
[box type=”bio”] Learning Point of the Article: [/box]
The incidence of tarsal coalition is low, and the occurrence of a triple coalition with a planovalgus deformity is extremely rare. Most cases of symptomatic tarsal coalition are treated conservatively; in this case, despite two years of conservative management, symptoms were not relieved and worsened; hence correction of the deformity at the apex, at talonavicular coalition was performed to achieve a plantigrade foot with the best functional result. Based on the available literature, this approach provides a good functional outcome at a single intervention.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 35-37 | Rajiv Shah, Pascal DeNiese, Shivam Shah. DOI: 10.13107/jocr.2020.v10.i04.1790
Authors: Rajiv Shah[1], Pascal DeNiese[2], Shivam Shah[1]
[1]Department of Foot and Ankle Orthopaedics, Sunshine Global Hospitals, Vadodara, Gujarat, India,
[2]Department of Foot and Ankle Orthopaedics, Foot and Ankle Surgeon, Holy Spirit Hospital, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Rajiv Shah,
Department of Foot and Ankle Orthopaedics, Sunshine Global Hospitals, Vadodara, Gujarat, India.
E-mail: rajivortho@gmail.com
Abstract
Introduction: Tarsal coalitions in the general population are low, possibly due to the asymptomatic nature. In the symptomatic group, however, the presentation is usually during adolescence or early adulthood. The occurrence of a triple tarsal coalition is extremely rare, especially if not associated with a syndrome.
Case Report: We report a case that has the unique configuration of talocalcaneal, talonavicular, and calcaneocuboid coalitions with a planovalgus foot. We review the available literature on this rare occurrence and outline our management in this case to achieve a plantigrade, painless functional foot.
Conclusion: Symptomatic triple coalition planovlagoid cases, require a surgical corrective procedure in order to achieve a plantigrade foot.
Keywords: Tarsal coalitions, rigid flatfoot, planovalgus foot, triplecoalition.
Introduction
Tarsal coalition is the abnormal fusion between adjacent tarsal bones, which may be partial (fibrous or cartilaginous) or complete (bony)[1]. The incidence of tarsal coalition is low, 1–2% of the general population, and the incidence of symptomatic cases even less[2]. Calcaneonavicular and talocalcaneal are the most common coalitions followed by calcaneocuboid and talonavicular, to a lesser extent [3]. The occurrence of these coalitions usually results in rigid deformity. Most cases are managed conservatively with activity modification or orthotics. However, when symptoms are persistent, and the biomechanics of the foot are altered, resulting in damage to adjacent joints due to overload, a more aggressive approach has to be taken [4]. We present a rare case of a triple coalition in a young female, presented with the symptomatic planovalgus foot, and managed with corrective procedures.
Case Report
A 24-year-old female patient presented with complaints of painful deformity of her right foot with marked restriction of activities. Over the past 2years, she received conservative management in the form of medications, physiotherapy, and orthotics without any relief. Clinical examination revealed a planovalgoid foot along with a tight gastrocnemius, with a preserved ankle range of movements (Fig. 1). The subtalar and transverse tarsal joint movements were absent, along with tenderness over the subtalar, talonavicular, and calcaneocuboid joints. The diagnosis was confirmed with standing radiographs. Radiographs demonstrated the congenital fusion of subtalar, calcaneocuboid, and talonavicular joints with heel in valgus (Fig. 2).
Given her disablement and failure of conservative modalities over the past 2years, a decision of surgical management was undertaken. Her pre-surgery American Orthopedic Foot and Ankle Society (AOFAS) score was 35. Correction of heel valgus with a sliding medial calcaneal osteotomy, release of Achilles tightness with gastrocnemius recession, and correction of a collapsed medial longitudinal arch with a corrective fusion of talonavicular joint was planned. In a floppy lateral position, a gastrocnemius recession was performed followed by a medial displacement calcaneal osteotomy. 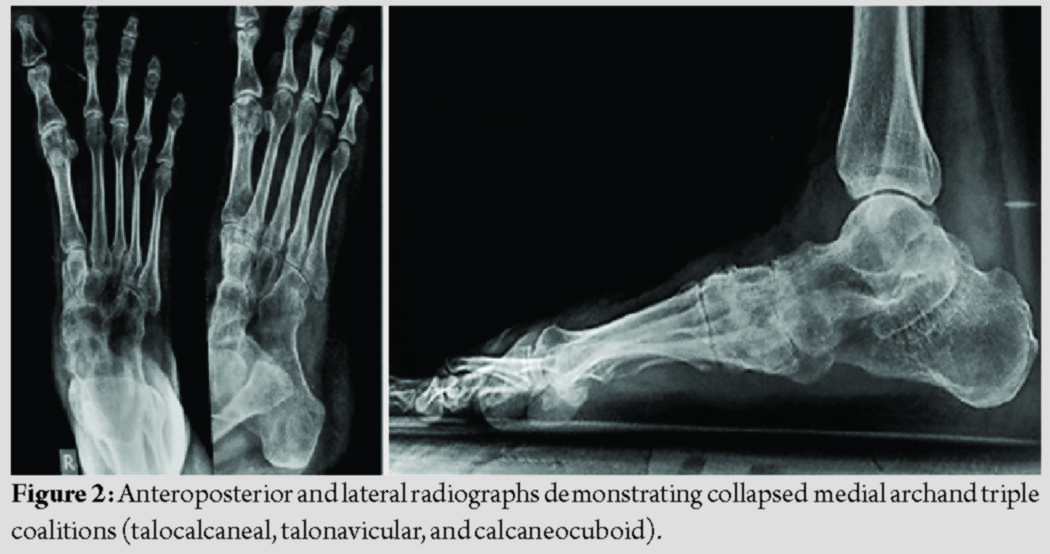 The osteotomy was fixed with two 6.5 mm cannulated cancellous screws, pushed through the subtalar joint up to the neck of the talus. Finally, to correct the sag at the talonavicular joint, a dorsal open wedge osteotomy was carried out at the level of the talonavicular joint, packed with iliac crest bone graft and fixed using a plate, and screws to restore the medial arch (Fig. 3).
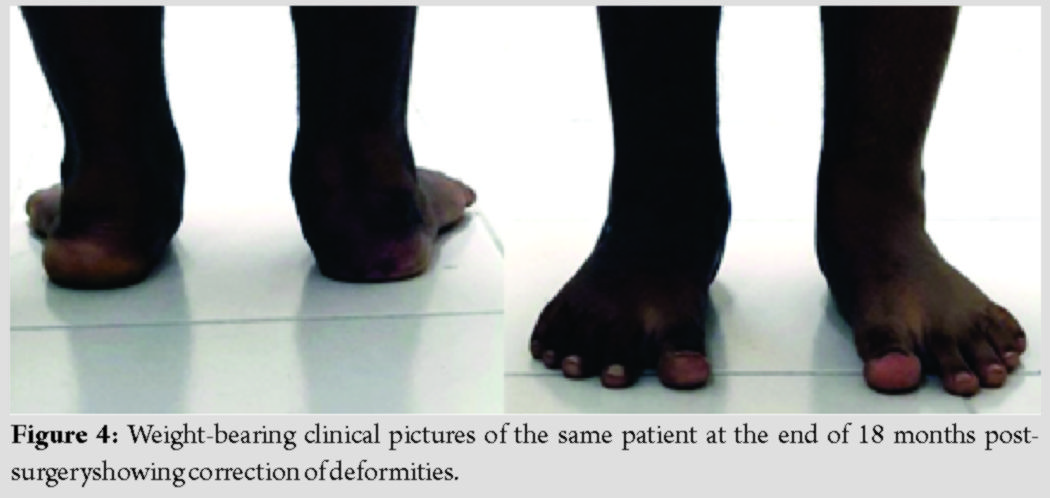
The osteotomy was fixed with two 6.5 mm cannulated cancellous screws, pushed through the subtalar joint up to the neck of the talus. Finally, to correct the sag at the talonavicular joint, a dorsal open wedge osteotomy was carried out at the level of the talonavicular joint, packed with iliac crest bone graft and fixed using a plate, and screws to restore the medial arch (Fig. 3). 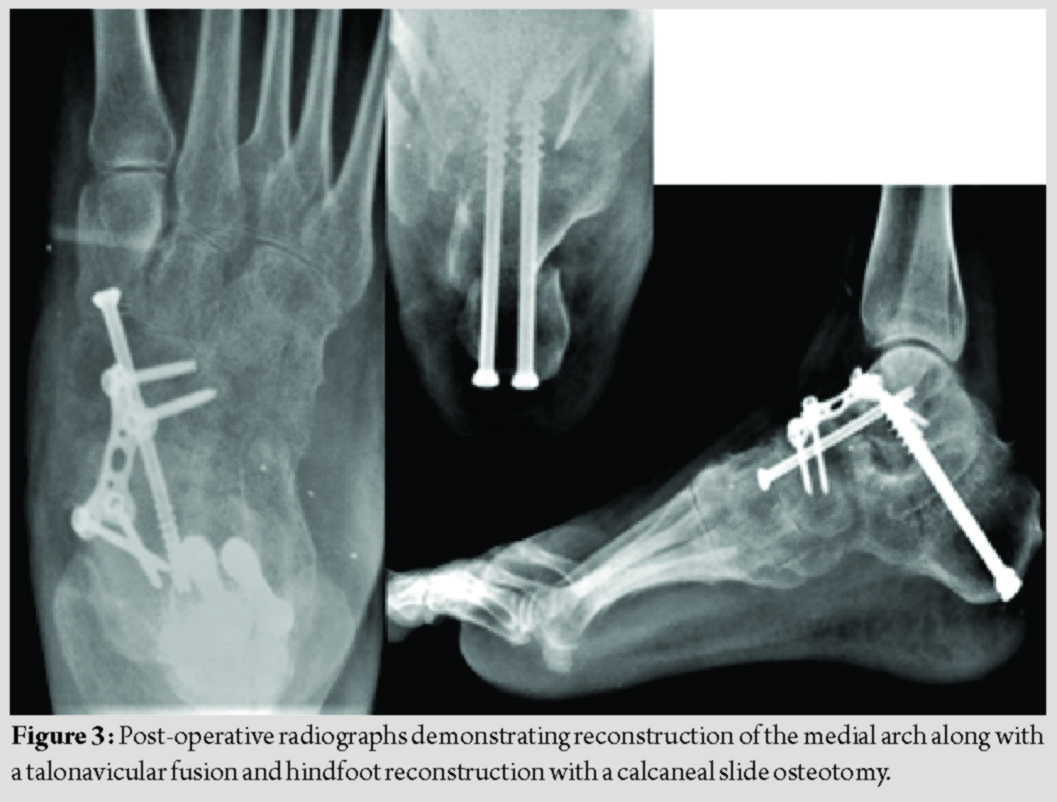 Postoperatively, she was immobilized for 4 weeks. Progressive weight-bearing with ankle range of motion physiotherapy was advised at the end of 6 weeks. The patient went back to all activities of daily living by 4 months.Her post-surgery AOFAS score was calculated as 72. At present, at 18 months post-surgery, she is asymptomatic (Fig. 4 and 5).
Postoperatively, she was immobilized for 4 weeks. Progressive weight-bearing with ankle range of motion physiotherapy was advised at the end of 6 weeks. The patient went back to all activities of daily living by 4 months.Her post-surgery AOFAS score was calculated as 72. At present, at 18 months post-surgery, she is asymptomatic (Fig. 4 and 5).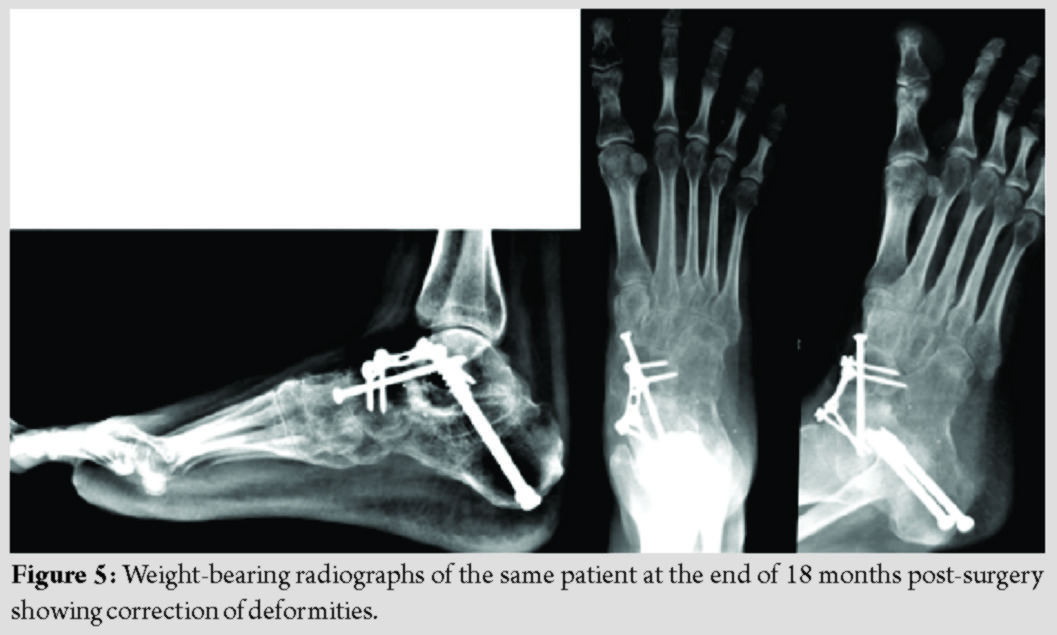
Discussion
The global incidence of tarsal coalition is unknown; this could be primarily due to its asymptomatic nature; however, at present, it is assumed to be <1%[2]. Le Bouq’s theory proposed a failure of differentiation of mesenchymal tissue either due to a first-trimester insult or due to an autosomal dominant defect [5, 6]. Pfitzner proposed the ossification of adjacent accessory bones as another possible reason for the origin of coalitions [7].Common coalitions are talocalcaneal and calcaneonavicular. Most cases can be treated with conservative measures. However, for refractory cases, there is controversy regarding the surgical intervention period and the procedure required to achieve maximum symptomatic relief as well as prevent further complications [8]. Tarsal coalitions with severe planovalgus deformities treated by simple resections tend to have poorer outcomes based on a literature review. Lisella et al. conducted a retrospective case series in which, along with coalition resections, hindfoot reconstructions were performed. The functional outcomes were better than coalition resections alone. All these patients had mild arthritis, and hence, no fusions were done [9]. The presence of triple coalitions, talocalcaneal, calcaneocuboid, and talonavicular is scarce [10]. In patients showing signs of arthritis, a fusion procedure is advised. The literature has suggested corrective triple fusion in such cases [11]. There are sporadic case reports in the literature which mention its conservative management; however, when the coalition results in arthrosis, a double fusion, along with correction of hindfoot deformities, has shown good functional outcomes [12]. In the case reported by us, the patient had no relief following conservative management of 2 years and was disabled with extreme restriction of activities of daily living, affecting her ankle. To reduce, symptoms of foot pain and prevent deterioration of the ankle joint surgical intervention were undertaken. The correction of equinus and valgus of the heel was carried out as a hindfoot deformity corrective procedure. The apex of deformity being at talonavicular joint, corrective fusion at a talonavicular coalition, was carried out to recreate the arch. Failure to correct the biomechanics of the foot would result in complications such as degenerative arthritis of unaffected joints, pathological fractures, and a poor functional outcome[10].
Conclusion
The management tarsal coalition cases associated with symptomatic arthritis may require the fusion of affected joints. When associated with a planovalgus foot, the biomechanics of the foot and ankle have to be taken into consideration to provide a better functional outcome.
Clinical Message
The incidence of a (-) tarsal coalition is low, and the occurrence of a triple coalition with a planovalgus deformity is extremely rare. Most cases of symptomatic tarsal coalition are treated conservatively; in this case,despite2years of conservative management, symptoms were not relieved and worsened; hence, correction of the deformity at the apex, at talonavicular coalition, was performed to achieve a plantigrade foot with the best functional result. Based on the available literature, this approach provides a good functional outcome at a single intervention.
References
1. Lawrence DA, Rolen MF, Haims AH, Zayour Z, Moukaddam HA. Tarsal coalitions: Radiographic, CT, and MR imaging findings. HSS J 2014;10:153‐66.
2. Stormont DM, Peterson HA. The relative incidence of tarsal coalition. Clin Orthop Relat Res 1983;181:28‐36.
3. Bryson D, Uzoigwe CE, Bhagat SB, Menon DK. Complete bony coalition of the talus and navicular: Decades of discomfort. BMJ Case Rep 2011;2011:bcr0320114031.
4. Thorpe SW, Wukich DK. Tarsal coalitions in the adult population: Does treatment differ from the adolescent? Foot Ankle Clin 2012;17:195‐204.
5. Downey MS. Tarsal coalition. In: Banks AS, Downey MS, Martin DE, Miller SJ, editors. McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001. p. 993-1031.
6. Leonard MA. The inheritance of tarsal coalition and its relationship to spastic flat foot. J Bone Joint Surg Br 1974;56B:520-6.
7. Mosier KM, Asher M. Tarsal coalitions and peroneal spastic flat foot. A Review. J Bone Joint Surg Am 1984;66:976-84.
8. Cass AD, Camasta CA. A review of tarsal coalition and pes planovalgus: Clinical examination, diagnostic imaging, and surgical planning. J Foot Ankle Surg 2010;49:274-93.
9. Lisella JM, Bellapianta JM, Manoli A 2nd. Tarsal coalition resection with pes planovalgus hindfoot reconstruction. J Surg Orthop Adv 2011;20:102‐5.
10. Farid A, Faber FW. Bilateral triple talocalcaneal, calcaneonavicular, and talonavicular tarsal coalition: A case report. J Foot Ankle Surg 2019;58:374‐6.
11. Lemley F, Berlet G, Hill K, Philbin T, Isaac B, Lee T. Current concepts review: Tarsal coalition. Foot Ankle Int 2006;27:1163‐9.
12. Ahmad J, Pedowitz D. Management of the rigid arthritic flatfoot in adults: Triple arthrodesis. Foot Ankle Clin 2012;17:309‐22.
 |
 |
 |
| Dr. Rajiv Shah | Dr. Pascal DeNiese | Dr. Shivam Shah |
| How to Cite This Article: Shah R, DeNiese P, Shah S. A Rare Case of Symptomatic Planovalgus Foot with Triple Coalition. Journal of Orthopaedic Case Reports 2020 July;10(4): 35-37. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


