
[box type=”bio”] Learning Point of the Article: [/box]
To expect the unexpected case during an emergency trauma call and the ability to go by the principles – A message to all young surgeons.
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 63-66 | S Gokulprasath, K R Tarun Prashanth. DOI: 10.13107/jocr.2020.v10.i03.1752
Authors: S Gokulprasath[1], K R Tarun Prashanth[1]
[1]Department of Orthopaedic Surgery, Sri Ramachandra Medical College and Research Institute, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India.
Address of Correspondence:
Dr. S Gokulprasath,
Department of Orthopaedic Surgery, Sri Ramachandra Medical College and Research Institute, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai, Tamil Nadu, India.
E-mail: gokulsrinivasan272762@gmail.com
Abstract
Introduction: Combined subtrochanteric femur fracture with anterior dislocation of hip is a very rare injury to occur with subminimal reported cases available in the literature. This study report describes one such unusual case presentation.
Case Report: A 26-year-old gentleman presented to our emergency room following road traffic accident, complained of severe pain over his right hip and inability to move his right lower limb. The hip was diffusely swollen and the lower limb externally rotated, clinical and radiological evaluation revealed anterior dislocation of the right hip with ipsilateral subtrochanteric femur fracture. Emergency closed reduction of the right hip was performed using joystick maneuver with two Schanz pins and concomitantly the subtrochanteric fracture reduced, and uniplanar external fixator was applied on the same day of presentation. Following 2 days, external fixator removal and IMIL nailing were performed as an elective definitive procedure. The patient was regularly followed up both clinically and radiologically from the index procedure until now with 2 years as follow-up.
Conclusion: Anterior hip dislocation with ipsilateral subtrochanteric femur fracture in a young adult requires early emergency evaluation and rapid intervention (reduction within 6 h) and early closed reduction of the joint helps decreasing the risk of complications such as avascular necrosis and chondrolysis and joint reduction with fracture fixation allows early rehabilitation.
Keywords: Anterior hip dislocation, subtrochanteric femur fracture, fracture dislocation.
Introduction
Hip joint (coxofemoral joint) is a very stable joint and implies a high degree of stability which is why dislocations usually occur following a high-energy trauma (road traffic accident [RTA], industrial accidents, and sports injuries) [1]. Posterior dislocation of hip is very common and approximately 9 times more frequent than the anterior dislocation because of its most common mode of injury (dashboard injury) and due to its severity of impact, it may be associated with fractures of various patterns [2, 3, 4]. However, hip dislocation associated with fracture of neck or shaft of femur is very rare and only a few cases have been described [5]. The combination of anterior dislocation of hip with associated ipsilateral subtrochanteric femur fracture is very rare and literature evidence is very scarce until now and hence a very challenging injury to treat. These high-energy injuries may result in significant morbidity and loss of function as a consequence to avascular necrosis (AVN) and secondary osteoarthritis when they occur in young individuals [6, 7]. Forceful abduction is the most important factor in producing anterior dislocation and thereby in this position, neck or trochanter impinges on acetabular rim and forces the head of femur forward through anterior capsule. These cases are usually associated with significant trauma and many patients will have concomitant injuries. Subtrochanteric femur fractures are generally defined as those fractures occurring within 5 cm of the distal extent of the lesser trochanter and represent an unstable injury. These fractures usually occur in young adults when high-velocity injury happens. Furthermore, these fractures present a challenge for the treating surgeon, as the deforming force on both the proximal and distal segments is difficult to control. The most probable cause of this presentation may be due to the high-velocity vector force acting in the subtrochanteric region associated with a twisting force, leading to an abduction, flexion, and external rotation of the proximal fragment which there on move the femoral head anterior to the anterior acetabular rim and causes to terminally dislocate due to the high energy. The aim of this paper is to report on how to manage a rare case of anterior hip dislocation with ipsilateral subtrochanteric femur fracture and its clinical and radiological outcome.
Case Report
A 26-year-old male, a young adult who is a welder by occupation, was brought on new year’s eve of 2017 to the emergency room following a history of RTA when he fell over from his motorbike as he was about to crash into a stationary vehicle and sustained injury to his right thigh, he was brought within 2 h after sustaining trauma and complained of severe pain over his right hip and inability to move his right lower limb. On examination, he was conscious and oriented, hemodynamically stable, and unable to move his right lower limb which was externally rotated and shortened with a diffusely swollen upper thigh. He had tenderness over the right groin area with a palpable lump. Distal neurovascular examination was normal. Radiographic evaluation of pelvis and right thigh revealed right hip anterior dislocation with ipsilateral subtrochanteric femur fracture (Fig. 1).
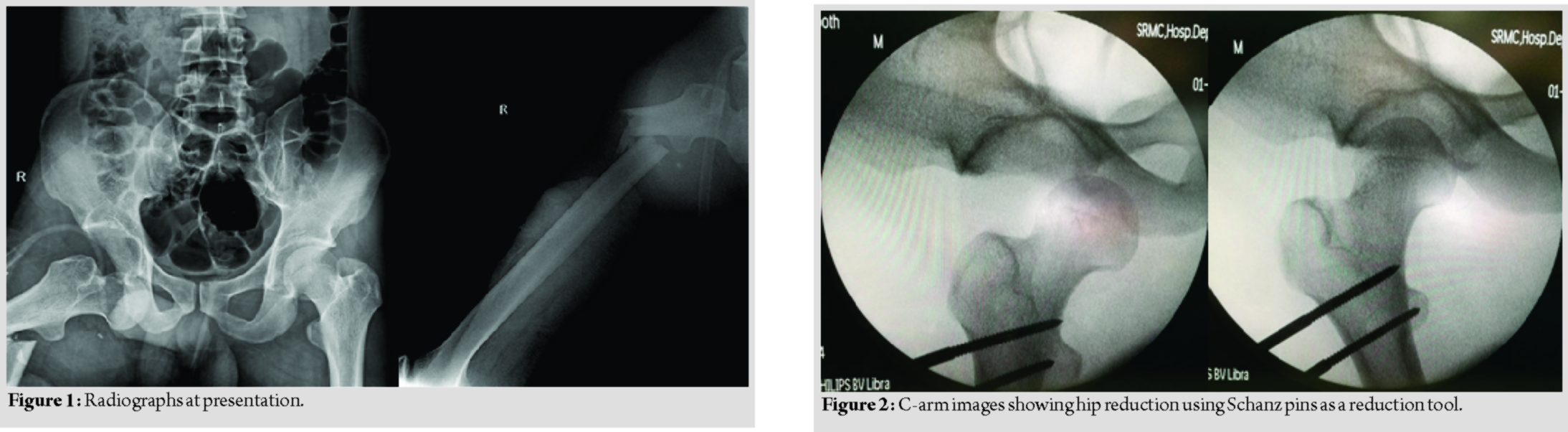
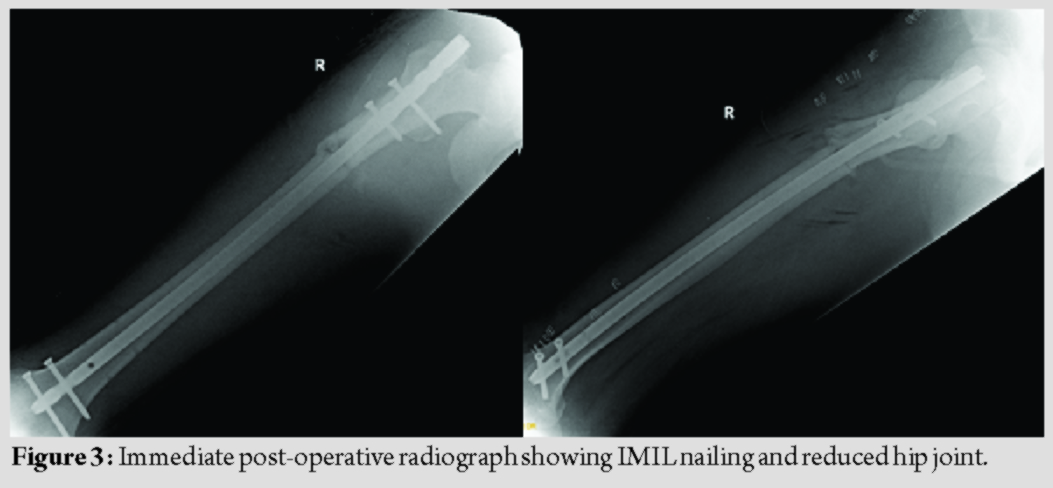
The patient was worked up for surgery immediately and emergency surgical intervention to reduce the hip was planned. After inducing anesthesia, no attempts of closed reduction using the various techniques to reduce the anterior dislocation were tried as the patient had an ipsilateral femur fracture because all the forces pass through the fracture site. Therefore, the patient was placed on a radiolucent table and with a help of image intensifier, under strict sterile precaution, initially, one 5 mm Schanz pin was placed close to the intertrochanteric region and used as a joystick to reduce the head into the acetabulum but was unsuccessful; hence, another Schanz pin was placed parallelly and connected with each other using a pin to rod connector and then the rod along with the pins was used as an external reduction tool to reduce the right hip in a closed manner without the need of open reduction, thereby reducing the chances of vascular insult on the capsule. The closed reduction was found to be satisfactory as checked under the image intensifier (Fig. 2) and further reduction of the subtrochanteric region was done and a uniplanar external fixator was applied as a temporary procedure. This emergency procedure was done within 6 h of the insult. After 2 days, the patient was taken up for definitive procedure in the form of external fixator removal and closed reduction and intramedullary interlocking nailing using a cephalomedullary nail but used as IMIL nail (Fig. 3) with the patient placed on a fracture table under C-arm guidance. Postoperatively, regular wound inspections and dressings were done and wound was found to be healthy.
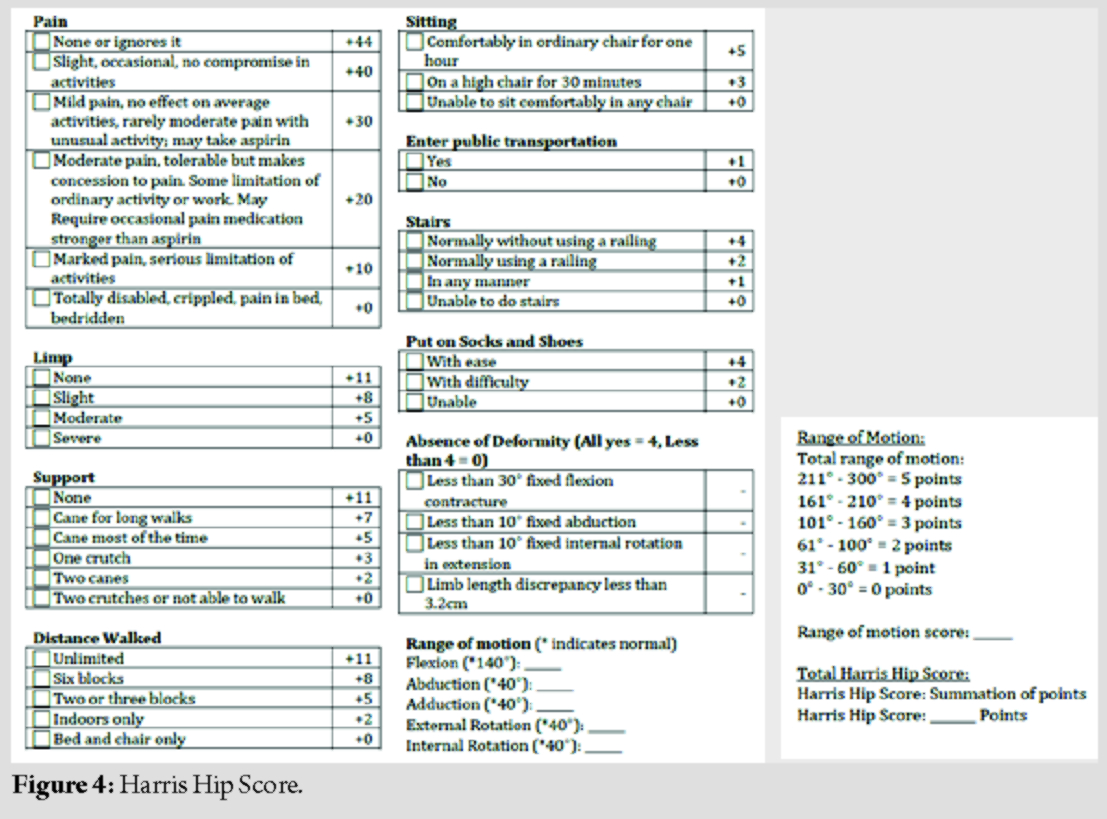
The patient was started on non-weight-bearing mobilization for 2 weeks initially and then was started on weight-bearing as tolerated and gently to full weight-bearing. The patient was also started on physiotherapy in the form of hip exercises at the end of 6 weeks. The patient resumed his daily work and had not faced any challenges. Functional assessment was done using Harris Hip Score (Fig. 4) at 6 weeks, 3 months, 1 year and 2 years follow-up.
Radiological assessment was done at the time of 2 months (Fig. 5) and regularly until 2 years follow-up to check for fracture union and to rule out AVN of femoral head, secondary arthritis, and implant loosening.
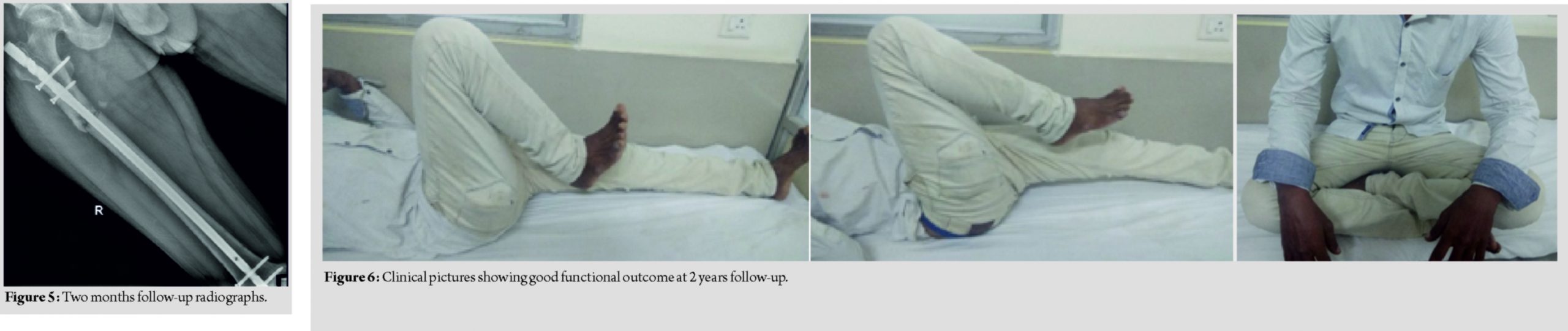
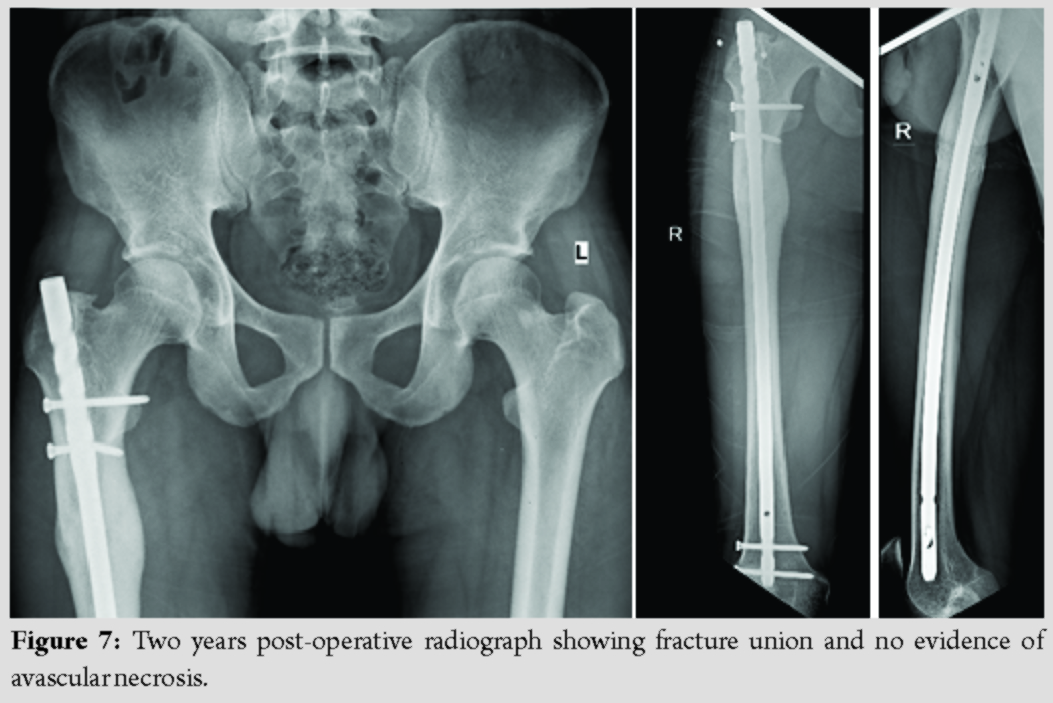
At 2 years follow-up, Harris Hip Score was found to be 95 with no restriction of movements (Fig. 6) and fracture was united completely with no evidence of AVN and secondary osteoarthritis in the femoral head (Fig. 7).
Discussion
Dislocation of hip is an orthopedic emergency which usually occurs due to high-energy trauma and it must be reduced as soon as possible (within 6 hours) to avoid complications such as avascular necrosis (AVN) and secondary osteoarthritis. Hip dislocations are usually associated with injury to femoral head, neck or shaft of femur, and acetabulum [8]. A posterior dislocation of hip associated with femoral head, neck, or shaft fracture is very unusual but not rare entity, but of that anterior hip dislocation with subtrochanteric femur fracture is very rare according to the literature support.The main peculiarity of our case is the anterior dislocation of the femoral head association with subtrochanteric femur fracture and the difficulty in the management of reduction of the hip and the treatment of the subtrochanteric fracture and its excellent clinical and radiological outcome after 2 years following the surgery. Addition to that, subtrochanteric femur fractures are very challenging due to its deforming force. Significant fracture displacement occurs due to the secondary pull of iliopsoas, gluteus medius, and short external rotators on the proximal fragment and pulls this segment into a position of flexion, abduction, and external rotation. Further, the unopposed pull of the adductors on the distal segment often leads to femoral shortening and adduction. These deforming forces need to be overcome in order to achieve an anatomical reduction. In our case, forceful abduction is the most important factor contributing to anterior dislocation with associated direct impact high-velocity injury leads to subtrochanteric femur fracture. Such injuries are orthopedic emergencies and require immediate surgical intervention. The biggest difficulty faced in this case is the need of achieving emergency reduction and the method of attempting closed reduction and maintaining reduction. The reason being that the proximal fragment cannot be reduced using the conventional reduction maneuvers described in literature, that as its discontinuity from the shaft cannot aid in its movement when the limb is pulled in traction. And that, the need of open reduction may cause an insult to the femoral head as it may require an incision to the anterior capsule in order to reduce the femoral head. The various studies in pertinence to anterior fracture dislocation of the hip are tabulated below. The main complications following this type of rare presentation usually will be avascular necrosis (AVN) of femoral head and secondary osteoarthritis usually more in patients with an ipsilateral neck as well as in old age. Thus, early reduction in the dislocated hip decreases the risk of AVN. A delay of more than 6 hours increases the risk of AVN from 10 to 40%. But However, we did not encounter this complication in our case at 2-year follow-up. Femoral head was reduced under GA and external fixator was applied temporarily to reduce the subtrochanteric fracture and then IMIL nailing was done on the second day. Non-weight-bearing mobilization was started from the 2nd post-operative day and then it was changed gradually into full weight-bearing walking at the end of 6 weeks. At 2 years follow-up after surgery, the radiographic assessment showed stable joint without any evidence of AVN and complete healing of fracture with good functional outcome with Harris Hip Score of 95.
Conclusion
Anterior hip dislocation associated with ipsilateral subtrochanteric femur fracture is a rare case and challenging injury to treat due to its deforming force and reduction difficulty. Early emergency evaluation and rapid surgical intervention in these cases can give a good clinical and radiological outcome. Closed reduction should be attempted in such cases with the help of percutaneous Schanz pins placed in the dislocated fragment and reduced by joystick maneuver. Early intervention achieving stable congruent joint reduction and definitive fracture fixation thereby allow an early rehabilitation and reduce the risk of complications.
Clinical Message
The idea of presenting this case is to report and reflect the various ways, in which a rare trauma can present to an emergency room and the necessary thought process to use your clinical and technical acumen on treating a rare case of anterior hip dislocation associated with subtrochanteric femur fracture and the importance of rapid evaluation and emergency intervention.
References
1. Mascioli AA. Acute dislocations. In: Azar FM, Beaty JH, Canale ST, editors. Campbell’s Opertive Orthopaedics. 13th ed., Ch. 60. Philadelphia, PA: Elsevier; 2017.
2. Brav EA. Traumatic dislocation of the hip. J Bone Joint Surg Am 1962;44:1115-34.
3. Dreinhofer KE, Schwarzkopf SR, Haas NP, Tscherne H. Isolated traumatic dislocation of the hip. J Bone Joint Surg Br 1994;76:6-12.
4. Raja JA, Valsalan BP. A Case of Anterior Dislocation of Hip Associated with an Unusual Pattern of Fracture of Proximal Femur. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 34-35.
5. Reggiori A, Brugo G. Traumatic anterior hip dislocation associated with anterior and inferior iliac spines avulsions and a capsular-labral tear. Strategies Trauma Limb Reconstr 2008;3:39-43.
6. Pipkin G. Treatment of grade IV fracture-dislocation of the hip a review. J Bone Joint Surg Am 1957;39:1027-197.
7. Stewart MJ, Milford LW. Fracture-dislocation of the hip. An end-result study. J Bone Joint Surg Am 1954;36:315-42.
8. Radulescu R, Badila A, Japie I, Papuc A, Manolescu R. Anterior dislocation of the hip associated with intertrochanteric fracture of the femur-case presentation. J Med Life2013;6:336-9.
9. McClelland SJ, Bauman PA, Medley CF Jr., Shelton ML. Obturator hip dislocation with ipsilateral fractures of the femoral head and femoral neck. A case report. Clin Orthop Relat Res 1987;224:164-8.
10. Richards BS, Howe DJ.Anterior perineal dislocation of the hip with fracture of the femoral head. A case report.Clin Orthop Relat Res1988;228:194-201.
11. Sadler AH, DiStefano M.Anterior dislocation of the hip with ipsilateral basicervical fracture. A case report.J Bone Joint Surg Am 1985;67:326-9.
12. Esenkaya I, Gorgec M. Traumatic anterior dislocation of the hip associated with ipsilateral femoral neck fracture: a case report. Acta Orthop Traumatol Turc. 2002;36(4):366–368.
 |
 |
| Dr. S Gokulprasath | Dr. K R Tarun Prashanth |
| How to Cite This Article: Gokulprasath S, Prashanth KRT, Anterior hip dislocation with ipsilateral subtrochanteric femur fracture in a young adult – A rare case report.. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 63-66. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


