
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Traumatic glenosphere dissociation is a rare complication that may be associated with reverse total shoulder endoprostheses with longer humeral stems that generate a greater levering effect.
Case Report | Volume 10 | Issue 8 | JOCR November 2020 | Page 63-67 | Michael M Chau, Erick M Marigi, Zac B Novaczyk, Allan F Hunt, Jeffrey T Luna. DOI: 10.13107/jocr.2020.v10.i08.1862
Authors: Michael M Chau[1], Erick M Marigi[2], Zac B Novaczyk[1], Allan F Hunt[1],[3],[4], Jeffrey T Luna[1],[4]
[1]Department of Orthopaedic Surgery, University of Minnesota, Minneapolis, Minnesota, USA.
[2]Department of Orthopaedic Surgery and Sports Medicine, Mayo Clinic, Rochester, Minnesota, USA.
[3]Department of Orthopaedic, Twin Cities Orthopedics, Edina, Minnesota, USA.
[4]Department of Orthopaedic Surgery, Minneapolis Veterans Affairs Health Care System, Minneapolis, Minnesota, USA.
Address of Correspondence:
Dr. Michael M Chau,
2450 Riverside Avenue South, Suite R200, Minneapolis, Minnesota 55454 USA.
E-mail: mchau@umn.edu
Abstract
Introduction: Reverse total shoulder endoprosthetic reconstruction after margin-negative tumor resection of the proximal humerus is becoming more conventional in orthopeadic oncology practices. Mid-term survival and functional outcomes have been satisfactory. This case report corroborates with current literature and further describes a rare traumatic complication.
Case Presentation: We report a case of a 70-year-old male with periosteal chondrosarcoma of the proximal humerus who underwent margin-negative resection and reverse total shoulder endoprosthetic reconstruction that was complicated by glenosphere dissociation sustained from falling onto a hyperflexed arm. Successful revision arthroplasty was performed.
Conclusion: Enhancing glenohumeral joint stability after wide resection of the proximal humerus is important to address rotator cuff insufficiency. The greater levering effect of a longer humeral prosthesis used to increase soft tissue tension may also increase the risk of glenosphere dissociation secondary to trauma. Proper soft-tissue tensioning and surgical technique are critical.
Keywords: Glenosphere dissociation, periosteal chondrosarcoma, reverse total shoulder endoprosthetic reconstruction.
Introduction
Chondrosarcoma is a hyaline cartilage-forming tumor and the third most common primary bone malignancy after myeloma and osteosarcoma. Periosteal chondrosarcoma is a rare subtype comprising <2% of all chondrosarcomas [1]. It originates subperiosteally and typically erodes cortical bone but spares the medullary canal. It predominantly occurs in patients older than 50 years and localizes to the humerus and femur with potential to metastasize to the lungs [2]. Symptoms may include pain, swelling, and insidious loss of limb function. The diagnosis is made clinically, radiographically, and with a biopsy. Wide resection is the current standard of care as chondrosarcomas are resistant to chemotherapy and radiation [3]. Wide resection of the proximal humerus can result in significant functional impairment. Various reconstructive strategies to preserve shoulder function have been described [4, 5, 6]. Reverse total shoulder endoprosthetic reconstruction after margin-negative tumor resection to account for rotator cuff insufficiency is becoming more conventional in orthopaedic oncology practices. However, outcomes and complications have not been fully described. We report a case of periosteal chondrosarcoma of the proximal humerus treated with margin-negative resection and reverse total shoulder endoprosthetic reconstruction that was complicated by traumatic glenosphere dissociation requiring revision arthroplasty.
Case Presentation
A 70-year-old male presented with 18 months of indolent right shoulder pain attributed to a slow growing mass. Medical history was notable for prostate cancer treated with prostatectomy and 50-pack-years of smoking. On exam, there was a prominent mass anteriorly over the right shoulder that was immobile, indurated, and nontender. There were no overlying skin changes. Shoulder range of motion was limited to 110o of forward flexion, 90o of abduction, 60o of external rotation, and internal rotation to L5 compared to the contralateral side (180o, 170o, 60o, and T12, respectively). Motor and sensory function was intact. Radiographs demonstrated an ossified mass arising from the surface of the proximal humeral meta-diaphysis with cortical scalloping (Fig. 1a, b). MRI revealed a lobulated soft tissue mass with T1 and T2 heterogeneous signal enhancement around the proximal humerus, cortical scalloping, and areas of linear dense calcification (Fig. 1c-f).
Workup proceeded with a percutaneous core needle biopsy of the right proximal humerus. Fourteen samples were obtained and all exhibited a cartilaginous appearance. Histopathology diagnosed intermediate-grade chondrosarcoma of periosteal origin (Fig. 2). Tumor staging was carried out with a chest CT and whole-body bone scan, which revealed no evidence of metastasis (Fig. 1g, h). The patient consented for wide resection of the right proximal humerus and reverse total shoulder endoprosthetic reconstruction. A standard extended deltopectoral approach was used (Fig. 3a). The previous core needle biopsy site was ellipsed. Vessels feeding the tumor were ligated. The distal musculotendinous junction of the biceps muscle was resected leaving tendon with the tumor. All segments of the deltoid muscle were spared. The rotator cuff muscles were resected leaving a 1 cm margin of healthy tendon on the resected humeral head. Neurolysis of the axillary and musculocutaneous nerves was performed. The pectoralis major, latissimus dorsi, and teres major muscles were resected from the medial aspect of the humerus leaving a 1 cm margin of healthy tendon on the resected bone. Dissection was carried out distally and the humerus was resected 12 cm from the glenohumeral joint line. Neurolysis of the radial nerve was performed. The resected proximal humerus measured 12×2.5×2.5 cm and peri-humeral mass 8×7.5×6.9 cm. (Fig. 3b). Tissues were sent for frozen sectioning and confirmed tumor-free margins.
Reverse total shoulder endoprosthetic reconstruction was performed(Comprehensive Reverse Shoulder System, Zimmer-Biomet). The glenoid was predrilled and the base plate was affixed with 1 center screw and 4 peripheral screws slightly inferior on the glenoid to avoid scapular notching and shoulder impingement. The glenosphere was sized and engaged with the baseplate by Morse taper. The humeral shaft was reamed and press-fit components were secured (Fig. 3c). The rotator cuff tendons were sutured to the prosthetic neck and the deltoid tendon was myodesed. The pectoralis major, latissimus dorsi, and teres major tendons were sutured through the prosthetic portals (Fig. 3d, e). A standard multilayered closure was performed. Radiographs demonstrated satisfactory prosthetic positioning (Fig. 4a-c).
The humeral shaft was reamed and press-fit components were secured (Fig. 3c). The rotator cuff tendons were sutured to the prosthetic neck and the deltoid tendon was myodesed. The pectoralis major, latissimus dorsi, and teres major tendons were sutured through the prosthetic portals (Fig. 3d, e). A standard multilayered closure was performed. Radiographs demonstrated satisfactory prosthetic positioning (Fig. 4a-c).
Postoperatively, the patient remained in a shoulder immobilizer for 6 weeks before starting physical therapy. Tumor surveillance was planned with shoulder and chest X-rays every 3 months until 2 years postoperatively, biannually for the next 3 years until 5 years postoperatively, and annually thereafter. At 1 year postoperatively, the patient was doing well with acceptable shoulder range of motion: 70o of forward flexion, 80o of abduction, 30o of external rotation, and internal rotation to S1. At 2 years postoperatively, he sustained a fall with the arm hyperflexed resulting in glenosphere dissociation requiring revision arthroplasty (Fig. 5a, c).  Intraoperatively, the glenosphere was completely disengaged (Fig. 6a), there was minimal fretting wear and no corrosion of the Morse taper (Fig. 6b), the polyethylene was inferiorly worn (Fig. 6b), there was no scapular notching, and the humeral component and baseplate were intact (Fig. 6c). Decision was made to increase the prosthetic constraint to account for soft-tissue attenuation by upsizing both the glenosphere and humeral tray (Fig. 6d, 7a-7c).
Intraoperatively, the glenosphere was completely disengaged (Fig. 6a), there was minimal fretting wear and no corrosion of the Morse taper (Fig. 6b), the polyethylene was inferiorly worn (Fig. 6b), there was no scapular notching, and the humeral component and baseplate were intact (Fig. 6c). Decision was made to increase the prosthetic constraint to account for soft-tissue attenuation by upsizing both the glenosphere and humeral tray (Fig. 6d, 7a-7c).
The patient is currently 3 years postoperatively from the index surgery and 1 year postoperatively from revision arthroplasty. There has been no clinical or radiographic evidence of tumor burden or hardware complication. Shoulder range of motion is limited to 70o of forward flexion, 60o of abduction, 30o of external rotation, and internal rotation to S1.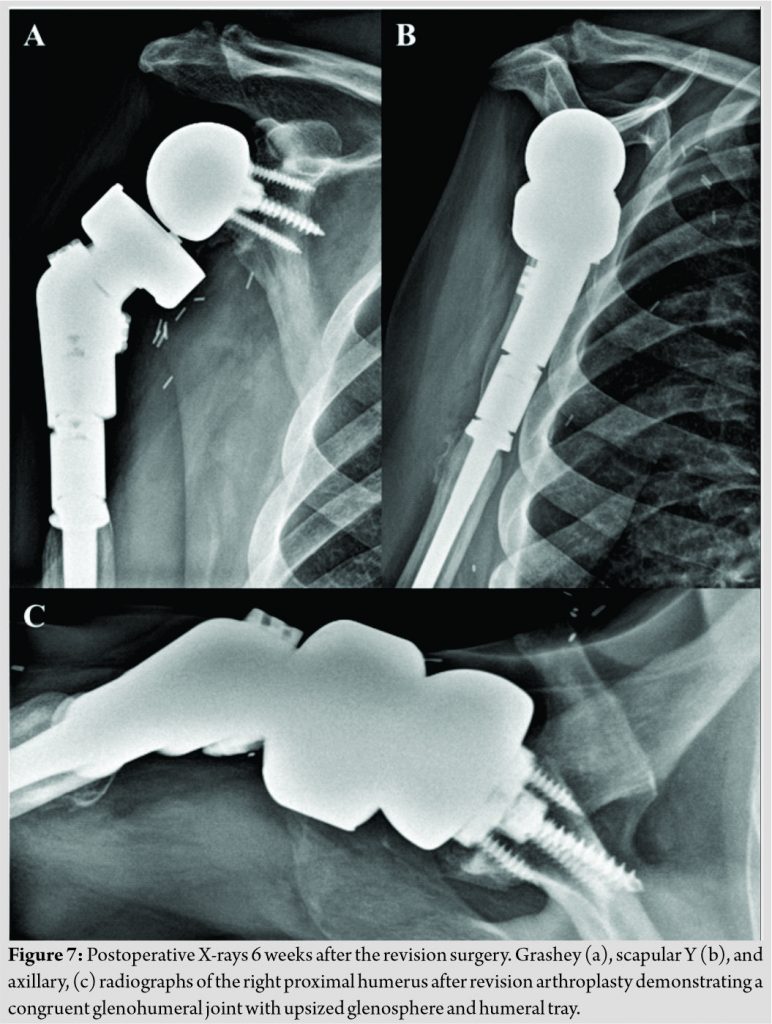
Discussion
Complete resection of periosteal chondrosarcoma is essential to decrease the risk of local recurrence and pulmonary metastasis. Simultaneously preserving shoulder function after margin-negative resection is important for quality of life. Strategies for shoulder reconstruction after proximal humerus wide resection include arthrodesis, resection arthroplasty, osteoarticular allografts, allograft-prosthesis composites, and reverse total shoulder endoprostheses [4, 5, 6]. Mid-term outcomes of reverse total shoulder endoprosthetic reconstruction have been satisfactory in terms of shoulder function, but complications such as instability, glenoid component loosening, and dislocation are possible [7, 8, 9, 10, 11, 12]. To the best of our knowledge, this is the first report to describe glenosphere dissociation following reverse total shoulder endoprosthetic reconstruction. De Wilde et al. retrospectively reported nine patients who underwent reverse total shoulder endoprosthetic reconstruction for proximal humeral tumors, including four chondrosarcomas, that resulted in a mean abduction of 157o and satisfactory functional outcome scores. However, there were two dislocations thought to be due to loss of anterior shoulder stability and the authors recommended using a glenosphere with high contact area combined with optimal prosthetic tensioning [11]. Kaa et al. similarly performed a retrospective review of ten patients with proximal humeral tumors, including four chondrosarcomas, who underwent reverse total shoulder endoprosthetic reconstruction resulting in a mean abduction of 78o but also several complications, including one deep infection, two component loosening, and one dislocation. The dislocation occurred on two separate occasions and was thought to be secondary to deltoid pseudo-paralysis, which was treated with a stem extension to increase soft-tissue tension [10]. Furthermore, Bonnevialle et al. retrospectively reviewed eight patients with proximal humeral tumors, including one chondrosarcoma, who underwent reverse total shoulder endoprosthetic reconstruction providing a mean forward elevation of 122o with satisfactory functional outcome scores. However, three patients experienced a dislocation of which two were anterior and one was posterior. Of the two patients with anterior dislocations, one was a result of brachial plexus injury and the other was due to significant humeral shortening after tumor resection [7]. For our 70-year-old male patient, emphasis was placed on obtaining tumor-free margins while preserving as much muscle and tendon as possible to optimize functional outcomes. Glenoid baseplate and screws were carefully placed to decrease the risk of scapular notching and shoulder impingement. The glenosphere was assembled to maximize durability by fully seating the baseplate screws and engaging the Morse taper with cleaned and dried surfaces. The patient did well up to 2 years postoperatively until he sustained a fall onto a hyperflexed arm resulting in complete glenosphere dissociation. In standard reverse total shoulder arthroplasty, factors contributing to glenosphere dissociation are thought to be improper taper engagement and incomplete glenosphere seating on the baseplate due to soft-tissue interposition or impingement of an osseous rim remaining on the glenoid [13, 14, 15]. Reverse total shoulder endoprosthetic reconstruction may also have an increased susceptibility for glenosphere dissociation due to a longer humeral prosthesis exerting a greater levering force. The optimal amount of soft-tissue tension is unknown and difficult to measure but is often increased to enhance glenohumeral joint stability in the setting of rotator cuff insufficiency.
Conclusion
Treatment of proximal humerus periosteal chondrosarcoma with margin-negative resection and reverse total shoulder endoprosthetic reconstruction can offer cure and satisfactory mid-term outcomes. Traumatic glenosphere dissociation is a potential complication following reverse total shoulder endoprosthetic reconstruction. There may be an important balance between enhancing glenohumeral joint stability and the risk of glenosphere dissociation due to the greater levering effect of a longer humeral prosthesis used to increase soft-tissue tension. Further research can help optimize the amount of soft-tissue tension needed to achieve shoulder stability and desired functional outcomes while decreasing the risk of postoperative complications, including mechanical failure of implanted components.
Clinical Message
Treatment goals for periosteal chondrosarcoma of the proximal humerus are definitive cure followed by preservation of shoulder function. Traumatic glenosphere dissociation is a rare complication that may be associated with reverse total shoulder endoprostheses with longer humeral stems that generate a greater levering effect. Proper soft-tissue tensioning and surgical technique are critical.
References
1. Gelderblom H, Hogendoorn PC, Dijkstra SD, van Rijswijk CS, Krol AD, Taminiau AH, et al. The clinical approach towards chondrosarcoma. Oncologist 2008;13:320-9.
2. Cleven AH, Zwartkruis E, Hogendoorn PC, Kroon HM, Briaire-de Bruijn I, Bovée JV. Periosteal chondrosarcoma: A histopathological and molecular analysis of a rare chondrosarcoma subtype. Histopathology 2015;67:483-90.
3. Goedhart LM, Ploegmakers JJ, Kroon HM, Zwartkruis EC, Jutte PC. The presentation, treatment and outcome of periosteal chondrosarcoma in the Netherlands. Bone Joint J 2014;96:823-8.
4. Nota S, Teunis T, Kortlever J, Ferrone M, Ready J, Gebhardt M, et al. Functional outcomes and complications after oncologic reconstruction of the proximal humerus. J Am Acad Orthop Surg 2018;26:403-9.
5. Teunis T, Nota SP, Hornicek FJ, Schwab JH, Lozano-Calderón SA. Outcome after reconstruction of the proximal humerus for tumor resection: A systematic review. Clin Orthop Relat Res 2014;472:2245-53.
6. Potter BK, Adams SC, Pitcher JD Jr., Malinin TI, Temple HT. Proximal humerus reconstructions for tumors. Clin Orthop Relat Res 2009;467:1035-41.
7. Bonnevialle N, Mansat P, Lebon J, Laffosse JM, Bonnevialle P. Reverse shoulder arthroplasty for malignant tumors of proximal humerus. J Shoulder Elbow Surg 2015;24:36-44.
8. Guven MF, Aslan L, Botanlioglu H, Kaynak G, Kesmezacar H, Babacan M, et al. Functional outcome of reverse shoulder tumor prosthesis in the treatment of proximal humerus tumors. J Shoulder Elbow Surg 2016;25:e1-6.
9. Maclean S, Malik SS, Evans S, Gregory J, Jeys L. Reverse shoulder endoprosthesis for pathologic lesions of the proximal humerus: A minimum 3-year follow-up. J Shoulder Elbow Surg 2017;26:1990-4.
10. Kaa AK, Jørgensen PH, Søjbjerg JO, Johannsen HV. Reverse shoulder replacement after resection of the proximal humerus for bone tumours. Bone Joint J 2013;95B:1551-5.
11. de Wilde L, Boileau P, van der Bracht H. Does reverse shoulder arthroplasty for tumors of the proximal humerus reduce impairment? Clin Orthop Relat Res 2011;469:2489-5.
12. de Wilde LF, Plasschaert FS, Audenaert EA, Verdonk RC\. Functional recovery after a reverse prosthesis for reconstruction of the proximal humerus in tumor surgery. Clin Orthop Relat Res 2005;430:156-62.
13. Cusick MC, Hussey MM, Steen BM, Hartzler RU, Clark RE, Cuff DJ, et al. Glenosphere dissociation after reverse shoulder arthroplasty. J Shoulder Elbow Surg 2015;24:1061-8.
14. Affonso J, Nicholson GP, Frankle MA, Walch G, Gerber C, Garzon-Muvdi J, et al. Complications of the reverse prosthesis: Prevention and treatment. Instr Course Lect 2012;61:157-68.
15. Middernacht B, de Wilde L, Molé D, Favard L, Debeer P. Glenosphere disengagement: A potentially serious default in reverse shoulder surgery. Clin Orthop Relat Res 2008;466:892-8.
 |
 |
 |
|
 |
| Dr. Michael M Chau | Dr. Erick M Marigi | Dr. Zac B Novaczyk | Dr. Allan F Hunt | Dr. Jeffrey T Luna |
| How to Cite This Article: Chau MM, Marigi EM, Novaczyk ZB, Hunt AF, Luna JT. Traumatic Glenosphere Dissociation Following Reverse Total Shoulder Endoprosthetic Reconstruction for Proximal Humerus Periosteal Chondrosarcoma: A Case Report. Journal of Orthopaedic Case Reports 2020 November;10(8): 63-67. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


