneveldP, vanBekkum DW. The effect of whole-body irradiation on skeletal growth in rhesus monkeys.Radiology1979;130:789-91.
10. KumarS, GowP. A survey of indications, results and complications of surgery for tophaceous gout.N Z Med J2002;115:U109.
 |
 |
 |
 |
| Dr. Siddhartha Sinha | Dr. Raju Rijal | Dr. Jitendra Shah | Dr. Pashupati Chaudhary |
| How to Cite This Article: Sinha S, Rijal R, Shah J, Chaudhary P. A Case of Surgically Intervened Chronic Tophaceous Gout and Review of Literature. Journal of Orthopaedic Case Reports 2020 Jan-Feb;10(1): 66-69. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


