
[box type=”bio”] Learning Point of the Article: [/box]
Segmental fibulectomy is required to remove the adherent osteochondromas completely and to prevent the recurrence and secondary surgical procedures.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 1-4 | Neetin P Mahajan, Farokh Wadia, Prasanna Kumar. G S, Amit Kumar Yadav, Mrugank Narvekar, Pranay Kondewar. DOI: 10.13107/jocr.2020.v10.i04.1774
Authors: Neetin P Mahajan[1], Farokh Wadia[1], Prasanna Kumar. G S[1], Amit Kumar Yadav[1], Mrugank Narvekar[1], Pranay Kondewar[1]
[1]Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Prasanna Kumar. G S,
Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India.
E-mail: prasannakumargs5@gmail.com
Abstract
Introduction: Hereditary multiple exostosis (HME) is an autosomal dominant disorder affecting the skeletal system, which is characterized by multiple osteochondromas in bones arising from osteochondral ossification and leading to skeletal deformities, short stature, soft tissue, and neurovascular compressive symptoms.
Case Report: A 10-year-old female a case of HME presented with painless multiple swelling around knees, wrist, and painful varus deformity in the lower third of the right leg. The large exostosis of the right distal tibia was symptomatic and indenting the fibula which required excision along with the segment of the fibula of about 2.5 cm above the syndesmosis adjacent to the exostosis as the mass was adherent to the fibula.
Conclusion: Although distal tibia osteochondromas are rare, they can lead to deformity of the ankle and loss of function if not managed early and properly. Hence, early detection, proper planning, and management of periarticular distal tibia osteochondromas are essential to prevent the development or progression of the deformity. Segmental fibulectomy is required to remove the adherent osteochondromas completely and to prevent the recurrence and secondary surgical procedures. It is very essential to follow up the patient till the skeletal maturity to identify the delayed presentation and late progression of the ankle deformities.
Key words: Deformity, Fibulectomy, Hereditary multiple exostosis, Osteochondroma.
Introduction
Osteochondromas also known as exostosis are the benign bony lesions accounting for about 10–15% of all bone tumors and 20–50% of benign bone tumors. Exostosis are developmental malformations rather than true neoplasm, which usually grows during the growth period and the growth usually ceases when skeletal maturity is reached. These exostoses contain cartilage cap and the marrow cavity that is continuous with that of underlying bone. The lesions may be solitary or multiple, the multiple lesions are called hereditary multiple exostosis (HME) which is an autosomal dominant disorder accounts for about 15%. Males are more commonly affected, females are usually carriers, and two-third of the affected patients have a positive family history [1]. These may develop as sessile or pedunculated mass, most commonly in the metaphysis of long bones, such as distal femur, proximal tibia, and proximal humerus and may also arise from flat bones such as scapula and ilium. The pedunculated osteochondromas are directed away from the growth plate and the joint, the broad-based osteochondromas are difficult to differentiate from the normal underlying bone [2]. Most of the patients with osteochondroma are asymptomatic usually, found incidentally as a hard, immobile, non-tender, and protuberant swelling of long duration. Pain in the exostosis may be due to bursitis, fracture, mechanical irritation of surrounding structures, and malignant change which can be suspected by sudden increase in size of the swelling and persistent pain. Most of the asymptomatic masses are observed, surgical intervention is necessary when restriction of joint movements present which hampers the daily routine activity of the patients, deformity, pain, and in suspicion of malignancy. Surgical treatment options include excision and deformity correction using osteotomy.
Case Report
A 10-year-old female patient presented with a complaints of painless swelling around both the knees, right ankle, and left wrist which was first noticed at the age of 6 years and was gradually progressive. The patient started developing pain and deformity at the right ankle for 2 years, which was gradually progressive and had a difficulty in walking since then. There was no history of trauma, fever, weight loss, loss of appetite, and no other constitutional symptoms. Family history of multiple hereditary exostosis was present in father and younger male sibling. On examination, swellings were present over the medial and posterolateral aspect of the distal femur region, in posterolateral aspect of the right proximal tibia and posterolateral aspect of the right distal tibia, which were bony hard in consistency and immobile. The patient had varus deformity in the distal third of the right leg with no distal neurovascular deficit. X-rays of both knees, both ankles, both wrists, and full length both tibia taken in two planes which confirmed the bony exostosis and showed flattening/distortion of the right fibula by large exostosis of the distal tibia and ankle mortise appeared to be preserved (Fig. 1, 2).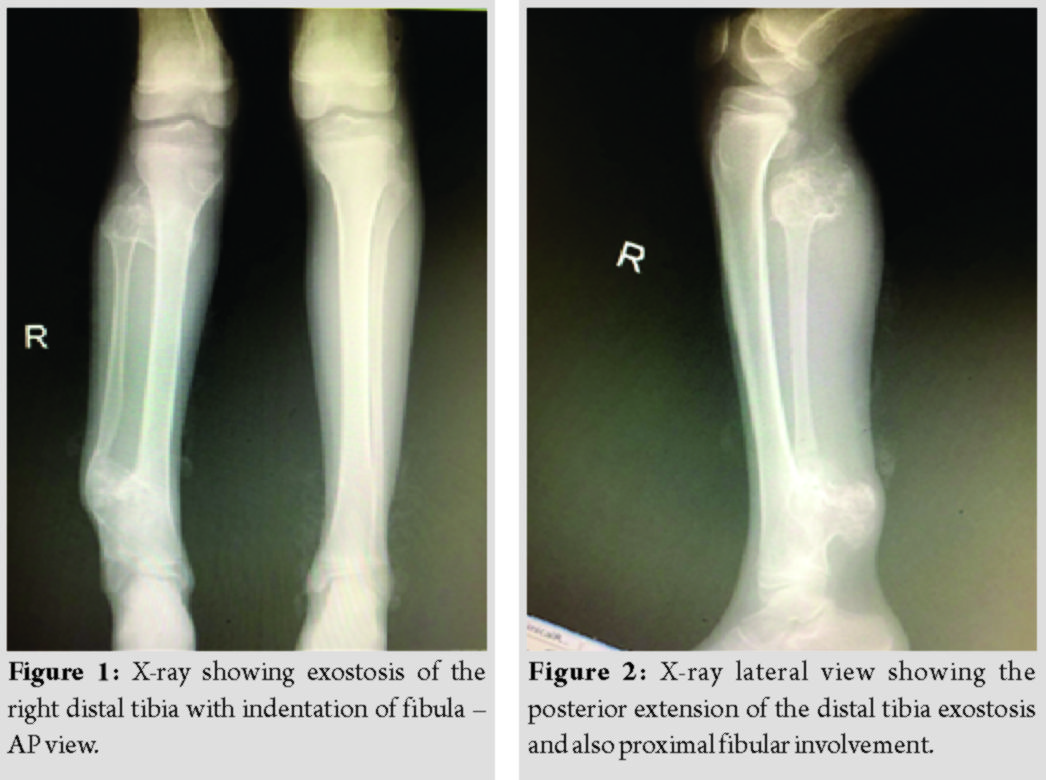
Two-dimensional and three-dimensional computed tomography scan of the right lower limb was taken to know the extent of the exostosis and pre-operative planning, which suggested multiple osseous outgrowths in the lower end of femur, upper tibial metaphysis, distal tibia and proximal fibular metaphysis (Fig. 3, 4). All the swellings showed the continuation with medullary cavity of long bones. The largest lesion was measuring 4.8 × 3.4 × 3.1 cm in size in the posterolateral aspect of the right distal tibial metaphysis, which was indenting the fibula with bowing deformity, the knee and ankle joint movements appeared normal.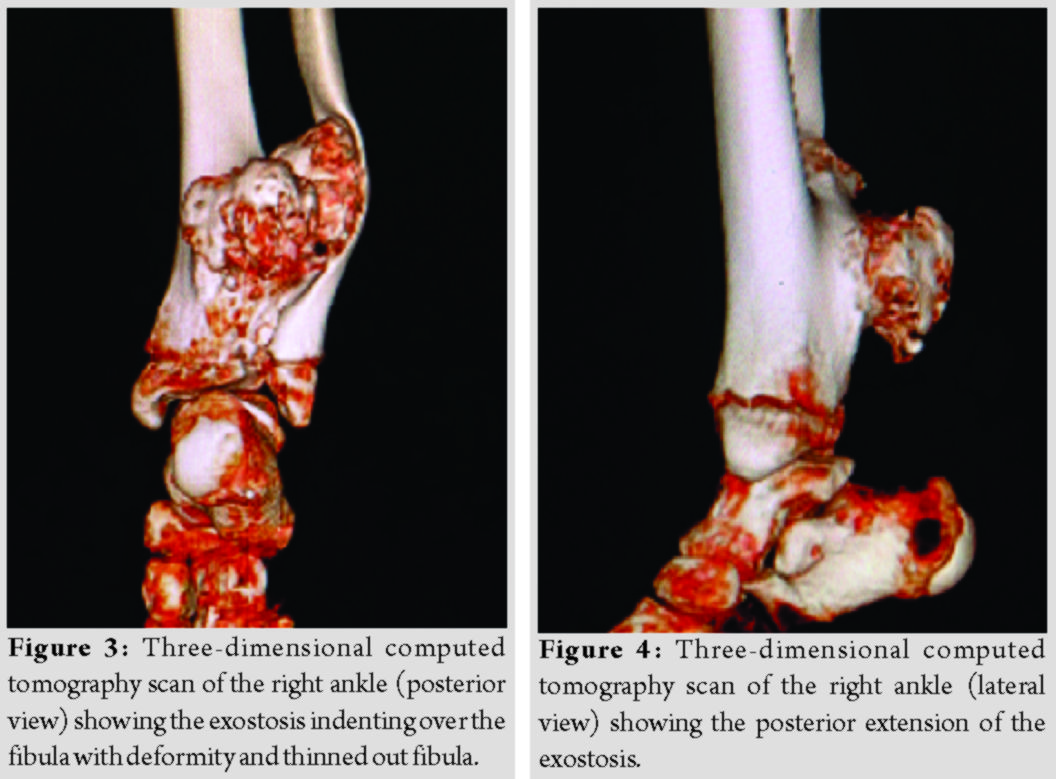
As the patient had symptoms in the right ankle, we planned for excision of the right distal tibia exostosis through posterolateral approach. All routine blood investigations done and were within normal limits and pre-anesthetic checkup was taken for fitness for surgery. The patient was operated in the left lateral position using posterolateral incision, dissection was done between peroneal tendons and flexor hallucis longus, the bony exostosis mass was exposed and excised from the underlying bone using osteotome. Exostosis mass of distal tibia was adherent to the medial aspect of the right distal fibula, a segment of fibula measuring about 2.5 cm was excised above the syndesmosis Level to complete the excision of the bony mass (Fig. 5). Ankle was stable on examination after the segmental fibular excision, so nothing was required to maintain the ankle stability. Excised bony mass was sent for histopathological examination, wound was closed in layers and below knee slab was given for 3 weeks.
Post-operative period was uneventful and post-operative X-ray of the right ankle (Fig. 6, 7) showed complete removal of exostosis mass. The histopathology report was suggestive of osteochondroma (exostosis) with no malignant transformation and the patient was started on full weight-bearing after 3 weeks of surgery. At present (1 year follow-up), the patient has no pain and deformity (Fig. 8, 9) at the ankle and having good ankle range of motion. We are following up the patient regularly (till skeletal maturity) to check for ankle stability and deformity.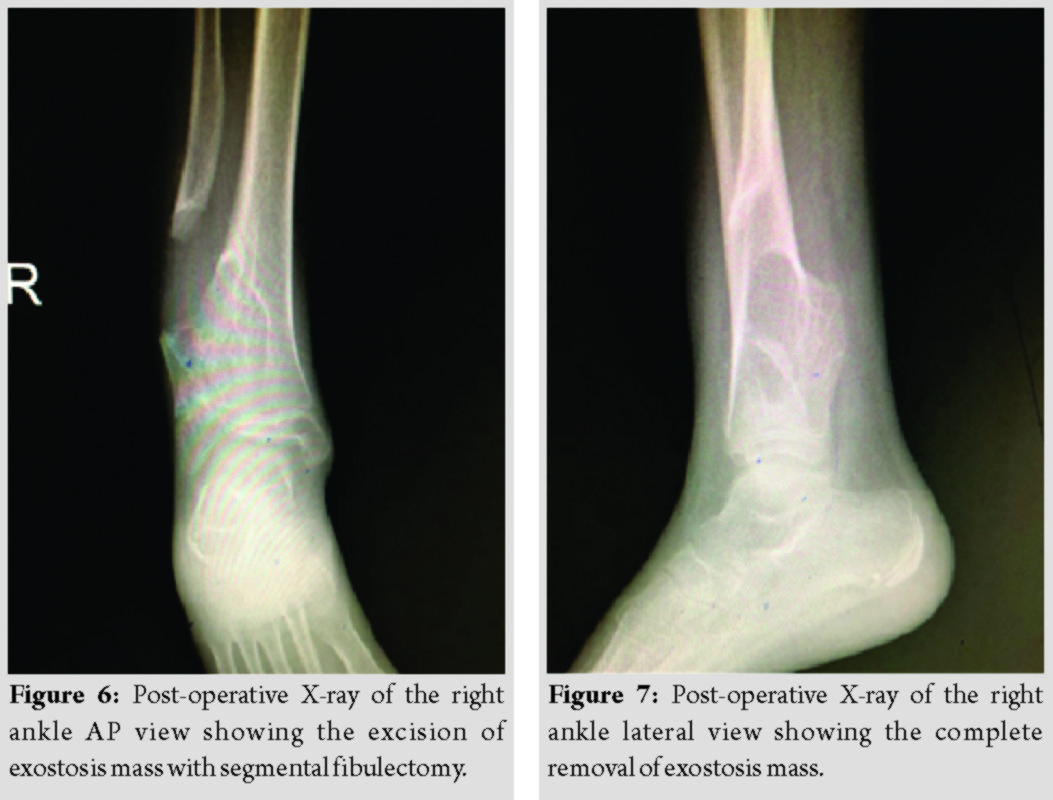
Discussion
HMEs are an autosomal dominant skeletal disorder, which affects 0.9–2 individuals per 100,000 population [3-7]. It is a genetically heterogeneous disorder associated with mutations in tumor suppressor genes called exostosins (EXT). The three EXT loci have been mapped: EXT1 is in chromosomal region 8q23-q24, EXT2 is on 11p11-p12, and EXT3 is on chromosome arm 19p. Mutations of EXT1 and EXT2 are likely to be responsible, respectively, for one-half and one-third of all cases of multiple hereditary exostoses, whereas EXT3 has not been fully isolated and characterized and is probably less frequently involved [3, 4].
Osteochondromas can be associated with a reduction in skeletal growth, bony deformity, restricted joint motion, shortened stature, premature osteoarthrosis, and compression of peripheral nerves. The median age of diagnosis is 3 years, and nearly all the affected individuals are diagnosed by the age of 12 years. The risk for malignant degeneration to osteochondrosarcoma increases with age, although the lifetime risk of malignant degeneration is low (~1%). Family history consistent with autosomal dominant inheritance, which was observed in our case and approximately 10% of affected individuals has no family history of multiple osteochondromas.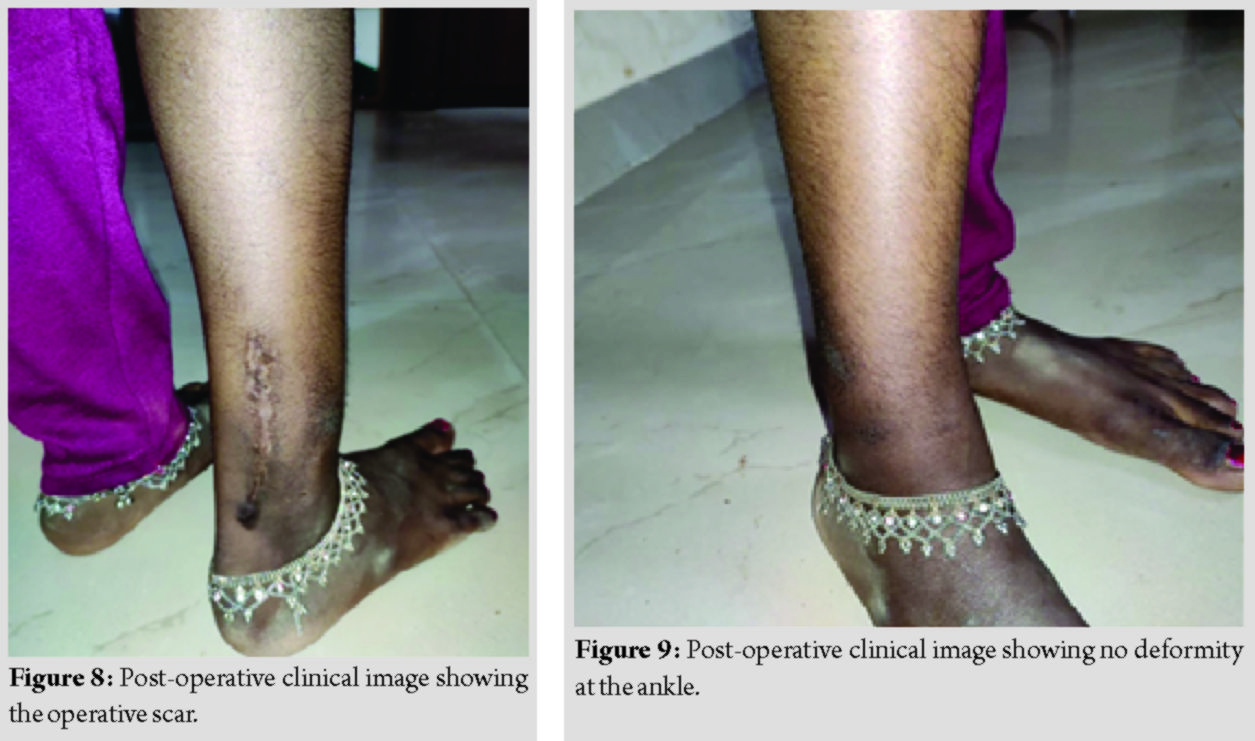
Painful lesions in the absence of bone deformity are treated with surgical excision which includes the cartilage cap and overlying perichondrium to prevent recurrence. Forearm deformity is treated with excision of the exostoses, corrective osteotomies, and ulnar-lengthening procedures. Uncomplicated resection of osteochondromas in growing children is frequently reported, but there is a theoretic risk of growth abnormality resulting from resection of periphyseal osteochondromas. Leg-length inequalities of greater than 2.5 cm are often treated with epiphysiodesis of the longer leg or lengthening of the shorter leg. Angular misalignment of the lower limbs may be treated with hemiepiphysiodeses or osteotomies in the distal femur, proximal tibia, or distal tibia. Early treatment of ankle deformity may prevent or decrease the future deterioration of function, which is observed in our case and the sarcomatous degeneration is treated by surgical resection [8]. In a study of 46 kindred in Washington state, 39% of individuals had a deformity of the forearm, 10% had an inequality in limb length, 8% had an angular deformity of the knee, and 2% had a deformity of the ankle. Angular deformities (bowing) of the forearm and/or ankle are the most clinically significant orthopaedic issues [4]. Ankle joint is also prone for valgus deformity due to relative shortening of distal fibula relative to distal tibia with medial dislocation of talus [9]. Segmental fibulectomy is not required in all the cases of distal tibia osteochondromas, it depends on the adherence of the osteochondromas to the fibula. If the exostosis is very adherent to the fibula along with thinning of the fibula because of the pressure effect by the exostosis and by the deformity, in these situations, segmental fibulectomy is useful. Incomplete excision of the adherent osteochondroma in view of saving the fibula can lead to recurrence and requires secondary procedures. Interosseous osteochondromas can be managed through transfibular excision technique and refixation of the fibula with intramedullary implants [10] or by fibular osteotomy described by Yang et al. [11]. Interosseous osteochondromas of the distal tibia with deformity of the fibula can be managed with transfibular excision of the exostosis and correction of the deformity by Sofield’s method [10, 12]. If the fibula is very thin and not able to pass the intramedullary implants, it is difficult to perform the Sofield’s method. It is essential to keep the ankle joint stable in all the cases to prevent future ankle deformity and chronic ankle pain and the ankle stability can be increased using syndesmotic screws if required.
Conclusion
Although distal tibia osteochondromas are rare, they can lead to deformity of the ankle and loss of function if not managed early and properly. Hence, early detection, proper planning, and management of periarticular distal tibia osteochondromas are essential to prevent the development or progression of the deformity, which hinders the daily routine activities of the patients and to get better functional outcome. Segmental fibulectomy is required to remove the adherent osteochondromas completely and to prevent the recurrence and secondary surgical procedures. It is very essential to follow up the patient till the skeletal maturity to identify the delayed presentation and late progression of the ankle deformities.
Clinical Message
Early detection and management of distal tibia osteochondroma is essential to prevent the development or progression of the deformity. Segmental fibulectomy is essential to remove adherent osteochondromas.
References
1. Pedrini E, Jennes I, Tremosini M, Milanesi A, Mordenti M, Parra A, et al. Genotype-phenotype correlation study in 529 patients with multiple hereditary exostoses: Identification of protective and risk factors. J Bone Joint Surg Am 2011;93:2294-302.
2. Beltrami G, Ristori G, Scoccianti G, Tamburini A, Capanna R. Hereditary multiple exostoses: A review of clinical appearance and metabolic pattern. Clin Cases Miner Bone Metab 2016;13:110.
3. Black B, Dooley J, Pyper A, Reed M. Multiple hereditary exostoses: An epidemiologic study of an isolated community in Manitoba. Clin Orthop 1993;287:212-7.
4. Schmale GA, Conrad EU 3rd, Raskind WH. The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-92.
5. Hennekam RC. Hereditary multiple exostoses. J Med Genet 1991;28:262-6.
6. Nawata K, Teshima R, Minamizaki T, Yamamoto K. Knee deformities in multiple hereditary exostoses: A longitudinal radiographic study. Clin Orthop 1995;313:194-9.
7. Voutsinas S, Wynne-Davies R. The infrequency of malignant disease in diaphyseal aclasis and neurofibromatosis. J Med Genet 1983;2:345-9.
8. Wuyts W, Schmale GA, Chansky HA, Raskind WH. Hereditary Multiple Osteochondromas. Seattle: University of Washington, InGeneReviews®; 2013.
9. D’Arienzo A, Andreani L, Sacchetti F, Colangeli S, Capanna R. Hereditary multiple exostoses: Current insights. Orthop Res Rev 2019;11:199.
10. Thakur GB, Jain M, Bihari AJ, Sriramka B. Transfibular excision of distal tibial interosseous osteochondroma with reconstruction of fibula using sofield’s technique-a case report. J Clin Orthop Trauma 2012;3:115-8.
11. Yang H, Shou K, Wei S, Fang Z, Hu Q, Wan Q, et al. A revised surgical strategy for the distal tibiofibular interosseous osteochondroma. BioMed Res Int 2020;2020:6371456.
12. Sofield HA, Millar EA. Fragmentation, realignment, and intramedullary rod fixation of de-formities of the long bones in children. J Bone Joint Surg Am 1959;41:1371-91.
 |
 |
 |
 |
 |
| Dr. Neetin P Mahajan | Dr. Farokh Wadia | Dr. Prasanna Kumar.G S | Dr. Amit Kumar Yadav | Dr. Mrugank Narvekar |
| How to Cite This Article: Mahajan NP, Wadia F, Kumar P, Yadav AK, Narvekar M, Kondewar P. Segmental Fibulectomy to Excise the Adherent Distal Tibia Osteochondroma in a Case of Hereditary Multiple Exostosis – A Rare Case Report. Journal of Orthopaedic Case Reports 2020 July;10(4): 1-4. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


