
[box type=”bio”] Learning Point of the Article: [/box]
Tearing of the acromioclavicular joint disk may cause lingering symptoms in patients with prior trauma or injury involving their shoulder, however further study is needed to determine if these findings are truly causative or merely incidental.
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 90-94 | Andrew W Kuhn, John E Kuhn, Scott M LaTulip, James E Carpenter. DOI: 10.13107/jocr.2020.v10.i03.1764
Authors: Andrew W Kuhn[1], John E Kuhn[2], Scott M LaTulip[3], James E Carpenter[4]
[1]Department of Orthopaedic Surgery, Washington University in St. Louis, 660 S. Euclid Avenue, St. Louis, MO 63110 USA,
[2]Department of Orthopaedic Surgery and Rehabilitation, Vanderbilt University Medical Center, Medical Center East, South Tower, Suite 4200, 1215 21st Avenue, Nashville, TN 37232 USA,
[3]Department of Orthopaedic Surgery, Case Western Reserve University, 11100 Euclid Avenue, Cleveland, OH 44106-5043 USA,
[4]Department of Orthopaedic Surgery, University of Michigan Medical School, MedSport Domino’s Farms, 24 Frank Lloyd Wright Drive, Lobby A, Suite 1000, Ann Arbor, MI 48106 USA.
Address of Correspondence:
Dr. John E. Kuhn,
Department of Orthopaedic Surgery and Rehabilitation, Vanderbilt University Medical Center, Medical Center East, South Tower, Suite 4200, 1215 21st Avenue Nashville, TN 37232 USA.
E-mail: j.kuhn@vanderbilt.edu
Abstract
Introduction: Degeneration of the fibrocartilaginous acromioclavicular (AC) joint disk can become significant in later life and lead to primary osteoarthritis and shoulder pain. Younger, non-arthritic individuals may develop residual shoulder symptoms due to tearing of the disk itself.
Case Report: Six patients (seven shoulders) were included in this case series. They were athletic and between the ages of 17 and 22. They typically presented with lingering symptoms of pain, popping, and instability in and around the AC joint after prior trauma or injury involving their shoulder. For most, symptoms lasted longer than 2 months before they sought additional treatment. Plain films were negative, and magnetic resonance imaging occasionally demonstrated pathology at the AC joint. Conservative treatment provided limited relief. All patients included in this series underwent arthroscopic distal clavicle resection. Intraoperatively, the disk could be seen as acutely torn or degenerative in all cases. In some, it was hypermobile and could be manually subluxed in and out of the joint.
Conclusions: A torn AC joint disk may cause lingering symptoms in young patients without radiographic evidence of arthritis. Further study is needed to determine if these findings are truly causative or merely incidental.
Keywords: Acromioclavicular joint, shoulder, arthroscopy.
Introduction
The acromioclavicular (AC) joint is a diarthrodial joint, formed between the distal clavicle and anteromedial acromion. It is surrounded by a capsule containing an intra-articular synovium and fibrocartilaginous disk [1, 2]. The disk is thought to provide cushioning, correct for incongruences, and act in a load-bearing fashion, similar to the function of the meniscus in the knee [3, 4]. Beginning in the second and into the fourth decade of life, degeneration of the AC joint disk occurs [5]. The progression of AC joint disk degeneration has been observed in cadaveric specimens, with disks described as being “full,” “meniscoid like,” “remnants,” or “completely absent” [6]. In mature adults, the presence of a full disk in the AC joint cavity is relatively rare. Emura et al. [7] found that nearly 71% of the 52 cadaveric shoulders did not have an intra-articular disk in the AC joint cavity, whereas in roughly 25%, a disk divided the articular cavity incompletely and in 4%, completely. The disk tissue consists primarily of fibrocartilage, whereas the articular joint surfaces contain zones of fibrocartilage and hyaline cartilage [8]. Incongruity between the two opposing joint surfaces has been hypothesized as one of the underlying mechanisms of disk degeneration and progressive osteoarthritic changes seen within the AC joint [3]. While AC joint disk degeneration concomitant with the onset of primary osteoarthritis is a common cause of shoulder pain [9], younger individuals with pathology or tearing of a full or partial AC joint disk but without significant degenerative changes of the articular surfaces may become symptomatic as well [10]. However, to date, the identification, treatment, and outcomes of non-arthritic, symptomatic patients with damaged AC joint disks have not been described thoroughly in the literature or in athletic populations. In this case series, we report on the clinical and radiological outcomes of individuals who were treated for presumed symptomatic AC joint disk pathology. We provide discussion about whether or not these findings are causative or merely incidental.
Case Report
Six patients were included and averaged 19 years old (range: 17–22). Five were male and one was female. All were former or currently active in sports participation at the time of presentation. Sports participated in included: Ice hockey, collegiate tennis, collegiate football, collegiate wrestling, and high school cheer leading. Height and weight were available for five of the six patients averaging, 175.3 cm (range: 165.1 cm–180.3 cm) and 80.7 kg (range: 62.6 kg–103.4 kg) pounds, respectively, equating to an average body mass index of 26.4 (range: 21.5–32.7).
Injury history and clinical presentation
At presentation, all (6/6; 100%) patients reported a prior traumatic event or injury involving their shoulder, where half (3/6; 50.0%) sought prior care and received diagnoses including: Low grade (I/II) AC joint sprains (2/6; 33.3%) and a subscapularis partial tear, with mild partial thickness rotator cuff tearing and mild posterosuperior labral degeneration (1/6; 16.7%). For the other half, one was involved in a traumatic skiing accident where his left arm was pulled back into hyperabduction and hyperextension, and another believed his injury came about after heavy bench pressing exercises. The last, who had both shoulders evaluated and treated, was involved in a motor vehicle accident. The majority presented with lingering symptoms of minor to moderate pain localized primarily to the anterolateral aspect of their injured shoulder (5/6; 83.3%), clicking/popping sensations (5/6; 83.3%), and a feeling of instability (2/6; 33.3%). The popping was commonly reported to be exacerbated by activities of daily living. It was initially thought that in the patient with a diagnosed subscapularis partial tear, a flap moving in and out over the middle glenohumeral ligament was the source of symptomatic popping. However, even after debridement of the flap, he continued to report significant popping and instability. All patients without prior surgery failed conservative therapy, including corticosteroid injections and physical therapy. For most, symptoms lasted longer than 2 months before they sought additional treatment, including surgery. Two were athletes who were “in-season” and waited to have surgery until the end of their seasons. One had surgery 5 months post-injury and after failing non-operative management. The patient with bilateral shoulder pain resulting from a motor vehicle accident did not have surgery until 2–2.5 years after their injury.
Physical examination
Tenderness over the AC joint was a consistent finding on examination. Other findings were more variable. Some also demonstrated minimal tenderness at the biceps tendon, rotator cuff (supraspinatus), deltoid, and subacromial bursa in addition to their primary AC joint tenderness. The clicking/popping sensations were localized to the anterior aspect of the shoulder or the AC joint. Patients demonstrated popping with rotator cuff resistance maneuvers or with passive shoulder elevation and rotation. In one, the popping could be elicited manually with her palm supinated, forearm slightly abducted, and shoulder elevated forward. It only occurred when her forearm was pronated and not supinated. Manual stabilization of the distal clavicle seemed to eliminate the popping. A tight posterior capsule and scapular dyskinesis were observed in two of the three available cases, and a scapular assist and scapular retraction test were both positive in one. At the time of presentation, strength was generally normal. Five had no reported limitations in range of motion, whereas one initially demonstrated limitation in active range of motion with abduction, internal rotation, and external rotation. Cross-arm adduction was positive in all available cases. In one, O’Brien’s test caused some discomfort, and on a load-shift examination, he had increased posterior play and clicking. He had no biceps tenderness and negative Mayo shear, lift-off, bear-hug, and belly hug tests. Another patient had scapular winging with forward flexion, subtle paresthesia with abnormal sensation, positive apprehension and Speed’s test, and a negative Yergason’s test.
Imaging
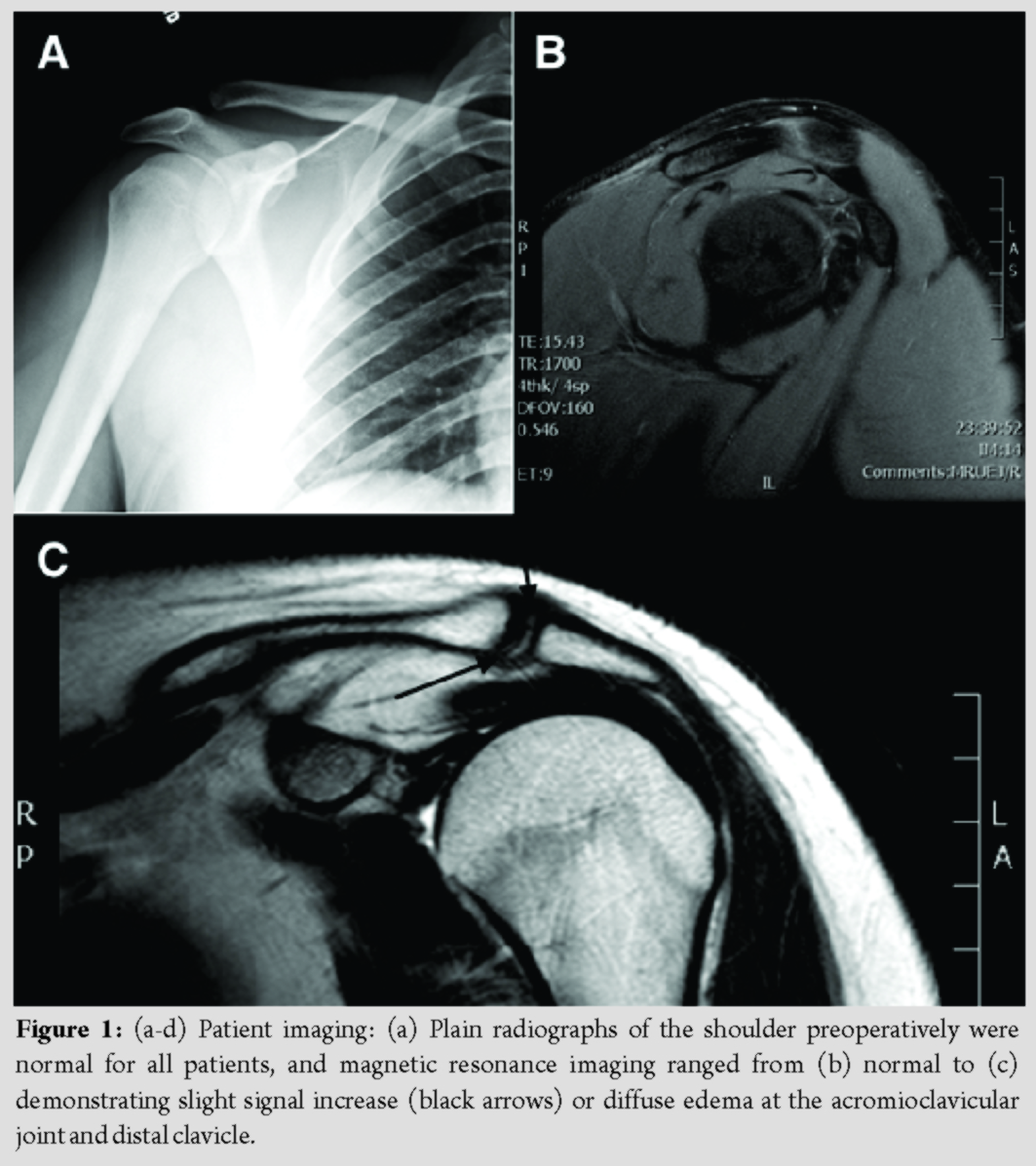
Radiographs were unremarkable and indicated no evidence of arthritis, fracture, or dislocation. The AC joint was normal or at the upper limits of normal (Fig. 1a). Magnetic resonance imaging (MRI) ranged from completely normal (Fig. 1b) to displaying significant changes about the AC joint, including hypertrophied tissue on the undersurface of the AC joint, distal clavicle marrow edema, and increased signal density between the thinned fibrocartilage disk and the chondral surface of the distal acromion (Fig. 1c). Other findings included one patient demonstrating a small amount of signal in the supraspinatus, suggesting a 2–3 mm partial thickness rotator cuff tear. Another showed mild increase in signal in the supraspinatus tendon with no evidence of a tear of the musculotendinous junction. This same patient had some slight signal increase in the anterior aspect of the superior labrum, but it was thought that this was more representative of the sublabral cleft representing a small tear without displacement. One patient with imaging data available had an incidental cyst beneath the posterior superolateral humeral head margin. All other available findings were otherwise normal.
Intraoperative findings and treatment
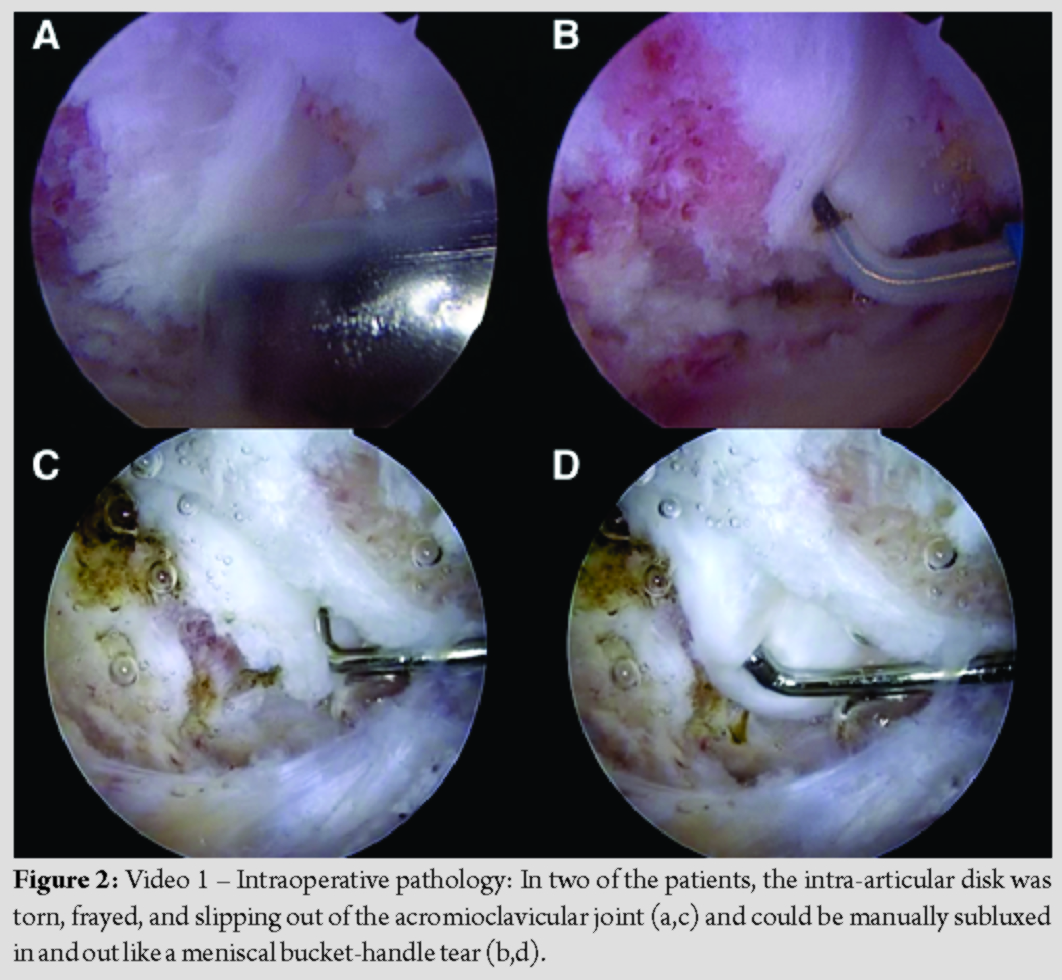
Arthroscopy for all patients was performed in the lateral decubitus position with a general anesthetic and interscalene block. The AC joint was approached through the subacromial space in all cases. When the arthroscope was placed, the bursa was noted to be thickened or inflamed in nearly half (3/7; 42.9%). After removing the inferior surface of the AC joint capsule, attention was paid immediately to the intra-articular disk which was found to have an acute tear (5/7; 71.4%) or degenerative/chronic tear (2/7; 28.6%) in all cases. Acute tears in the disk had clear margins with no fraying, fibrillation, or other signs of chronicity and were localized to the superior quadrant in one and centered in another. In two cases, the intra-articular disk was hypermobile and could be subluxed in and out of the joint (Fig. 2a-d; Video 1). All patients had soft tissue removed and their distal clavicles excised. Aside from AC joint disk pathology, one had a normal appearing biceps tendon, but with a secondary slip that was in continuity with the superior capsule of his shoulder. He also had a Buford complex. Another had some synovitis above the labrum at the superior aspect of his shoulder. One patient was found to have the superior labrum detached at the biceps anchor, but the rest of the labrum looked normal. The SLAP lesion was repaired with one suture anchor into the glenoid and with two sutures attached to it from the posterior and anterior biceps root to secure it down. The patient with minimal supraspinatus signal on imaging had delamination of the supraspinatus and about 15–25% biceps delamination and tearing. The rest of his biceps was intact. He also had some cracking in the posterior labrum. All other structures in these and the other patients were normal.
Outcomes
Maximum follow-up duration ranged from 2 weeks to 1 year. No complications, including weakness, numbness, or paresthesias, were reported. Physical therapy was started on post-operative day 2 for most. At 2-week follow-up, patients generally had decreased pain and were making improvements or even reaching full range of motion and strength. At 6 weeks postoperatively, patients were still making marked progress. Although some were not completely back to all activities, their pain was minimal and they began working back into their normal athletic routines. One patient reported having some additional popping in her shoulder at 6 weeks, but it was minimal and not painful and she reported being very happy with her outcome. Two months from her contralateral shoulder surgery, this same patient felt normal, had full range of motion, excellent strength, and was unable to reproduce popping and ultimately stopped physical therapy. Four months postoperatively, one patient had to return to physical therapy for post-operative general shoulder weakness with reported minimal intermittent pain and popping, and tenderness localized to the AC joint. He was prescribed home exercises for major shoulder muscle groups and range of motion, as well as for cervical spine flexibility. This particular patient had a history of cervical spine issues following a hockey injury, which preceded his traumatic shoulder injury. At 7 months follow-up, one patient reported some pain and slightly limited mobility and strength, specifically with any overhand activities such as overhand tennis serving or throwing. Radiographs taken were consistent with appropriate distal clavicle excision. The patient explained that he had been busy and traveling and although prescribed, he had not completed any real active physical therapy postoperatively. On physical examination, he had no specific point tenderness; negative cross-arm and O’Brien’s tests; and sensation completely intact with 5/5 muscle strength. He had slightly limited internal rotation to about 50°, but otherwise had preserved internal and external rotation and full active and passive range of motion. While he had slow progress, there was no evidence of structural issues accounting for his discomfort at that time. One of the previously mentioned patients with additional popping presented a year later with popping again and pain in her shoulder after heavy renovation work. Pain was described as pressure like, and she felt like it might be subluxing. When she rested, it felt better. She reported difficulty with sleeping and lying on it. On physical examination, her AC joint was non-tender even when the clavicle was moved anteriorly and posteriorly. She did have some mild glenohumeral joint symptoms with translation, particularly posterior translation in both shoulders, suggesting that she might have mild posterior shoulder instability. She had full range of motion and normal strength on strength. As mentioned, she had no real point tenderness, except at the biceps tendon at the coracoid. She had normal sensation, strength, and reflexes. Poor posture and scapular dyskinesis were noted and worse on the right than left. It was determined that she had mild glenohumeral joint instability (multidirectional), with normal MRI findings. All patient data can be found in Table 1 in the additional file. (Table 1 Additional File)
Discussion
The current case series reports on six patients who presented with symptoms of pain, popping, and instability in and around the AC joint after a past traumatic event or shoulder injury with normal radiographs. A torn intra-articular AC joint disk was visualized during surgical treatment. This condition has not been reported commonly in the literature. Atoun et al. [10] reported on nine patients with AC joint pain following road traffic and found that all presented with normal X-rays, but with torn AC joint disks and effusion on MRI. While they could not comment on whether or not the torn disk was an incidental finding or the underlying etiology of symptomatic shoulder pain, arthroscopic AC joint excision provided good outcomes to patients suffering from what they determined was an acceleration-deceleration injury. In 2012, Song et al. [11] reported on 15 patients presenting with residual symptoms following a neglected Grade II AC joint dislocation and found that disk removal instead of ligament reconstruction improved pain scores, Constant scores, and strength in the majority of patients. However, while they make mention of torn articular disks, they also included patients with AC joint osteolysis and osteoarthritis. In our series, one-third of the patients received previous diagnoses of Grade I/II AC joint sprains, lending credence to the hypothesis that a torn AC joint disk may be concomitant, and the result of a post-traumatic injury involving the AC joint (even in low-grade sprains), potentially leading to residual symptoms. Because the AC joint disk degenerates with age and because pain around the AC joint can be non-specific and referred from injury elsewhere in the shoulder or neck, attributing the cause of AC joint pain and popping to a torn intra-articular disk should be a diagnosis of exclusion. Pain from superior labral tears, for instance, can be referred to the AC joint, and so it is suggested that in younger patients with a history of trauma, glenohumeral arthroscopy be considered part of the work-up of AC joint pain to assess a potentially missed SLAP lesion and prevent unnecessary distal clavicle resection [12]. All patients in our series had glenohumeral arthroscopy and many were found to have additional pathology that was treated at the time of removal of the intra-articular disk. One patient had a concomitant SLAP lesion that was repaired. His disk was found to be torn. He reported symptoms of pain but not popping or clicking, indicating that his anterior shoulder pain may be primarily from his SLAP lesion. Regardless, he achieved favorable outcomes postoperatively after both labral repair and distal clavicle resection. Nearly half of the patients had an inflamed subacromial bursa and one demonstrated some minimal delamination and tearing of the biceps tendon and insertion of the supraspinatus. It is unclear whether these changes are separate or related to the pathological changes seen within the AC joint, again highlighting the importance and complexity of diagnosing the pathologic cause of post-traumatic anterior shoulder pain. Furthermore, it is unclear if isolated disk repair or removal would relieve symptoms solely, given that it seems that these injuries are concomitant with previous traumatic shoulder injuries. Disk tissue removal and distal clavicle resection provided good outcomes, though follow-up varied and it is hard to comment on the success of distal clavicle arthroscopic intervention long term. In addition, many of these patients had additional procedures and it is unclear if these were more responsible for clinical improvement than the disk excision and distal clavicle resection itself. In addition to a variable and truncated follow-up, there are many limitations inherent to a level IV evidence treatment case series study. Patients were identified from memory and through a CPT 29824 code query, and there is a chance that patients were not identified if a different billing code or procedure was undertaken. For instance, because a CPT code for distal clavicle excision was used, patients with normal MRIs who were or are currently being treated non-operatively would have been missed. We preemptively excluded all patients with signs of degenerative joint disease, and it is possible that these injuries may be present in patients with osteoarthritis of the AC joint. We cannot comment on the incidence or prevalence of AC joint disk injury, and given the retrospective nature, no formal scoring system was used, and these results are purely correlative, not causative, and should be taken in that light.
Conclusions
In this case series, we report on six young non-arthritic patients who had tearing or degeneration of their AC joint disks, which was thought to be responsible for lingering symptoms of pain, popping, and instability localized to the AC joint. This finding was recognized in patients under the age of 25 with no radiographic evidence of arthritis, who had a prior traumatic event or injury involving their shoulder.
Clinical Message
Further study is needed to determine if AC joint disk tearing is truly symptomatic pathology or merely an incidental finding.
References
1. Buttaci CJ, Stitik TP, Yonclas PP, Foye PM. Osteoarthritis of the acromioclavicular joint: A review of anatomy, biomechanics, diagnosis, and treatment. Am J Phys Med Rehabil 2004;83:791-7.
2. Bontempo NA, Mazzocca AD. Biomechanics and treatment of acromioclavicular and sternoclavicular joint injuries. Br J Sports Med 2010;44:361-9.
3. Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr. Degenerative joint disease of the acromioclavicular joint: A review. Am J Sports Med 2013;41:2684-92.
4. Brys P, Geusens E. Scapular, clavicular, acromioclavicular and sternoclavicular joint injuries. In: Vanhoenacker FN, Maas M, Gielen JL, editors. Imaging of Orthopedic Sports Injuries. Berlin, Germany: Springer-Verlag; 2007. p. 169-82.
5. Saccomanno MF, DE Ieso C, Milano G. Acromioclavicular joint instability: Anatomy, biomechanics and evaluation. Joints 2014;2:87-92.
6. Heers G, Gotz J, Schubert T, Schachner H, Neumaier U, Grifka J, et al. MR imaging of the intraarticular disk of the acromioclavicular joint: A comparison with anatomical, histological and in-vivo findings. Skeletal Radiol 2007;36:23-8.
7. Emura K, Arakawa T, Miki A, Terashima T. Anatomical observations of the human acromioclavicular joint. Clin Anat 2014;27:1046-52.
8. Salter EG Jr., Nasca RJ, Shelley BS. Anatomical observations on the acromioclavicular joint and supporting ligaments. Am J Sports Med 1987;15:199-206.
9. Menge TJ, Boykin RE, Bushnell BD, Byram IR. Acromioclavicular osteoarthritis: A common cause of shoulder pain. South Med J 2014;107:324-9.
10. Atoun E, Bano AA, Tongel AV, Narvani A, Sforza G, Levy O. Acromioclavicular joint acceleration-deceleration injury as a cause of persistent shoulder pain: Outcome after arthroscopic resection. Indian J Orthop 2014;48:193-6.
11. Song HS, Song SY, Yoo YS, Lee YB, Seo YJ. Symptomatic residual instability with grade II acromioclavicular injury. J Orthop Sci 2012;17:437-42.
12. Berg EE, Ciullo JV. The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-9.
 |
 |
 |
 |
| Dr. Andrew W Kuhn | Dr. John E Kuhn | Dr. Scott M LaTulip | Dr. James E Carpenter |
| How to Cite This Article: Kuhn AW, Kuhn JE, LaTulip SM, Carpenter JE. Acromioclavicular joint disk tearing in young non-arthritic individuals: A case series. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 90-94. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


