
[box type=”bio”] Learning Point of the Article: [/box]
Meticulous surgery avoiding spillage of cyst material, appropriate medication as advised by the infectious disease specialist, long follow-up to ensure compliance with medication and to detect recurrence will give fruitful results in spinal hydatid cyst disease.
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 57-59 | Jeevan Kumar Sharma, Vikas Tandon, Nandan Marathe, Yogendra Agrahari, Abhinandan Reddy Mallepally, Harvinder Singh Chhabra. DOI: 10.13107/jocr.2020.v10.i03.1748
Authors: Jeevan Kumar Sharma[1], Vikas Tandon[1], Nandan Marathe[1], Yogendra Agrahari[1], Abhinandan Reddy Mallepally[1], Harvinder Singh Chhabra[1]
[1]Department of Spine Services, Indian Spinal Injuries Centre, Delhi, India.
Address of Correspondence:
Dr. Nandan Marathe,
Saraswati Prasad, Gaul Wada, Vasai, Palghar – 401201, Maharashtra, India.
E-mail: nandanmarathe88@gmail.com
Abstract
Introduction: Hydatid disease is caused by the parasite Echinococcus granulosus which is also known as the dog tapeworm. This disease is a relatively uncommon cause of spinal cord and dural compression.
Case Report: We came across a peculiar case in a 41-year-old male patient who presented to us with pus discharge from a surgical wound over lower back for 10 days. The patient was a diagnosed as a case of lumbar canal stenosis with recurrent hydatid cyst. The patient had neurological involvement in the form of left-sided foot drop. The patient gave a history of lumbar canal stenosis secondary to hydatid cyst, for which decompression and cyst excision were done 3 years prior. The patient was re-operated in the form of wound debridement with removal of hydatid cyst.
Conclusion: Meticulous surgery avoiding spillage of cyst material, appropriate medication as advised by the infectious disease specialist, will avoid recurrence of the disease.
Keywords: Lumbar spine, hydatid cyst, Echinococcus granulosus.
Introduction
Hydatid disease is caused by the parasite Echinococcus granulosus which is also known as the dog tapeworm [1]. This disease is usually associated with visceral involvement and skeletal involvement is uncommon. Vertebral body is the most common site for bony involvement among which thoracic vertebra is the commonest [2]. Isolated spinal hydatid disease without any visceral involvement is a rare entity [3]. Here, we present a case of isolated spinal hydatid cyst of the lumbar spine with neurological involvement.
Case Report
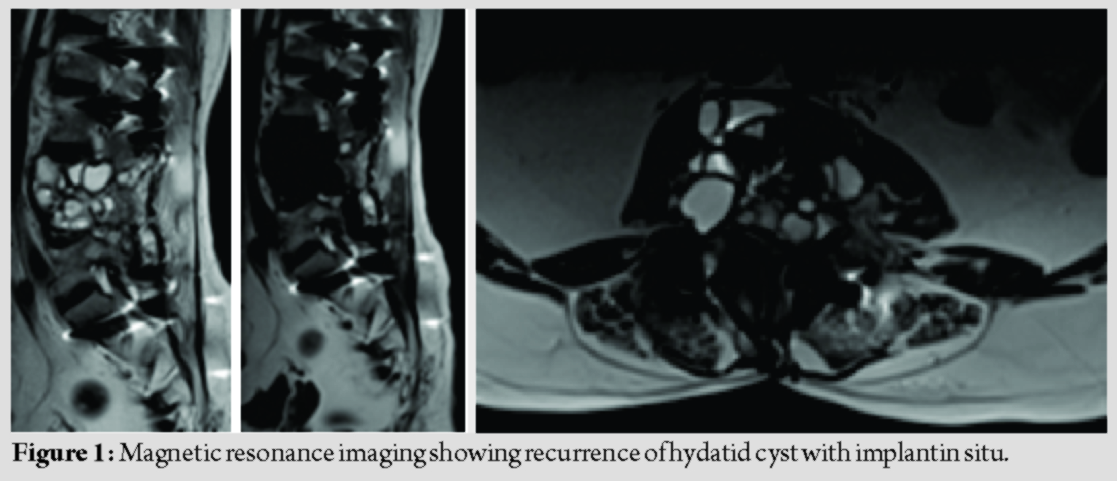
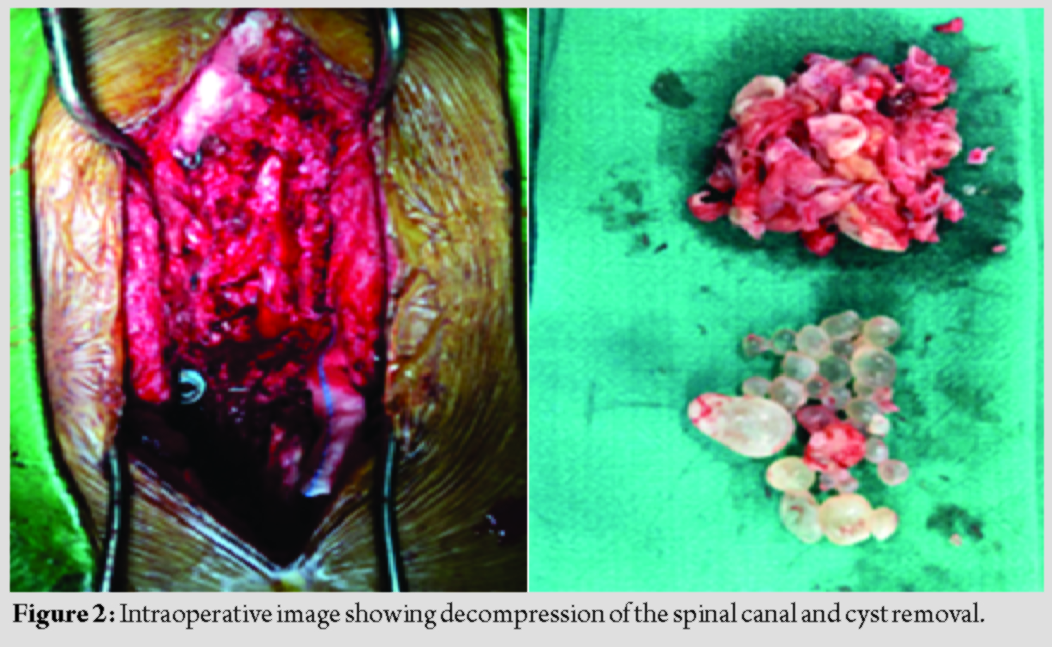
A 41-year-old male patient presented to our tertiary care spinecenter with complaints of pus discharge from the lower back for 10 days, persistent low back pain, and weakness of the left foot. He gave a history of the previous surgery 3 years ago for similar complaints, after which the patient was asymptomatic. On examination of the spine, the previous surgical scar with pus discharge, local tenderness, and warmth was noted. Neurological examination revealed Grade 0 Medical Research Council(MRC) power in the left ankle dorsiflexion and extensor hallucislongus (EHL). Sensations were reduced in the left L4-L5 and S1 dermatome. The straight leg raising test was positive on the left side at 40°. Radiological examination revealed a laminectomy defect at L4-L5 level on plain radiographs. Multiple intraspinal cystic lesions which were hyperintense on T2 and hypointense on T1 magnetic resonance imaging (MRI)were seen. Blood examination revealed raised lymphocytes, eosinophil, and C-reactive proteins. Ultrasonography of abdomen and chest X-ray which were done to look for visceral involvement were normal. Based on these investigations, a diagnosis of lumbar canal stenosis at L4-L5 level due to the recurrence of hydatid disease was made. The patient underwent wound debridement and decompression surgery (Fig. 1) with hydatid cyst removal (Fig. 2) through the previous incision.
We did a wide surgical exposure. We encountered scar tissue due to the previous surgery. The level of laminectomy was identified on fluoroscopy. Gentle handling of the cyst was done to avoid spillage. The most common cause of recurrence is intraoperative spillage; hence, this step is critical. Following the debridement, copious wound irrigation with hypertonic saline was done. The wound was closed in layers over a negative suction drain. Post-operative daily dressing with antibiotic treatment was given. Signs of wound healing were present at the time of discharge. He was continued on anti-helminthic treatment postoperatively as per the advice of the infectious disease specialist.
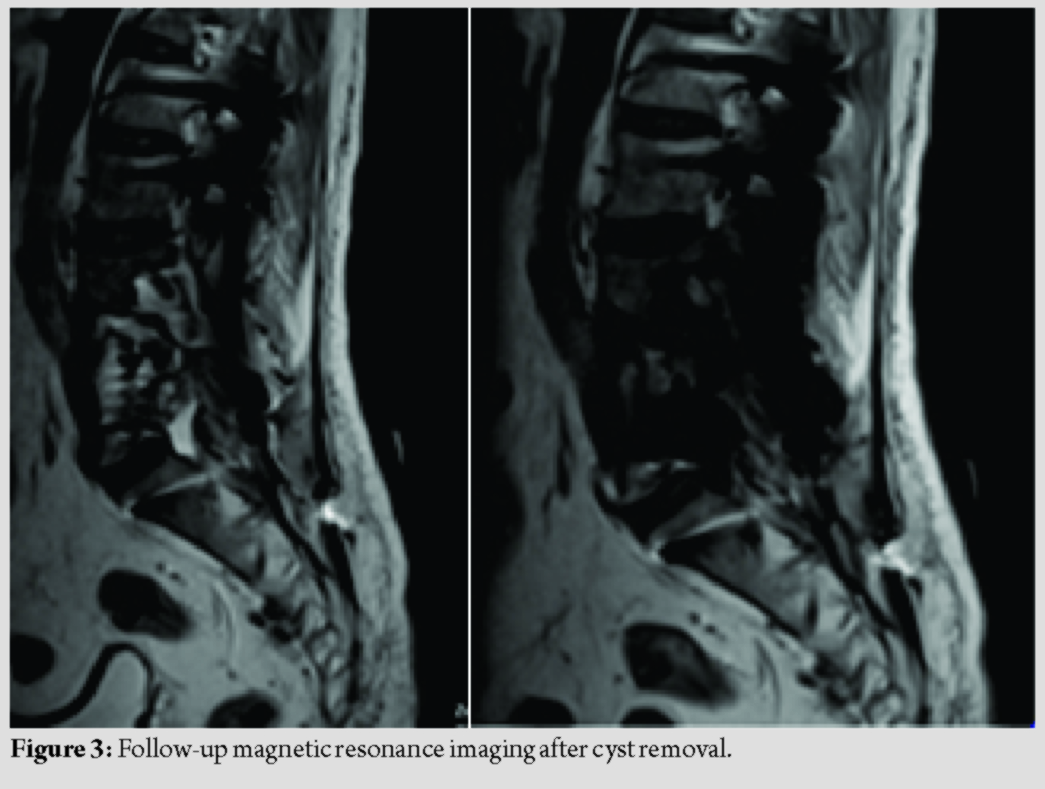
Patients neurology improved to Grade 3 (MRC) in the left ankle dorsiflexion and EHL. He is presently asymptomatic with a 3-year follow-up duration. Follow-upMRI did not reveal any recurrence of the lesion (Fig. 3).
Discussion
Hydatid disease is caused by the cestode E. granulosus. This disease is common in the Middle East region. The usual locations for this entity are the liver (60–70%) and lung (10–15%) [4]. Skeletal involvement is seen only in 0.5–2% of cases among which thoracic vertebra is the most common site. Vertebral involvement is generally associated with visceral involvement either in the lung or liver. Isolated vertebral involvement is uncommon. This can occur with direct portovertebral venous shunt [5]. In our case, the lumbar spine was involved with no visceral involvement. Braithwaite and Lees classified spinal hydatid cyst disease based on location into five types, namely, intramedullary, extramedullary intradural, extradural-intraspinal, vertebral, and paravertebral [6]. Spinal hydatid cyst disease does not manifest with any pathognomicsigns except those of direct compression on the cord [7]. Neurological involvement is seen in 20–80% of cases [8]. Our case was of the extradural intraspinal type. The aim of surgery in symptomatic cases of spinal hydatid cyst is to decompress the cord mainly with laminectomy and removal of the cyst. Care must be taken not to rupture any cyst to avoid recurrence [9]. However, cyst rupture is a common occurrence during surgical intervention. Thus, the hypertonic saline wash at the end of procedure, and post-operative anti-helminthic therapy for 6 months is recommended to prevent redevelopment of the cyst. Recurrence in spinal hydatid disease is 30–40% which is usually due to rupture of cyst intraoperatively [10]. Failure of surgical decompression and recurrence can also be due to a lack of diffusion of anthelminthic medication like albendazole into intradural space. In our case, the patient was operated 3 years ago for lumbar canal stenosis at L4-L5 level due to hydatid cyst, and anti-helminthic medication was given postoperatively. He came with a recurrence of symptoms due to relapse of spinal hydatid disease evident on investigation. Revision surgery in the form of debridement and removal of cysts was done.
Conclusion
Our case represents a rare variety of isolated spinal hydatid disease in the lumbar spine without visceral involvement leading to lumbar canal stenosis. Meticulous surgery avoiding spillage of cyst material, appropriate medication as advised by the infectious disease specialist, and long follow-up to ensure compliance with medication and to detect recurrence will give fruitful results in spinal hydatid cyst disease.
Clinical Message
Meticulous surgery avoiding spillage of cyst material, appropriate medication as advised by the infectious disease specialist, and long follow-up to ensure compliance with medication and to detect recurrence are needed for successful treatment of hydatid cyst of the spine.
References
Sharma JK, Tandon V, Marathe NA, Agrahari Y, Mallepally AR, Chhabra HS.Hydatid Cyst of the Spine: A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 57-59.
 |
 |
 |
 |
 |
| Dr. Jeevan Kumar Sharma | Dr. Vikas Tandon | Dr. Nandan Marathe | Dr. Yogendra Agrahari | Dr. Harvinder Singh Chhabra |
| How to Cite This Article: Sharma JK, Tandon V, Marathe NA, Agrahari Y, Mallepally AR, Chhabra HS.Hydatid Cyst of the Spine: A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 57-59. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


