
[box type=”bio”] Learning Point of the Article: [/box]
Scapholunate Dissociation with Ulnar Impaction: A Case with Review of Literature
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 79-79 | Bipul K. Garg, Harshit Dave. DOI: 10.13107/jocr.2020.v10.i03.1758
Authors: Bipul K. Garg[1], Harshit Dave[1]
[1]Department of Orthopaedic Surgery, Sir J.J. Group of Hospitals and Grant Medical College, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Bipul K. Garg,
Department of Orthopaedic Surgery, Sir J.J. Group of Hospitals and Grant Medical College, Mumbai – 400 008, Maharashtra, India.
E-mail: garg.bipul@gmail.com
Abstract
Introduction: Scapholunate dissociation and ulnar impaction syndrome are common causes of wrist pain but often missed on initial clinical and radiological evaluation; hence, diagnosis is delayed. Management is challenging as there is diversity in surgical option. There is not a single case in literature described for both scapholunate dissociation and ulnar impaction syndrome treated in one setting. We are presenting a case of both ulnar impaction syndrome and scapholunate dissociation treated surgically in one setting with good functional outcome.
Case Report: A 30-year-old male with chronic scapholunate dissociation and ulnar impaction syndrome treated with modified Brunelli technique for scapholunate dissociation and extra-articular ulnar shortening osteotomy for ulnar impaction syndrome in one setting with good functional outcome.
Conclusion: In cases with scapholunate dissociation and ulnar impaction syndrome, treatment should be directed toward both. When done with careful pre-operative evaluation and planning in one setting, can yield favorable results.
Keywords: Scapholunate dissociation, ulnar impaction, modified Brunelli technique.
Introduction
Scapholunate dissociation is the most common type of carpal instability with a fall on the outstretched hand being the most common mode of injury [1]. An impact load to the hypothenar area of an extended and supinated wrist in ulnar deviation is thought to be a likely mechanism of scapholunate dissociation where the capitate driven proximally between the scaphoid and the lunate forcing them in opposite directions [2]. Patients typically present with symptoms suggestive of a scaphoid fracture, but with negative radiographs. An increase in the scapholunate gap of more than 2 mm is abnormal [3]. Several treatment options have been developed, including a limited intercarpal arthrodesis, bone-ligament- bone graft or soft-tissue stabilization with tenodesis described initially by Brunelli and Brunelli [4] and later modified by Van Den Abbeele et al. [5], being the most widely used. The technique aims to prevent instability using a split flexor carpi radialis tendon transfer to reconstruct the disrupted ligaments. The transferred tendon has been shown to replace the action of the scapholunate ligament and the dorsal intercarpal ligament and reduces the ulnar translation of the triquetrum and lunate [6]. The ulnar impaction syndrome is characterized by impaction of the ulnar head against the triangular fibrocartilage complex, lunate, and triquetrum resulting in progressive degeneration of these structures. Patients commonly present with ulnar sided wrist pain and clicking, often with a history of trauma or repetitive axial loading and rotation [7]. The etiology of this condition is related to a relatively long ulnar height compared with the radius at the wrist. The relative length of the ulna compared to the radius is expressed as ulnar variance, where a neutral variance is dictated by a difference of less than 1 mm from the radius. Treatment strategies consist of conservative management, arthroscopic debridement or repair, arthroscopic wafer procedure, or ulnar shortening osteotomy. The most common procedures used for ulnar impaction syndrome are an ulnar shortening osteotomy or an open or arthroscopic distal wafer resection with or without triangular fibrocartilage complex débridement [8]. Woitzik et al. in his case series described that in case of positive ulnar variance more than 2 mm, extra-articular ulnar shortening osteotomy is the best choice and when ulnar variance <2 mm with central or peripheral perforation of triangular fibrocartilage complex arthroscopic wafer surgery is the treatment of choice. When both scapholunate dissociation and ulnar impaction syndrome occur simultaneous treatment should be considered for both, only treating scapholunate dissociation or ulnar impaction alone will not be helpful. Here, we are presenting a case of both ulnar impaction syndrome and scapholunate dissociation treated surgically in one setting with good functional outcome.
Case Report
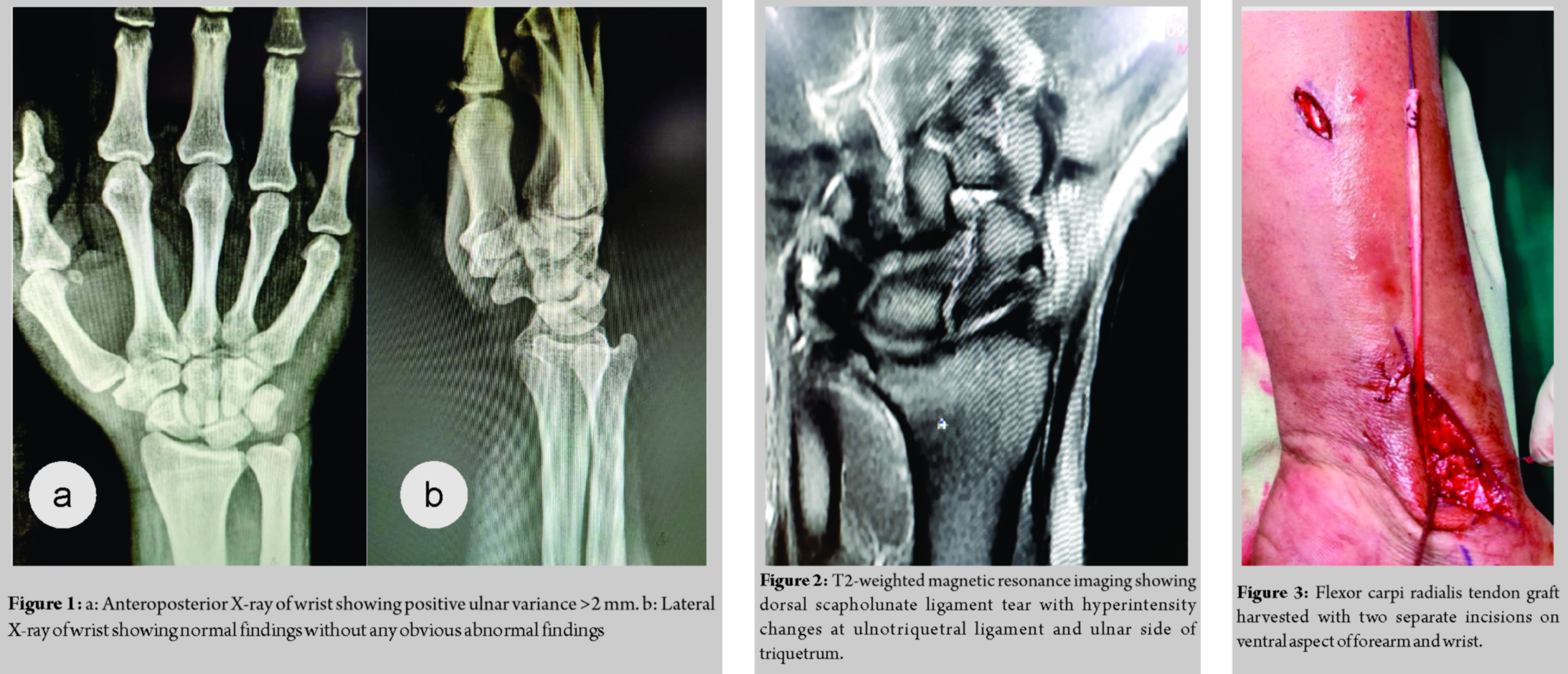
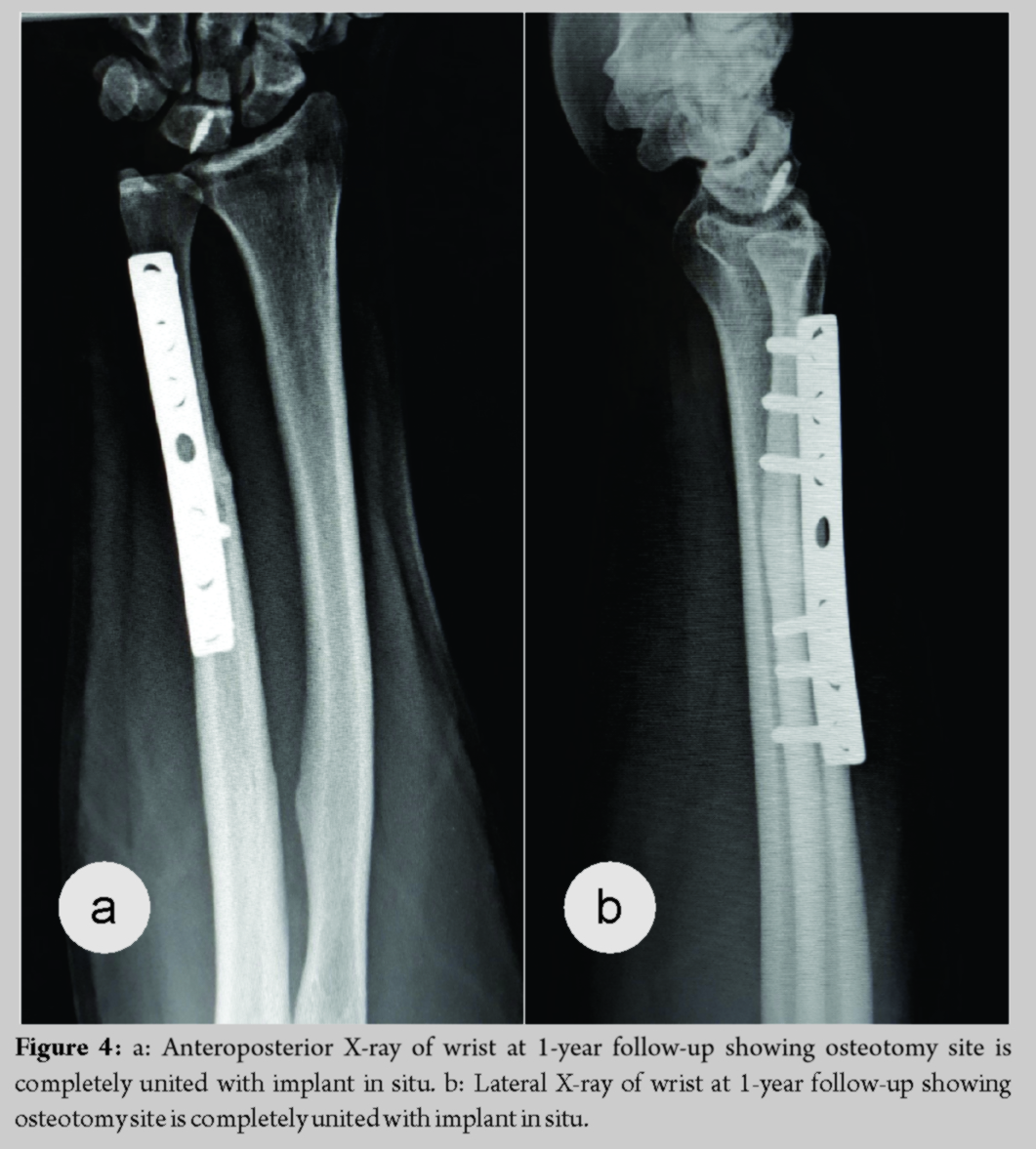
A 30-year-old male complains of the right wrist pain for 6 months due to fall on an outstretched hand. The patient was treated with below elbow cast for 6 weeks. Since then, the patient had wrist pain around ulnar the head by clicking on pronation, palmar flexion, and ulnar deviation. Range of motion was painful after 70° of palmar flexion, 10° of ulnar deviation with pronation. The scaphoid shift test and fovea sign test were negative whereas ulnocarpal stress test was positive. Anteroposterior view of wrist X-ray showed positive ulnar variance >2 mm, whereas the lateral view showed normal findings (Fig. 1). Magnetic resonance imaging (MRI) revealed dorsal scapholunate ligament tear with hyperintensity changes of ulnotriquetral ligament and ulnar side of the triquetrum (Fig. 2). Pre-operative disabilities of the arm, shoulder, and hand (DASH) score was 40.4 and visual analog score (VAS) score was 7. The patient was planned for modified Brunelli technique proposed by Elsaftawy et al. in which reconstruction of the scapholunate ligament with transfer of partial flexor carpi radialis tendon (Fig. 3) from plantar to the dorsal side through the distal pole of scaphoid and is anchored to the lunate with a specialized suture anchor, and extra-articular ulnar shortening osteotomy for positive ulnar variance in one setting. The patient was kept in below elbow dorsal slab for 6 weeks. After 6 weeks, wrist range of motion was gradually started. Heavy work started after 3 months. The patient had full range of motion at 6 months with DASH score of 10 and VAS score of 1 with complete radiological union at 1-year follow-up (Fig. 4).
Discussion
Scapholunate dissociation and ulnar impaction syndrome are often missed on initial clinical and radiological evaluation and hence diagnosis is delayed. The result of long-standing scapholunate ligament injury with dissociation is always dorsal intercalated segment instability and a so-called scapholunate advanced collapse wrist [6]. Scapholunate advanced collapse wrist is the most common pattern of degenerative arthritis of the wrist. Scapholunate stability is dependent on the scapholunate interosseous ligament, in particular, the dorsal part and the secondary scaphoid stabilizers, the extrinsic capsular ligaments which include the radioscaphoid, scaphotrapezial-trapezoidal, dorsal intercarpal, and dorsal radiocarpal ligaments. The scapholunate complex plays a significant role in the transmission of force across the wrist and on the carpal motion. When the diagnosis is made early, outcomes are better. Hence, they should be considered in the differential diagnosis of any patient who presents with non-resolving wrist pain with normal radiographs and should be managed with proper pre-operative planning as there is much diversity for surgical management of scapholunate dissociation.
Several treatment options for scapholunate dissociation have been developed with tenodesis described initially by Brunelli and Brunelli [4] and later modified by Van Den Abbeele et al.[5], being the most widely used. Brunelli described a procedure where a strip of flexor carpi radialis was passed through a tunnel in the distal pole of the scaphoid and pulled dorsally to reduce the flexed attitude of the scaphoid. The tendon was then sutured to the dorsum of the distal radius. This stabilized the proximal and distal ends of the subluxating scaphoid. The major drawback of this procedure was the significant reduction in wrist flexion, primarily due to the placement of the flexor carpi radialis tendon onto the radius. Van Den Abbeele et al. subsequently modified this procedure by suturing the tendon to the dorsal radiotriquetral ligament instead of the radius. Modified Brunelli procedure of Van Den Abbeele et al. proved to work very well in reducing the scapholunate gap and rotatory subluxation of the scaphoid, however, it may limit the wrist movements because of the involvement of dorsal extrinsic ligaments. Garcia-Elias et al. described his own modification of this procedure in 2006 and called it the three-ligament tenodesis for the treatment of scapholunate dissociation, however, it may limit the wrist movements because of involvement of dorsal extrinsic ligaments [7]. Elsaftawy et al. in 2014 proposed modification of Brunelli technique in which using flexor carpi radialis tendon graft through a hole created in distal part of the scaphoid, then flexor carpi radialis tendon is anchored to the lunate create a kind of axial lever that can fully reconstruct the anatomical relationship between the scaphoid and the lunate, with no involvement of extrinsic ligaments, and with simultaneous restriction of pathological alignment of the scaphoid [9].
The ulnar impaction syndrome is yet another cause of wrist pain that can cause considerable disability. The most common procedures used to address ulnar impaction syndrome are ulnar shortening osteotomy, open or arthroscopic distal wafer resection with or without triangular fibrocartilage complex debridement. Advantages of an ulnar shortening osteotomy include unloading the ulnar carpus, precise shortening, tightening the ulnocarpal ligament complex, and avoiding damage to the distal articular surface of the ulna [10]. Woitzik et al. [8] in his case series described that positive ulnar variance more than 2 mm, extra-articular diaphyseal ulnar shortening osteotomy is the best choice and when ulnar variance <2 mm with central or peripheral perforation of triangular fibrocartilage complex arthroscopic wafer surgery is the treatment of choice. We presented a case of 30-year-old male who presented with complaints of wrist pain with significant restriction to carry out daily activities. Initial radiographs were essentially normal, and hence, scapholunate dissociation with ulnar impaction syndrome was missed initially and was diagnosed with dynamic imaging and MRI. The patient was managed with modified Brunelli technique proposed by Elsaftawy et al. in 2014 and extra-articular ulnar diaphyseal shortening step cut osteotomy as described above in one setting. The patient improved significantly over 3 months postoperatively with the DASH improving significantly from 40 to 10 over 6 months and VAS scores from 7 to 1. Now, post-operative 1 year, the patient is symptom free and full range of motion with the radiological union at ulnar shortening osteotomy site.
Conclusion
Scapholunate dissociation with positive ulnar variance, ulnar impaction syndrome precipitates early so treatment should be directed toward both. Both these conditions are common causes of wrist pain, but are often missed on initial radiographs and hence present late and can be significantly disabling. Modified Brunelli procedure for scapholunate dissociation and extra-articular diaphyseal ulnar shortening osteotomy for ulnar impaction syndrome, when done with careful pre-operative evaluation and planning in one setting, can yield favorable results.
Clinical Message
Scapholunate dissociation with ulnar impaction syndrome when managed with careful pre-operative evaluation and planning can yield favorable results.
References
1. Larsen CF, Amadio PC, Gilula LA, Hodge JC. Analysis of carpal instability: I. Description of the scheme. J Hand Surg 1995;20:757-64.
2. Mayfield JK. Mechanism of carpal injuries. Clin Orthop Relat Res 1980;149:45-54.
3. Kindynis P, Resnick D, Kang HS, Haller J, Sartoris DJ. Demonstration of the scapholunate space with radiography. Radiology 1990;175:278-80.
4. Brunelli GA, Brunelli GR. A new surgical technique for carpal instability with scapho-lunar dislocation. (Eleven cases). Ann Hand Upper Limb Surg 1995;14:207-13.
5. Van Den Abbeele KL, Loh YC, Stanley JK, Trail IA, Early results of a modified Brunelli procedure for scapholunate instability. J Hand Surg 1998;23B:258-61.
6. Garcia-Elias M, Lluch AL, Stanley JK. Three-ligament tenodesis for the treatment of scapholunate dissociation: Indications and surgical technique. J Hand Surg 2006;31:125-34.
7. Tomiano MM, Elfer J. Ulnar impaction syndrome. Hand Clin 2005;21:567.
8. Woitzik E, deGraauw C, Easter B. Ulnar Impaction Syndrome: A case series investigating the appropriate diagnosis, management, and post-operative considerations. J Can Chiropr Assoc 2014;58:401.
9. Elsaftawy A, Jabłecki J, Jurek T, Domanasiewicz A, Gworys B. New concept of scapholunate dissociation treatment and novel modification of Brunelli procedure anatomical study. BMC Musculoskelet Disord 2014;15:172.
10. McBeath R, Katolik LI, Shin EK. Ulnar shortening osteotomy for ulnar impaction syndrome. J Hand Surg 2013;38:379-81.
 |
 |
| Dr. Bipul K. Garg | Dr. Harshit Dave |
| How to Cite This Article: Garg BK, Dave H. Scapholunate Dissociation with Ulnar Impaction: A Case with Review of Literature. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 76-79. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


