
[box type=”bio”] Learning Point of the Article: [/box]
Diagnostic modality and presentation of myxoma
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 60-62 | Manjeet Singh, Subodh Kumar Pathak, Vishesh Verma, Praveen Thivari. DOI: 10.13107/jocr.2020.v10.i03.1750
Authors: Manjeet Singh[1], Subodh Kumar Pathak[1], Vishesh Verma[1], Praveen Thivari[1]
[1]Department of Orthopedics, MMIMSR, M M Deemed to be University, Mullana, Ambala, Haryana, India.
Address of Correspondence:
Dr. Subodh Kumar Pathak,
Department of Orthopaedics, MMIMSR, M M Deemed to be University,
E-mail: drsubodh08@gmail.com
Abstract
Introduction: Myxoid soft tissue tumors consist of a heterogeneous group of mesenchymal neoplasms with a hallmark of the abundant extracellular myxoid matrix. Intramuscular myxomas are rare benign tumor affecting the musculoskeletal system. The common sites include the thigh, upper arm, calf, and the buttocks. Magnetic resonance imaging is the radiological modality of choice in diagnosing these cases, while tissue biopsy is the gold standard.
Case Presentation: A 70-year-old male presented to orthopedics out-patient department with complaints of a humongous swelling engulfing his right thigh all around. The gradual and progressive appearance of burning sensations and rest pain around the affected area with difficulty in bearing weight, over the past 6–7 months forced him to seek medical attention. Biopsy and imaging were performed followed by final excision. The tumor was removed En-bloc and post-operative period was uneventful. The patient did not show any signs recurrence and was asymptomatic until the final followup of 26 months.
Conclusion: Myxomatous swelling mimics an intramuscular lipoma, sarcoma, hematoma, or a hemangioma and must be carefully evaluated. En-bloc excision without spillage is the treatment of choice which ensures long and lasting recovery.
Keywords: Benign, excision, giant, intramuscular myxoma, magnetic resonance imaging.
MeSH terms: Myxoma, Benign, Thigh, Excision
Introduction
Myxomas were first described by Stout in 1948. Soft tissue myxomas consist of a group of mesenchymal tumors that are characterized by the abundance of extracellular myxoid matrix [1]. Myxoid tissue comprises a gelatinous mucopolysaccharide matrix of sulfated and non-sulfated glycosaminoglycans [2]. Based on radiological and histopathological findings, benign myxomas are further divided into intramuscular myxoma, aggressive angiomyxoma, superficial angiomyxoma, myxolipoma, dermal myxoma, and acral fibromyxoma [2]. The slow growth of the lesion is an essential attribute. Myxomas are usually seen in the 4th–6th decades of life and can attain relatively large sizes, as seen in many soft tissue sarcomas, making it difficult to distinguish from them [3]. En masse excision is the definitive treatment modality and no adjuvant or neoadjuvant therapy has been advocated in the literature.
Case Report
The patient was a 70-year-old male who presented to the orthopedic outpatient clinic with a slowly progressive swelling around his right thigh over the past 10 years. The patient had observed the swelling grow to its present size which was relatively painless in the past, but painful for the past 6 months, thereby causing difficulty in his activities of daily living. The pain was present even at rest and radiated to the right leg. On clinical examination, there was a smooth, lobulated, painless, and firm swelling covering the back of the thigh extending anteriorly, medially as well as laterally. On the posterior surface, it was approximately 25 × 10 cm, with anterior lobulation approximately 15 × 5 cm (Fig. 1).
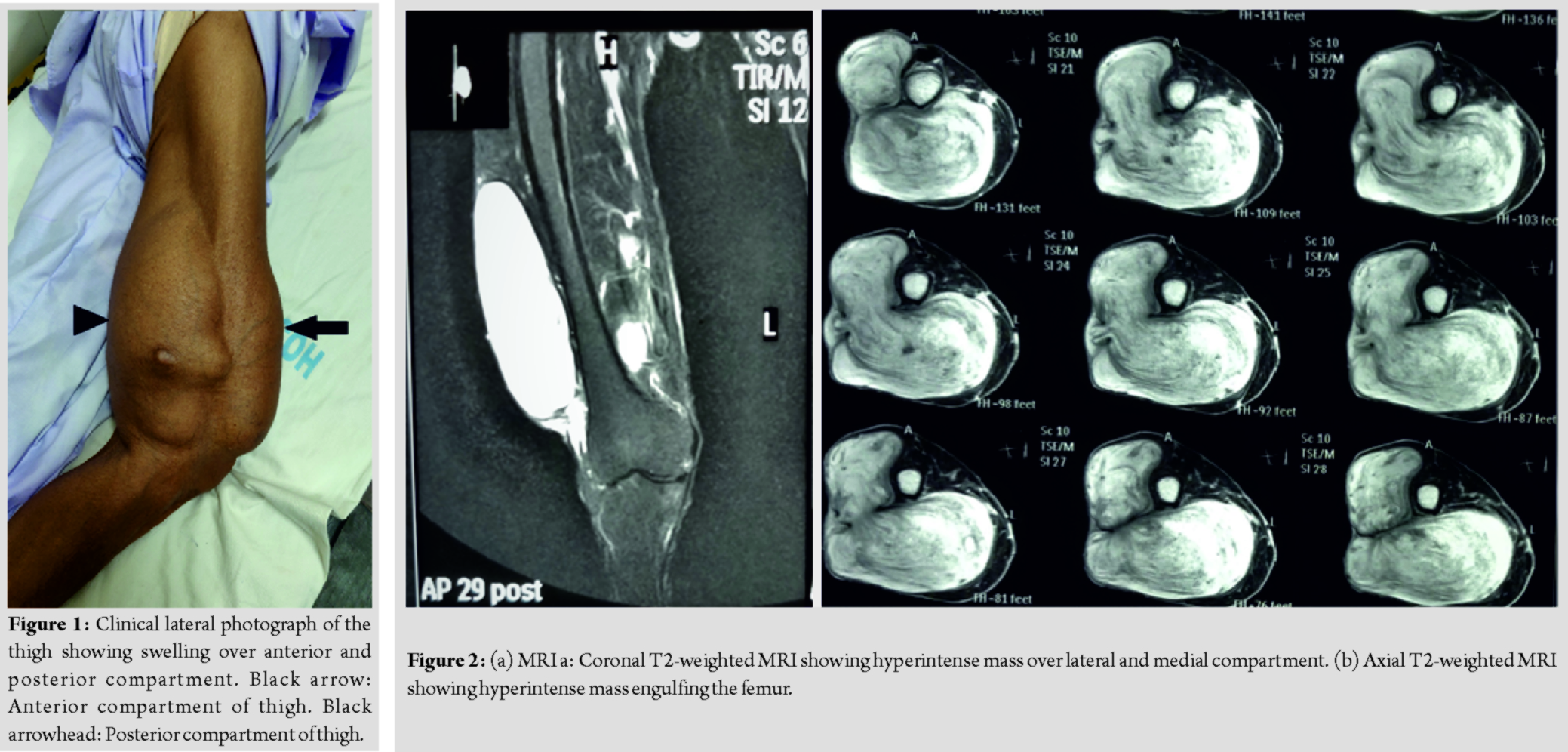
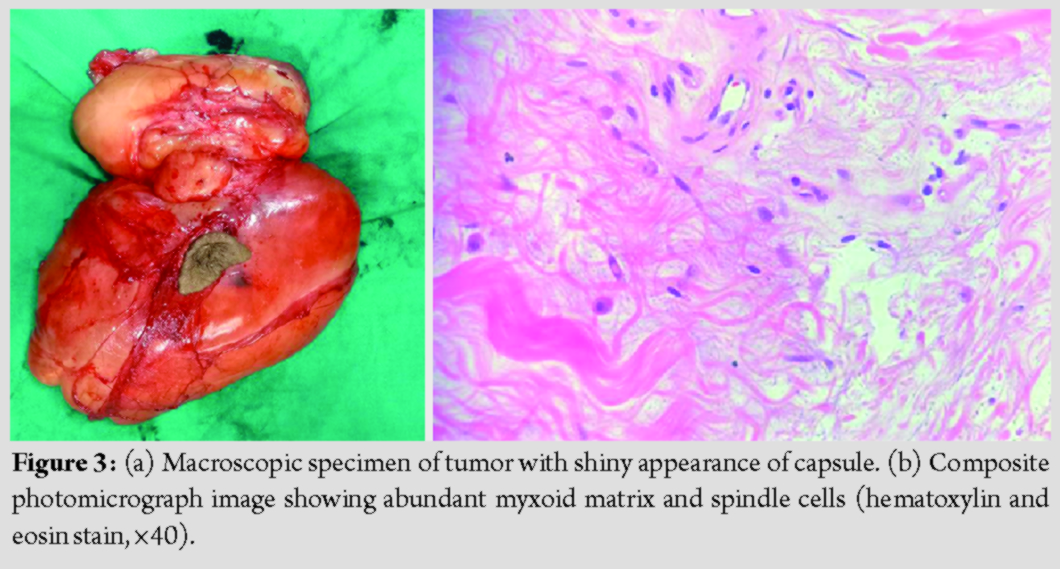
Medial as well lateral extensions were diffuse. The plain radiograph of the limb showed no bony involvement. Magnetic resonance imaging (MRI) revealed a well circumscribed encapsulated lobulated soft tissue mass measuring 25 × 15.5 × 10cm in the lower half of the thigh appearing heterogeneously hyperintense on T2 STIR sequence with a T2 hypointense rim and a hypointense T1, giving a whorled appearance. The mass was located mainly in the posterior compartment (just deep to superficial fascia and intermuscular planes), extending into anterior compartment along the lateral aspect of thigh caudally extending up to levels of the femoral condyles (Fig. 2a and b). No obvious invasion of the neurovascular bundle was seen; however, it was displaced medially lying in close proximity to the swelling. Tumor workup such as computed tomography of the chest and ultrasonography of the abdomen was normal. Routine blood investigations revealed mild anemia and ESR of 24mm/h. A biopsy was performed which was suggestive of a benign myxoid neoplasm. Having obtained the pathological diagnosis, surgical excision was planned for which due consent was obtained. Excision was performed by a single curvilinear incision over the posterior thigh, curving from superomedial to inferolateral direction, incorporating the biopsy site into it. The tumor was identified as swelling with a shiny white capsule, with rubbery consistency, lying in a subcutaneous plane extending to the intermuscular plane. The tumor was excised en-bloc without any spillage measuring 23 × 18 × 6 (Fig. 3a). The post-operative period was uneventful with no neurovascular deficit. Histopathology report showed moderately cellular growth with an abundant myxoid matrix containing oval to spindle cells with monomorphic nuclei and bland chromatin. No nuclear atypia or increased mitosis was seen (Fig. 3b). Immunohistochemistry markers were done which revealed accentuation of blood vessels on SMA, which was negative in tumor cells, few cells positive for S-100 and Ki-67 was <1% indicative of low proliferative index. Histopathological diagnosis was consistent with intramuscular myxoma. At the final follow-up of 26 months, the patient was asymptomatic and showed no signs of recurrence.
Discussion
The term myxoma was first used by Virchow (1871) to describe a tumor that resembled the substance of umbilical cord histopathologically [3]. Literature suggests that they originate from primitive mesenchymal cells, which have lost their capacity to produce collagen but instead produce copious amounts of hyaluronic acid and immature collagen fibers [4]. Clinically, the tumor is hallmarked by painless, palpable, and slow-growing lesion which has a plethora of myxoid matrix histopathologically. Although they are most commonly intramuscular in location (82%), they can rarely be intermuscular or subcutaneous [2]. As the lesion grows in size and manifests pressure symptoms (the first symptom being pain), the patient reports to the clinic and encourages further diagnostics. In the literature available, pain is described as the first symptom of the tumor, which is observed in 6–34% of patients [5]. In our case, the lesion was painless initially; however, in due course, the patient presented with pain and pressure symptoms. Intramuscular myxomas affect the musculoskeletal system with an incidence of 0.1–0.13/100,000. There is a slight preponderance for female sex and the mean age of affection is 50–60 years [2]. The thigh is the common site of involvement seen in 51% patients, followed by upper arm (9%), calf (7%), and rarely in buttocks [4]. The tumor manifests as either a solitary lesion or in association with fibrous dysplasia such as Mazabraud’s syndrome [3] or McCune–Albright syndrome [4]. The radiological diagnostic criteria for soft tissue myxomas were specified by Peterson [5] and then modified by Bancroft [6] and Murphey. Myxoid matrix has high water content as a result of which there is the hypoechoic appearance of these lesions on USG, low signal attenuation on CT scan, hypo-intensity on T1, and hyper-intensity on T2-weighted MRI images [7]. The typical picture of an intramuscular myxoma in MRI is a lesion within a muscle (or rarely intermuscular), which has fluid signal intensities, fatty tissue capsule, and T2 hyperintense signal from the surrounding muscle. It also helps surgical planning by evaluating the precise soft tissue extensions of the tumor along with neurovascular affections, if any. MRI image was characteristically synonymous with an intramuscular myxoid tumor. The gold standard for the diagnosis, however, remains histopathological examination [8]. Tumors of myxomatous origin are notorious for the invasion of surrounding musculature; hence, radical excision without spillage is advocated which ensures long and lasting recovery. The rate of local recurrence is as low as <10% and no case of distant metastasis has been described in the literature as of yet [3]. Hence, neither adjuvant nor neoadjuvant chemoradiotherapy is recommended. In our case, there was no recurrence at follow-up of 26 months.
Conclusion
Intramuscular myxomas are benign soft tissue lesions in which surgical excision is curative. An elderly patient presenting with a solitary soft tissue tumor should, therefore, be thoroughly investigated to rule out the soft tissue sarcomatous conditions.
Clinical Message
This case highlights that a giant swelling over thigh in elderly patient warrants a thorough investigation to rule out soft tissue sarcomas. It also focuses on the fact that radical resection is a must to prevent recurrence.
References
1. Enzinger FM. Intramuscular myxoma; a review and follow-up study of 34 cases. Am J Clin Pathol 1965;43:104-13.
2. Baheti AD, Tirumani SH, Rosenthal MH, Howard SA, Shinagare AB, Ramaiya NH, et al. Myxoid soft-tissue neoplasms: Comprehensive update of the taxonomy and MRI features. Am J Roentgenol 2015;204:374-85.
3. Spychała A, Murawa D, Niziołek A. Intramuscular myxoma of the left leg-case report of the lesion observed for several years. Rep Pract Oncol Radiother 2011;16:71-4.
4. Logel RJ. Recurrent intramuscular myxoma associated with Albright’s syndrome. J Bone Joint Surg Am 1976;58:565-8.
5. Peterson KK, Renfrew DL, Feddersen RM, Buckwalter JA, el-Khoury GY. Magnetic resonance imaging of myxoid containing tumors. Skeletal Radiol 1991;20:245-50.
6. Bancroft LW, Kransdorf MJ, Menke DM, O’Connor MI, Foster WC. Intramuscular myxoma: Characteristic MR imaging features. Am J Roentgenol 2002;178:1255-9.
7. Walker EA, Fenton ME, Salesky JS, Murphey MD. Magnetic resonance imaging of benign soft tissue neoplasms in adults. Radiol Clin North Am 2011;49:1197-217.
8. Yaligod V, Ajoy S M. Intramuscular Myxoma – A Rare Tumor. Journal of Orthopaedic Case Reports 2013 Oct-Dec ;3(4): 38-41.
 |
 |
 |
 |
| Dr. Manjeet Singh | Dr. Subodh Kumar Pathak | Dr. Vishesh Verma | Dr. Praveen Thivari |
| How to Cite This Article: Singh M, PathakSK, VermaV, ThivariP. Giant Intramuscular Myxoma of Thigh – A Rare Case Report. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 60-62. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


