
[box type=”bio”] Learning Point of the Article: [/box]
This case highlights the importance of having a high index of suspicion to detect non-union after tibial spine fracture as long as timely treatment may be crucial to avoid definite sequels and disabilities.
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 27-31 | Marco Bernardes, Guido Duarte. DOI: 10.13107/jocr.2020.v10.i03.1734
Authors: Marco Bernardes[1], Guido Duarte[1]
[1]Department of Orthopaedics, Orthopaedics and Traumatology Service, Centro Hospitalar de Vila Nova de Gaia/Espinho, Gaia, Portugal.
Address of Correspondence:
Dr. Marco Bernardes,
Department of Orthopaedics, Orthopaedics and Traumatology Service, Centro Hospitalar de Vila Nova de Gaia/Espinho, Gaia, Portugal.
E-mail: marco.silva.bernardes@gmail.com
Abstract
Introduction: Fractures of the tibial spines occur in 3/100,000 children per year and are rare in children under 8 years. Non-union after avulsion fracture of the tibial spine is even rarer, especially under 8 years, with only few cases described in the literature.
Case Presentation: A 6-year-old boy with went to the emergency department after suffering trauma in his left knee. In the performed X-ray, no osteoarticular injury was identified. Conservative treatment with immobilization with cast was performed. After removing the immobilization, the initial evolution was positive with no pain on mobilization. A few months later, he went again to the emergency department due to new left knee trauma. On examination, he had pain in the mobilization of the left knee, especially in knee extension which was not entire. Image study led to the diagnostic of avulsion fracture of the anterior tibial spines. The fracture was classified as modified Meyers and Mckeever Type II and conservative treatment with cast immobilization was performed. In the clinical and imaging revaluation done 4 weeks later, an evolution to non-union of the anterior tibial spine was noticed. At arthroscopy, non-union of tibial spines was confirmed, with elephant paw bone fragment with loss of its right to domicile. Open surgery was performed with debridement, cruentation, and fixation of the bone fragment to the tibia with a screw. The patient had favorable post-operative evolution with fracture consolidation, preserved mobility, no instability of the joint, and no limitation in daily and school activities. Four years after the initial surgery, a second procedure was performed for the removal of the screw. During 7 years of follow-up, no limitations or sequels were found.
Conclusion: This case illustrates a very rare complication of the fracture of the tibial spine, the non-union, which is very rare under 8 years age. Besides, it highlights the importance of having a high index of suspicion to detect non-union after tibial spine fracture as long as timely treatment may be crucial to avoid definite sequels and disabilities.
Keywords: Non-union, avulsion fracture of the tibial spines, osteosynthesis.
Introduction
Fractures of the tibial spines occur in 3/100,000 children per year and are rare in children under 8 years most commonly affecting the immature skeletal systems of children between 8 and 14 years old [1]. Usually, they are classified based on the X-ray results according to the most used classification, the modified Meyers and Mckeever classification, a system that includes four types [2]: Type I is non-displaced or minimally displaced fractures involving the anterior margin of the spine; Type II has superior displacement of the anterior bony fragment with an intact posterior cortical hinge; Type III is completely displaced but not rotated; and Type IIIþ is completely displaced with rotation. Zaricznyj described a fourth type of fracture, which includes complete displacement and comminution. The purpose of the treatment of these fractures is to achieve an almost anatomic reduction to restore anterior cruciate ligament (ACL) tension. Non-union after avulsion fracture of the tibial spine is even rarer, especially under 8 years, with only few cases described in the literature [3, 4, 5, 6, 7, 8, 9].
Case Presentation
A Caucasian 6-year-old boy with no relevant medical history went to the emergency department after suffering trauma in his left knee after fell off his bicycle. He complained of pain in the left knee and clinical examination showed functional disability of the joint and hematic joint effusion. In the performed X-ray (Fig. 1), no osteoarticular injury was diagnosed and a pattern of massive joint effusion was found. Arthrocentesis with drainage of hematic fluid was performed and the joint was immobilized with cast for conservative treatment. After removing the immobilization, the initial evolution was positive with no pain on mobilization or joint effusion.
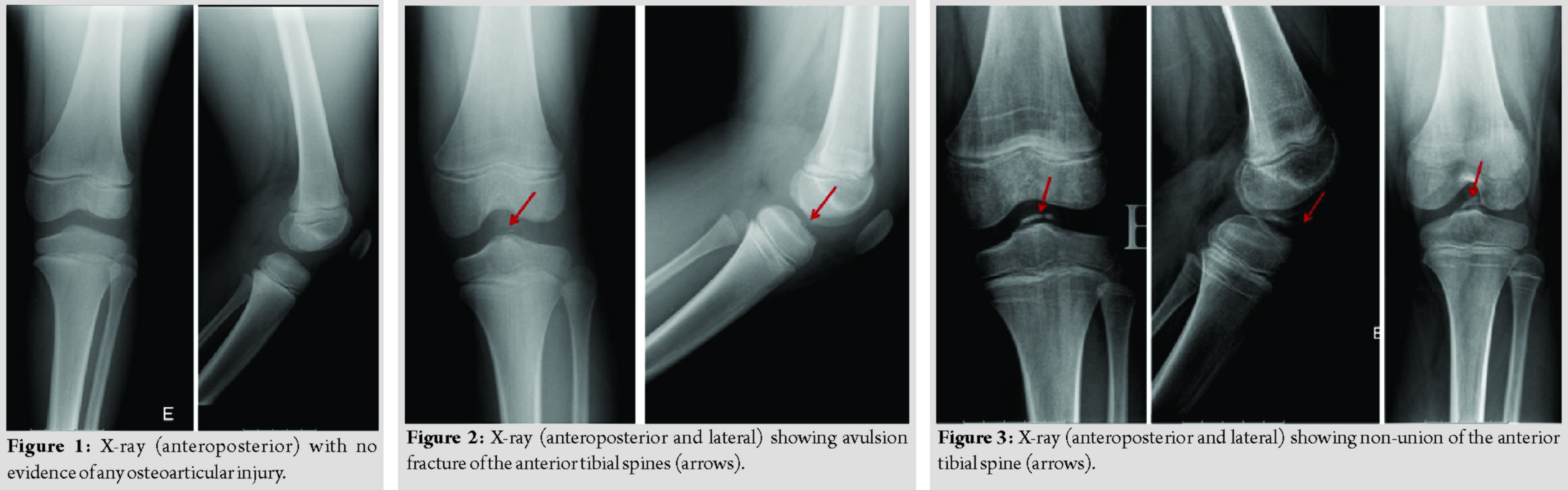
A few months later, he went again to the emergency department due to new left knee trauma after pivot-type rotation and worsening of the pain. He admitted that symptoms had become persistent after the first knee trauma and he had complained of pain and some limitation on knee extension. On examination, he had pain in the mobilization of the left Knee, especially in knee extension which was not entire. The performed X-ray revealed avulsion fracture of the anterior tibial spines (Fig. 2). The fracture was classified as modified Meyers and Mckeever Type II. Taking into account, the age of the patient and the apparent positioning of the bone fragment in relation to the bed led to the decision of conservative treatment with cast immobilization with weekly follow-up and serial imaging control. In X-ray performed (Fig. 3) 6 weeks later, an evolution to non-union of the anterior tibial spine was noticed. Besides, joint instability was detected by Lachman test and pivot shift test. The magnetic resonance imaging (MRI) of the knee (Fig. 4) confirmed the non-union of the avulsion fracture and excluded lesion of the ACL or the meniscus. A surgical treatment with reinsertion of the tibial spines was decided. At arthroscopy, non-union of tibial spines was confirmed, with elephant paw bone fragment with loss of its right to domicile. Based on these findings, conversion to open surgery was chosen for bed reshaping and anatomical reinsertion of the bone fragment in view of adequate ACL tension. The patient was prepared to open reduction. A paramedian arthrotomy was performed. The fracture was identified and debridement, cruentation, and fixation of the bone fragment to the tibia with a 3 cm screw were done (Fig. 5). The patient had favorable post-operative evolution with fracture consolidation seen on X-ray (Fig. 6), preserved mobility (symmetrical to contralateral), no instability of the joint, and no limitation in daily and school activities. Four years after the initial surgery, a second procedure was performed for the removal of the screw (Fig. 7). Although the screw had penetrated the physis (Fig. 7), there was no repercussion in the growth of the affected limb as can be seen in the serial extra long X-ray performed on follow-up (Fig. 8). Besides, the MRI of knee performed 6 years after the surgery showed consolidation of the fracture and integrity of the anterior crucial ligament (Fig. 9).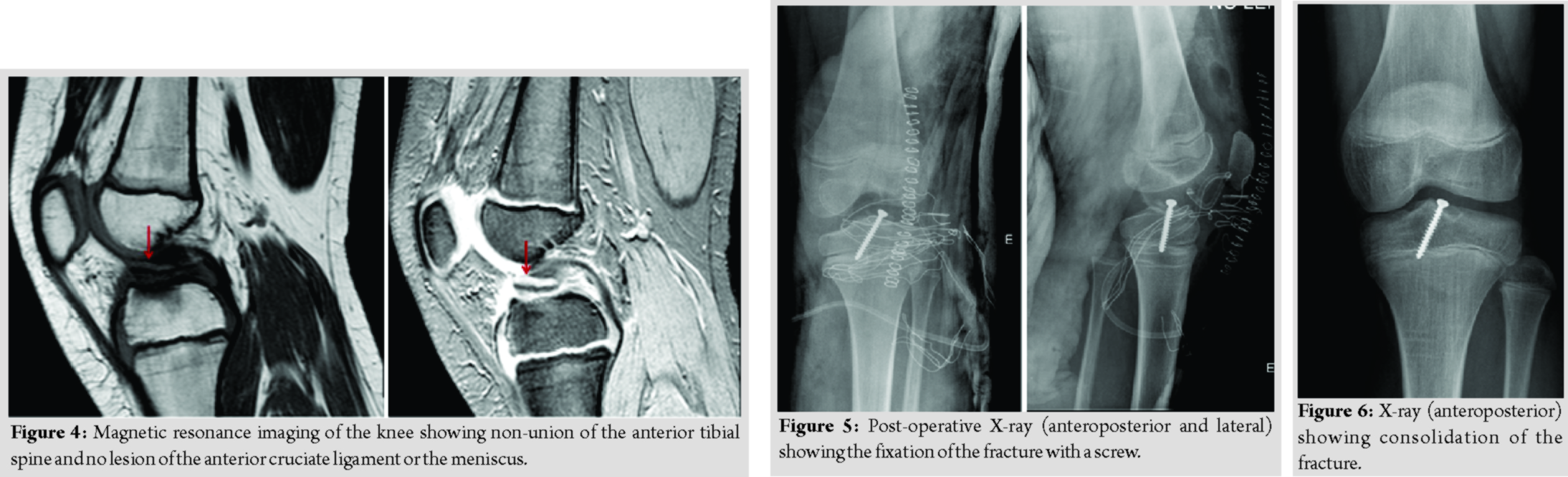
Discussion
This case illustrates a non-union after avulsion fracture of the anterior tibial spine in a 6-year-old child treated initially with conservative treatment and then with surgical treatment. According to the literature, this case has some peculiarities: At first, the fracture of the tibial spine is rare in children under 8 year’s old [1]. In fact, most of these fractures occur in children between 8 and 14 years [1]. Moreover, the non-union after avulsion fracture of the tibial spines is even rarer, with only few cases described in the literature [3, 4, 5, 6, 7, 8, 9]. At the best of our knowledge, this is the second case described in a so young child [3, 4, 5, 6, 7, 8, 9]. There are some facts in the way, this case was managed that should be discussed. At first, if present, the avulsion fracture was not diagnosed in the first visit of this patient to the emergency department. At that time, the patient had suffered a trauma in the knee after fall of his bike, which is one of the most frequent activities that result in these fractures together with skiing and motor vehicle accidents [10]. Moreover, the patient complained of pain and had hematic effusion. All these facts together seemed to point that a fracture/lesion could be present and although the X-ray was normal, maybe the patient should have done another image examination like MRI to exclude the fracture or lesions of the soft tissue. In fact, nowadays, MRI is not only used to diagnose the avulsion fraction of tibial spines but also to classify them. In 2018, Green et al. appointed an MRI-based classification for avulsion fractures of tibial spine that provides quantitative rather than qualitative recommendations for classifying fractures based on fracture pattern, fragment displacement, and soft-tissue involvement [11]. Besides, Green et al. recommend that MRI should be routinely obtained for patients with avulsion fracture of tibial spines as the use of the MRI-based system reduces ambiguity in grading and has the potential to streamline decisions regarding treatment. Despite that, the first treatment of the patient of the present case was appropriate with immobilization with cast and revaluation in 4 weeks. In the revaluation visit, the patient had no acute symptoms and the X-ray done seemed to be normal, which supported the treatment option. After that visit, the patient missed medical follow-up for some months but complained of pain and some limitation on knee extension which raises suspicion of underlying lesion after the first trauma and highlights the importance of high suspicion index and close follow-up maintenance in these cases, especially when symptoms persist. Unfortunately, the patient was only reassessed in his second visit to the emergency department. At that time, he referred new trauma in the left knee, after pivot-type rotation. This movement could cause a new fracture but could also disclose or worsen a previous lesion occurred in the first trauma. As in this case, some of the few causes of non-union avulsion fractures of tibial spines described in the literature, have described more than one trauma in the knee before diagnosis [6]. After image study, a modified Meyers and Mckeever Type II avulsion fracture of the tibial spines was diagnosed. While the treatment is well established in Type I (non-displaced) and in Type III and IV (displaced) fractures, in Type II avulsion fractures of the tibial spines, the treatment is more controversial. Some authors defend that conservative treatment is the treatment of choice because it can led to good results without surgical aggression including its risk [12]. In this option, close monitoring is recommended. For other hand, other authors defend the surgical treatment in the first intention to achieve osseous union, restoration of knee stability, return to function, treatment of associated injuries, and restoration of the range of motion [13]. Besides, current evidence has demonstrated equivalent outcomes for open and arthroscopic reduction strategies, as well as for screw-based and suture-based fixation techniques [14]. In the case presented, when Type II avulsion fracture of the tibial spines was diagnosed without involvement of the ACL or the meniscus, the first choice was conservative treatment. However, in the follow-up, non-union of the tibial spine was diagnosed and surgical fixation of the bone fragment with screw was needed. The few data available in the literature seem to indicate that non-union most frequently results from non-treatment or conservative treatment of avulsion fracture of tibial spines, as occurred in the case presented, than with surgical treatment [6]. However, taking into account, the few cases reported the factors that may predispose to non-union such as individual factors, type of fracture, and treatments performed remain unclear. Recent data demonstrated the potential application of recombinant human bone morphogenetic protein-2 as adjuvant treatment of congenital pseudarthrosis of the tibia or persistent tibial non-union in children and adolescents [15]. The future of the treatment of the avulsion fracture of tibial spines may also include this kind of treatment to obtain better results.
Conclusion
This case is an original case report of interest to orthopedics, traumatologists, and pediatricians. It illustrates a non-union after an avulsion fracture of the tibial spine, both of them very rare in a so young child. Besides, it highlights the importance of having a high index of suspicion of avulsion fracture of tibial spines as well as the recognition of non-union after tibial spine fracture, once timely treatment may be crucial to avoid definite sequels and disabilities. In general, a long follow-up is required and recommended to check the possible complications that can appear with the growth. The best treatment to Type II fractures is still to define.
Clinical Message
With this paper, the authors pretend to present two rare findings in a very young child, a non-union after an avulsion fracture of the tibial spine. Besides, the authors want to highlight the importance of having a high index of suspicion of avulsion fracture of tibial spines as well as the recognition of non-union after tibial spine fracture, once timely treatment may be crucial to avoid definite sequels and disabilities.
References
1. Shin YW, Uppstrom TJ, Haskel JD, Green DW. The tibial eminence fracture in skeletally immature patients. Curr Opin Pediatr 2015;27:50-7.
2. Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1959;41:209-22.
3. Meyerding HW, Walsh AC. Avulsion fracture with nonunion of the anterior tibial spine treated by fixation with beef-bone screw; report of a case. Surg Clin North Am 1949;29:1029-33.
4. Lugar EJ, Arbel R, Eichenblat MS, Menachem A, Dekel S. Femoral notchplasty in the treatment of malunited intercondylar eminence fractures of the tibia. Arthroscopy 1994;10:550-1.
5. Panni AS, Milano G, Tartarone M, Fabbriciani C. Arthroscopic treatment of malunited and nonunited avulsion fractures of the anterior tibial spine. Arthroscopy 1998;14:233-40.
6. Horibe S, Shi K, Mitsuoka T, Hamada M, Matsumoto N, Toritsuka Y. Nonunited avulsion fractures of the intercondylar eminence of the tibia. Arthroscopy 2000;16:757-62.
7. Kawate K, Fujisawa Y, Yajima H, Sugimoto K, Habata T, Takakura Y. Seventeen-year follow-up of a reattachment of a nonunited anterior tibial spine avulsion fracture. Arthroscopy 2005;21:760.
8. Ahn JH, Yoo JC. Clinical outcome of arthroscopic reduction and suture for displaced acute and chronic tibial spine fractures. Knee Surg Sports Traumatol Arthrosc 2005;13:116-21.
9. Vargas B, Lutz N, Dutoit M, Zambelli PY. Nonunion after fracture of the anterior tibial spine: Case report and review of the literature. J Pediatr Orthop B 2009;18:90-2.
10. Coyle C, Jagernauth S, Ramachandran M. Tibial eminence fractures in the paediatric population: A systematic review. J Child Orthop 2014;8:149-59.
11. Green D, Tuca M, Luderowski E, Gausden E, Goodbody C, Konin G. A new, MRI-based classification system for tibial spine fractures changes clinical treatment ecommendations when compared to Myers and Mckeever. Knee Surg Sports Traumatol Arthrosc 2018;27:86-92.
12. Gans I, Ganley TJ. Tibial eminence fractures: A review and algorithm for treatment. Univ PA Orthop J 2013;23:1-4.
13. Edmonds EW, Fornari ED, Dashe J, Roocroft JH, King MM, Pennock AT. Results of displaced pediatric tibial spine fractures: A comparison between open, arthroscopic, and closed management. J Pediatr Orthop 2015;35:651-6.
14. Tuca M, Bernal N, Luderowski E, Green DW. Tibial spine avulsion fractures: Treatment update. Curr Opin Pediatr 2019;31:103-11.
15. Hissnauer TN, Stiel N, Babin K, Rupprecht M, Hoffmann M, Rueger JM, et al. Bone morphogenetic protein-2 for the treatment of congenital pseudarthrosis of the tibia or persistent tibial nonunion in children and adolescents: A retrospective study with a minimum 2-year follow-up. J Mater Sci Mater Med 2017;28:60.
 |
 |
| Dr. Marco Bernardes | Dr. Guido Duarte |
| How to Cite This Article: Bernardes M, Duarte G. Non-union after Fracture of the Anterior Tibial Spine in a 6-Year-old Child: A Case Report. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 27-31. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


