
[box type=”bio”] Learning Point of the Article: [/box]
Open traumatic interphalangeal dislocations of toes can be treated successfully with direct joint`s reduction, soft tissue repair, adequate stabilization and intra/post-operative use of antibiotics.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 78-81 | Michael-Alexander Malahias, Dimitrios Oikonomou, Vikram V. Kadu, Michail Kotsapas, Nikolaos K. Paschos, Dimitrios Giotis. DOI: 10.13107/jocr.2020.v10.i04.1812
Authors: Michael-Alexander Malahias[1], Dimitrios Oikonomou[2], Vikram V. Kadu[3], Michail Kotsapas[2], Nikolaos K. Paschos[4], Dimitrios Giotis[2]
[1]Department of Orthopaedics, HYGEIA Hospital. Erythrou Stavrou 4, Marousi 15123. Athens, Greece,
[2]Department of Orthopaedics, General Hospital of Grevena, Region Military Camp, 51100. Grevena, Greece,
[3]Department of Orthopaedics, M.D. Sancheti Institute of Orthopaedics and Rehabilitation, Pune, Maharashtra, India,
[4]Department of Orthopaedics and Biomedical Engineering, University of California. 1 Shields Ave, Davis, CA 95616, USA.
Address of Correspondence:
Dr. Vikram V. Kadu,
Department of Orthopaedics, Sancheti Institute of Orthopaedics and Rehabilitation, Pune, Maharashtra, India.
E-mail: vikram1065@gmail.com
Abstract
Introduction: Open interphalangeal (IP) dislocations are completely uncommon. Up to now, different patterns of dislocation have been described. The combination of axial loading and hyperdorsiflexion forces, leading to plantar dislocation of the distal phalanx, is a rare type of injury, which has yet not been reported.
Case Report: A rare case of traumatic open dislocation of the left great toe IP joint in a highly active, overweighted, male, amateur football player is presented. The possible underlying mechanism was impact of the left great toe against the ground and subsequent hyperdorsiflexion. The distal phalanx was dislocated plantarly, whereas the proximal phalanx was protruding out the dorsal skin of the toe. Open exploration and reduction led to excellent clinical results 6 months after surgery.
Conclusion: Open traumatic IP dislocation of the great toe due to low force activity is a very rare mode of injury, which requires adequate treatment including immediate purification of the exposed joint, control of the sesamoids’ position, exclusion of intra-articular fractures, joint’s reduction, soft-tissue repair, and proper stabilization.
Keywords: Case report, great toe, interphalangeal dislocation, open dislocation.
Introduction
Toes dislocations are relatively rare injuries. According to a very recent study, 7.6% of all dislocations of the human body refer to toes [1], while other authors claim that the incidence is actually even lower [2]. Great toe dislocation frequently occurs at the metatarsophalangeal joint [3]. In such cases, hallucis longus tendon might be entrapped into the dislocated joint and inhibit closed reduction [4]. Interphalangeal dislocations seem to be more unusual. Paulus mentioned that dislocation of the hallux interphalangeal (IP) joint is a disorder rarely encountered by orthopedic and foot surgeons [5]. He reported a case of a distinct irreducible longitudinal distraction-dislocation that originally presented to the emergency department. A strong dorsiflexion force to the IP joint with the foot and metatarsophalangeal joint fixed in a weight-bearing position is necessary to produce this injury [6]. In another study, Doornberg et al. dealt with a 20-year-old male who required an open reduction of an IP great toe dislocation and subsequent stabilization with a K-wire [7]. Miki et al. identified two different types of IP great toe dislocations [8]. In one type, where the ruptured volar plate is displaced into the joint space between two phalanges, the toe is slightly elongated, but the deformity of the toe is not so marked. In the other type, where the volar plate is completely displaced over the proximal phalangeal neck, the deformity of the toe is extreme as the IP joint is locked in hyperextension. Open IP dislocations are completely uncommon. We present a rare case of traumatic open dislocation of the left great toe’s IP joint in a highly active, overweighted, male, amateur football player.
Case Report
A 31-year-old male police officer (and bodybuilder on his free time) visited our emergency department after an open injury of his left great toe. The patient was overweighted (body mass index: 28.7), but in other respects, he appeared to be healthy. He experienced an acute pain while he was playing football ½ h ago. The possible underlying mechanism was impact of the left great toe against the ground and subsequent hyperdorsiflexion of the distal phalanx. In his clinical examination, he appeared to have an open dislocation of the great toe’s IP joint. The distal phalanx was dislocated plantarly, whereas the proximal phalanx was protruding out the dorsal skin of the toe (Fig. 1a and b).
The patient underwent standard radiographic control (anteroposterior and lateral X-rays), which confirmed our clinical diagnosis (Fig. 2). 
An oral explanation of the proposed surgical intervention and its possible risks was given to the patient and an informed consent was obtained. Within 1 h after his arrival in the emergency room, the patient underwent an open exploration of the injury through his wound. The operation was carried out under local anesthesia on ambulatory basis. We performed a slight expansion (Z shaped) of the incision for better visualization and meticulous purification of the anatomic structures. The dorsal IP joint capsule was ruptured, whereas the hallucis longus tendon was intact and medially dislocated. After careful high-pressure lavage, and use of local antiseptics and antibiotics, an open reduction was performed and the tendon was repositioned properly over the joint axis. Free range of motion (RoM) without any mechanical blocking was obtained. The capsule was closed with absorbable sutures (Vicryl 2-0) and the skin with typical non-absorbable sutures (Prolene 3-0) (Fig. 3a and b).

The IP joint was evaluated after the closure and was found to be stable. Immediate post-operative X-rays confirmed the successful reduction of the joint, but they also revealed a non-displaced, minor linear fracture of the proximal phalanx (Fig. 4). To avoid post-operative infection, antibiotics (ciprofloxacin and clindamycin) were provided intravenously for the first 3 days and then per os for 5 more days.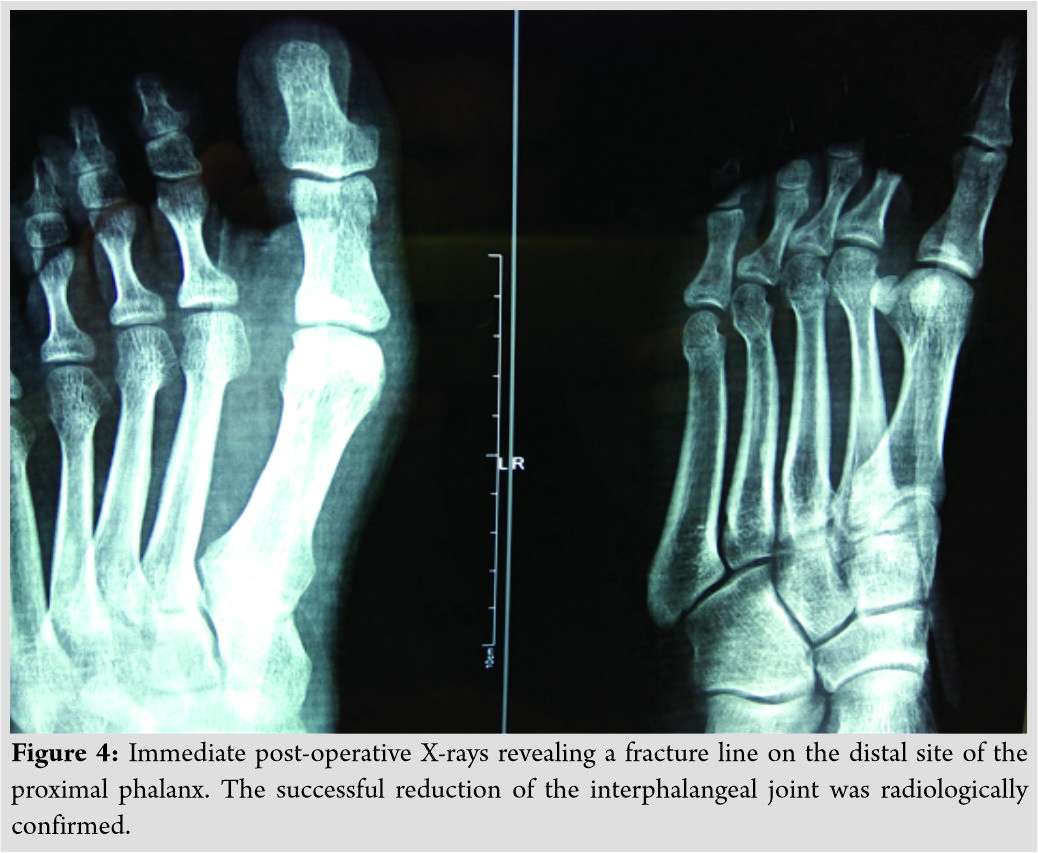
The patient was followed up at the outpatient clinic at 3 weeks, 6 weeks, and 6 months postoperatively with serial radiographs to ensure enlocation of the IP joint and to monitor possible complications. An aluminum zimmer-type splint of the 1st ray was utilized for 3 weeks, while the two first toes were bandaged together during the 4th post-operative week. Gradual mobilization was deployed after the 1st month. As a result, the patient gained full RoM 6 weeks after injury and remained with that RoM and free of pain till his follow-up end point.
Discussion
The first publication of an IP dislocation was made by Eibel at 1954 [9]. More recently, Yang et al. reported a case series of 18 patients suffering from different patterns of IP toe dislocations [10]. These dislocations can be divided into simple or complex, reducible or irreducible, acute or neglected, and closed or open. The vast majority of the published case reports describe a pattern of injury, which involves the interposition of sesamoid bone into the dislocated IP joint [10, 11]. According to Suwannahoy et al., the challenge in reduction is likely to be a result of the interposed plantar capsule with the sesamoid [12]. Invagination of the sesamoid becomes a barrier for manual reduction attempted after the initial injury [13]. Davies et al. focused on interphalangeal sesamoid bones incarcerated in a dislocated joint as a result of an anatomic variant, which demands careful scrutiny of the radiographs [14]. We found no interposed plantar capsule or incarcerated sesamoids intraoperatively. Hallucis longus tendon was not entrapped into the dislocated joint. On the contrary, the patient had an open dislocation of the IP joint after a relatively low-energy injury, whereas it was the dorsal capsule which was ruptured. The stability at the IP joint afforded by collateral ligaments, tendons, and plantar accessory ligament along with the short level arm of the distal phalanx normally resists dislocation [6]. According to Hatori et al., the mechanism for IP dislocations of the great toe is thought to be a combination of axial loading with a hyperextension force when the patient hits his great toe against an unbending surface [13]. In our case, the underlying mechanism was similar. Jones et al. reported a small case series of open IP great toe dislocations [15]. They described two cases of military personnel suffering from an open medial IP dislocation due to a “twisting force.” In contrast to them, our patient experienced a combination of axial loading and hyperdorsiflexion forces which led to plantar dislocation of the distal phalanx. Hence, the pattern of injury is completely different in our case. To the best of our knowledge, this type of great toe IP dislocation has yet not been reported. No post-operative complications were occurred. The patient experienced only mild pain on the 1st day after surgery. He did not receive any painkillers at all. In addition, he was very satisfied at the end of the follow-up and he came back to his physically demanding daily activities. In summary, open exploration and reduction of an open traumatic IP great toe dislocation led to excellent clinical results 6 months after surgery in a highly active, over weighted, young individual.
Conclusion
Open traumatic IP dislocation of the great toe due to low force activity is a very rare mode of injury, which requires adequate treatment including immediate purification of the exposed joint, control of the sesamoids’ position, exclusion of intra-articular fractures, joint’s reduction, soft-tissue repair, and proper stabilization.
Clinical Message
Clinicians must be aware of rare cases where open traumatic IP dislocations of toes can be treated successfully with direct joint’s reduction, soft-tissue repair, adequate stabilization, and intra-/post-operative use of antibiotics. To avoid additional risks for infection, stabilization can be achieved without using Kirschner wires or other types of fixation.
References
1. Nabian MH, Zadegan SA, Zanjani LO, Mehrpour SR. Epidemiology of joint dislocations and ligamentous/tendinous injuries among 2,700 patients: Five-year trend of a tertiary center in Iran. Arch Bone Jt Surg 2017;5:426-34.
2. Yang NP, Chen HC, Phan DV, Yu IL, Lee YH, Chan CL, et al. Epidemiological survey of orthopedic joint dislocations based on nationwide insurance data in Taiwan, 2000-2005. BMC Musculoskelet Disord 2011;12:253.
3. Lievers WB, Adamic PF. Incidence and severity of foot and ankle injuries in men’s collegiate American football. Orthop J Sports Med 2015;3:2325967115581593.
4. Tosun B, Akansel G, Sarlak AY. Traumatic dislocation of the first metatarsophalangeal joint with entrapment of the flexor hallucis longus tendon. J Foot Ankle Surg 2008;47:357-61.
5. Paulus MC, Neufeld SK. Irreducible longitudinal distraction-dislocation of the hallux interphalangeal joint. Am J Orthop (Belle Mead NJ) 2013;42:329-30.
6. Nelson TL, Uggen W. Irreducible dorsal dislocation of the interphalangeal joint of the great toe. Clin Orthop Relat Res 1981;157:110-2.
7. Doornberg JN, Postma IL, Struijs PA. A 20-year-old man with a dislocation of the great toe. Ned Tijdschr Geneeskd 2014;158:A7339.
8. Miki T, Yamamuro T, Kitai T. An irreducible dislocation of the great toe. Report of two cases and review of the literature. Clin Orthop Relat Res 1988;230:200-6.
9. Eibel P. Dislocation of the interphalangeal joint of the big toe with interposition of a sesamoid bone. J Bone Joint Surg Am 1954;36-A:880-2.
10. Yang IB, Sun KK, Sha WL, Yu KS, Chow YY. Interphalangeal dislocation of toes: A retrospective case series and review of the literature. J Foot Ankle Surg 2011;50:580-4.
11. Arvinius C, Valle J, Urda A, León C, Marco RF. Dislocation of the proximal hallux interphalangeal joint with interposition of a sesamoid bone: A blibliographic review. Acta Ortop Mex 2017;31:35-9.
12. Suwannahoy P, Srisuwan T, Pattamapaspong N, Mahakkanukrauh P. Intra-articular ossicle in interphalangeal joint of the great toe and clinical implication. Surg Radiol Anat 2012;34:39-42.
13. Hatori M, Goto M, Tanaka K, Smith RA, Kokubun S. Neglected irreducible dislocation of the interphalangeal joint of the great toe: A case report. J Foot Ankle Surg 2006;45:271-4.
14. Davies MB, Abdlslam K, Gibson RJ. Interphalangeal sesamoid bones of the great toe: An anatomic variant demanding careful scrutiny of radiographs. Clin Anat 2003;16:520-1.
15. Jones MD, May IC, Sweet KJ. Rare open hallux interphalangeal joint dislocations sustained in combatives training: A case series. Mil Med 2014;179:e253-8.
 |
 |
 |
 |
 |
| Dr. Michael-Alexander Malahias | Dr. Vikram V. Kadu | Dr. Michail Kotsapas | Dr. Nikolaos K. Paschos | Dr. Dimitrios Giotis |
| How to Cite This Article: Malahias MA, Oikonomou D , Kadu VV, Kotsapas M, Paschos NK, Giotis D. Open Interphalangeal Dislocation of the Great Toe in an Amateur Football Player: A Rare Case Report. Journal of Orthopaedic Case Reports 2020 July;10(4): 78-81. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


