
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
The Treatment of pediatric floating elbow often involve open surgery especially when it is associated with flexion type supracondylar fracture and ulnar nerve irritation ; the reduction and fixation of the elbow first is a reasonable technique.
Case Report | Volume 10 | Issue 9 | JOCR December 2020 | Page 71-74 | Mohamad K Moussa, Doumit Semaan. DOI: 10.13107/jocr.2020.v10.i09.1908
Authors: Mohamad K Moussa[1], Doumit Semaan[1]
[1]Department of Orthopaedics, Geitawi Lebanese Hospital, University Medical Center, Beirut – Lebanon.
Address of Correspondence:
Dr. Mohamad K Moussa,
Department of Orthopaedics, Geitawi Lebanese Hospital, University Medical Center. Beirut – Lebanon.
E-mail: mhamadmoussa71976798@gmail.com
Abstract
Introduction: Pediatric floating elbow in the setting of flexion type-supracondylar fracture is exceptional. Most reported cases in the literature include the more common variant of supracondylar fracture which is the extension type. We report a rare case of pediatric floating elbow associating flexion type supracondylar fracture with both bone forearm fracture and ulnar nerve irritation.
Case Report: A 5-year-old boy presenting to the emergency department after sustaining a fall from 3 m height. At presentation, he had an S-shaped deformity of the left upper limb, along with ecchymosis of the medial side of the elbow and the anterior aspect of the forearm. He was also complaining of severe pain with numbness in the territories of the ulnar nerve at the level of the wrist and hand without any signs of the median nerve or radial nerve neuropraxia or injury. The primary assessment demonstrated left flexion type supracondylar fracture, along with ipsilateral radial shaft fracture and ulnar shaft fracture. The patient was treated surgically by open reduction internal fixation of the supracondylar fracture followed by closed reduction and fixation of both bone forearm fracture.
Conclusion: This case is reported for the unique association of flexion type supracondylar fracture – a rare type of supracondylar fracture in children – with ipsilateral both bone forearm fracture in a setting of the floating elbow and a relatively low incident complication which is ulnar nerve neuropraxia.
Keywords: Flexion type supracondylar fracture, floating elbow, pediatric, both bone forearm fracture.
Introduction
Pediatric floating elbow in the setting of flexion type-supracondylar fracture is exceptional. The literature with largest number of clinical cases of supracondylar fracture and even some textbook of pediatric orthopedic does not enumerate such combination of injures [1]. Most reported cases were including the more common variant of supracondylar fracture which is extension type [2, 3]. We present herein a case of pediatric floating elbow associating flexion type supracondylar fracture with both bone forearm fracture with ulnar nerve neuropraxia in a 5-year-old male patient. Our aim is to add further documentation about the flexion type supracondylar fracture and its association because there are not much data about these fracture patterns in the literature. We also propose a modality of treatment of this association with satisfactory final outcome.
Case Report
The patient was a 5-year-old boy presenting to the emergency department after sustaining a fall from 3 m height with a direct blow to the posterior aspect of the left elbow.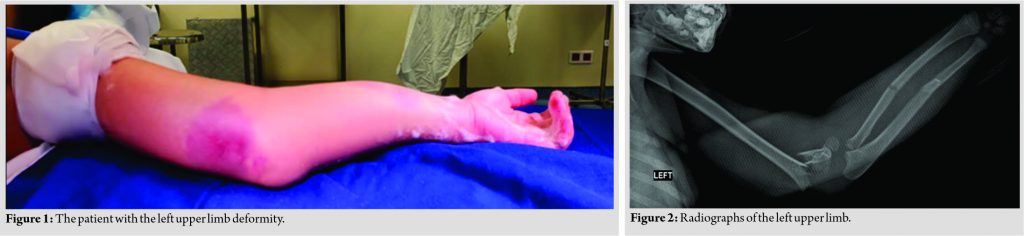
At presentation, he had severe left elbow and forearm pain with an S-shaped deformity of the left upper limb, along with ecchymosis of the medial side of the elbow and the anterior aspect of the forearm (Fig. 1). The patient was complaining of severe pain with numbness in the territories of the ulnar nerve at the level of the wrist and hand without any signs of the median nerve or radial nerve neuropraxia or injury. There was no vascular compromise and the limb was warm well perfused. X-rays were done in the emergency department and showed a left supracondylar fracture, along with ipsilateral radial shaft fracture and ulnar shaft fracture (Fig. 2). The supracondylar fracture was flexion type, displaced with complete loss of anterior and posterior periosteal hinge, type III, according to Gartland classification. Both bone forearm fracture was A3 according to the AO classification, the radial shaft fracture was simple transverse, non-displaced, and located in the diaphyseal mid-third, while the ulnar shaft fracture was simple with slight shortening, and located at the junction of the diaphyseal mid-third and distal third. This fracture could not be classified according to Cuellar-Nieto classification because it does not involve any metaphyseal region of the radius and/or ulna.
The injured limb was immobilized in the emergency room without reduction. The pre-operative plan was to start with reduction and fixation of the supracondylar fracture to limit as possible any additive damage to the ulnar nerve from manipulation of the forearm when addressing the radius and ulna, and then reduce and fix the forearm fracture. Having a warm perfused limb, with ulnar nerve irritation in a setting of floating elbow, the surgical intervention was judged to be urgent but not emergent. That is why the patient was then taken to the operating room during the same day of the injury, where under general anesthesia, supine position, a closed reduction of the supracondylar fracture was tried once under the control of the image intensifier with no success. The reduction technique involved longitudinal traction applied to the forearm to reduce the humeral length while holding the olecranon; the elbow was then extended gradually to correct the angulation. After the failure of the closed maneuver, the decision for the open reduction was taken. After scrubbing and draping, a lateral incision centered over the fracture was made, which allowed direct access to the fracture that was reduced anatomically and fixed by 2 parallel percutaneous Kirschner wires inserted from distal to proximal (lateral to medial) and a 3rd one inserted from proximal to distal (lateral to medical), through the mentioned incision, crossing the other two wires under the control of the image intensifier. Care was taken to not cross the medial cortex distally to avoid any injury to the ulnar nerve. After confirming the stability of the construct, the forearm fractures were reduced closed and fixed by antegrade elastic nailing of the ulna and retrograde elastic nailing of the radius. All wires were embedded under the skin. Finally, a well-padded circumferential long arm cast was applied. Post-operative circumferential cast. Post-operative radiographs of the elbow (Fig. 3) and forearm (Fig. 4) are shown below. Post-operative, the patient was doing well, there were no signs of compartment syndrome, and ulnar nerve symptoms such as numbness and slight weakness of the 5th finger flexion were present. He was discharged after 2 days of monitoring without any signs of compartment syndrome. At 3-week follow-up, the patient was improving in terms of ulnar nerve symptoms; follow-up radiographs showed increasing callus formation (Fig. 5).
At 2 months post-operative, the patient was readmitted for removal of cast and wires. Post-operative testing under general anesthesia showed a good range of motion of the elbow. Post-operative radiographs are shown in (Fig. 6).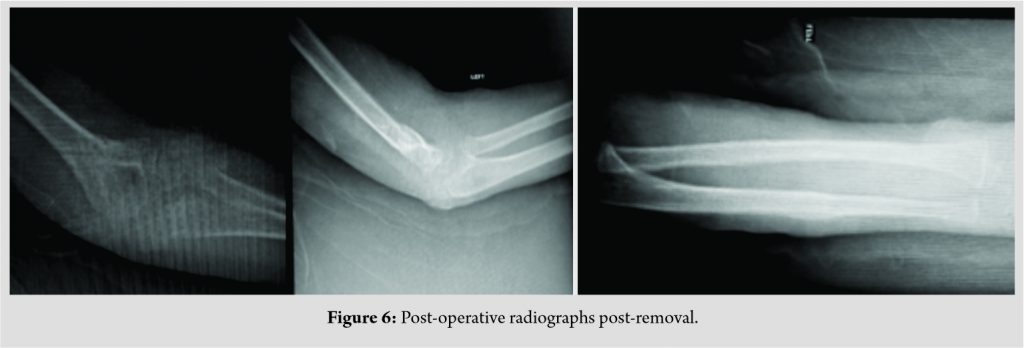
The patient had complete recovery of the ulnar nerve symptoms after 4 months of the initial injury. The patient and family were completely satisfied by the results where there was no complication or residual signs or symptoms.
Discussion
The simultaneous association of supracondylar fractures and both bone forearm fracture is a rare pattern that contributes to a medical condition called “Floating Elbow,” a term that was first introduced by Stanitski and Micheli [4]. It was first restricted to the ipsilateral forearm and humeral shaft fractures but then extended to include intra-articular fractures of distal humerus and elbow dislocation, along with forearm shaft fractures which lead to functional joint dissociation with the rest of the limb [5]. Epidemiologically, elbow fractures represent 12% of all fractures in children [6], of which isolated supracondylar fracture constitutes about 60% of elbow fracture in children [7]. Of these supracondylar fractures, the extension type accounts for 99% of cases [8], and the flexion type fracture, accounts for only 1–3% of them (some authors report 11%) [8, 9, 10, 11]. Its mean annual incidence is 0.8/100,000 [12]. On the other hand, both bone forearm fracture accounts for 13–40% [13]. The simultaneous association of these fractures “Floating Elbow” accounts for 3–13% of all elbow injuries in children [14, 15]. Due to the rarity of flexion type fracture, there was no epidemiological study to tell about its incidence in association with both bone forearm fracture. The very low incidence of flexion type supracondylar fracture and so its association with both bone forearm fracture is confronted by a high rate of complication. In fact, they carry a higher rate of growth disturbances than other fractures in children, higher risk of disrupted carrying angle, reduced range of motion, and a greater risk of ulnar nerve irritation [12]. To add, Muchow et al. studied retrospectively files of 1378 pediatric patients admitted for supracondylar fracture with or without ipsilateral forearm fracture, and the concluded that the presence of a floating elbow can double the risk of acute neurologic injury [16]. On the other hand, being caused by high-velocity injury [14], floating elbow is associated with severe soft-tissue injury which can result in compartment syndrome [17]. Treatment options were variable between authors due to the absence of consensus about it. Primary closed reduction of both fracture followed by long arm cast application is one of the suggested technique; the cast can be applied directly, or after a period of traction till subsidence of the swelling. Others suggested addressing each fracture alone; they recommend pinning of the elbow fracture first, then closely reduce and stabilized the forearm with below elbow cast [18]. And finally, primary surgical stabilization of both the supracondylar fracture and the forearm fractures has been also recommended [8]. The first problem in our case report is that closed reduction of a type III flexion supracondylar fracture is difficult and problematic by itself. It involves elbow extension or using the forearm to apply a posterior directed force to reduce the anteriorly displaced distal humeral fragment through a 90° flexion position [19]. This is not easy to achieve, and if achieved, the elbow is usually in extension, making it technically challenging to stabilize the distal fragment using pins [8]. Moreover, if we add the destabilizing effect of both bone forearm fracture, the reduction by closed maneuver tends to be impossible putting the neurovascular structures at a great risk. For us, this was a clear enough indication for prompt open reduction which has been recommended in the literature if an anatomic closed reduction cannot be obtained [8]. Furthermore, it is believed that the combination of flexion type supracondylar fracture with ulnar nerve palsy can predict the need for open reduction [20, 21]. This belief is valid in our case.
Conclusion
Pediatric floating elbow associating flexion type supracondylar fracture with both bone forearm fracture is a rare entity in pediatric traumatology, for which there are no big data that guide the therapeutic approach. There is a debate in the literature about the sequence of fixation. Reporting this case adopting, a clear strategy increases literature data and helps establishing a clear guideline for the treatment.
Clinical Message
Flexion type supracondylar fracture in a setting of floating elbow requires careful evaluation and pre-operative planning. We believe that this unique entity should be treated with surgical proposing to address the elbow first by open reduction internal fixation and then address the forearm.
References
1. Harrington P, Sharif I, Fogarty EE, Dowling FE, Moore DP. Management of the floating elbow injury in children. Simultaneous ipsilateral fractures of the elbow and forearm. Arch Orthop Trauma Surg 2000;120:205-8.
2. Ring D, Waters PM, Hotchkiss RN, Kasser JR. Pediatric floating elbow. J Pediatr Orthop 2001;21:456-9.
3. Blakemore LC, Cooperman DR, Thompson GH, Wathey C, Ballock RT. Compartment syndrome in ipsilateral humerus and forearm fractures in children. Clin Orthop Relat Res 2000;376:32-8.
4. Stanitski CL, Micheli LJ. Simultaneous ipsilateral fractures of the arm and forearm in children. Clin Orthop Relat Res 1980;153:218-22.
5. De Carli P, Boretto JG, Bourgeois WO, Gallucci GL. Floating dislocated elbow: A variant with articular fracture of the humerus. J Trauma 2006;60:421-2.
6. Illingworth KD, Meisel E, Skaggs DL. The pediatric floating elbow. Oper Tech Orthop 2018;29:43-8.
7. Lins RE, Simovitch RW, Waters PM. Pediatric elbow trauma. Orthop Clin North Am 1999;30:119-32.
8. Skaggs DL, Flynn JM. Supracondylar Fracture of the distal humerus. In: Rockwood and Wilkins’ Fractures in Children. 8th ed., Ch. 16. Philadelphia, PA: Wolters Kluwer Health; 2015.
9. Fowles JV, Kassab MT. Displaced supracondylar fractures of the elbow in children. A report on the fixation of extension and flexion fractures by two lateral percutaneous pins. J Bone Joint Surg Br 1974;56:490-500.
10. Williamson D, Cole W. Flexion supracondylar fractures of the humerus in children: Treatment by manipulation and extension cast. Injury 1991;22:451-5.
11. Farnsworth CL, Silva PD, Mubarak SJ. Etiology of supracondylar humerus fractures. J Pediatr Orthop 1998;18:38-42.
12. Kuoppala E, Parviainen R, Pokka T, Sirviö M, Serlo W, Sinikumpu JJ. Low incidence of flexion-type supracondylar humerus fractures but high rate of complications. Acta Orthop 2016;87:406-11.
13. Jones K, Weiner DS. The management of forearm fractures in children: A plea for conservatism. J Pediatr Orthop 1999;19:811-5.
14. Bhuller GS, Hardy AE. Ipsilateral elbow and forearm injuries in children. Aust N Z J Surg 1981;51:65-8.
15. Papavasiliou V, Nenopoulos S. Ipsilateral injuries of the elbow and forearm in children. J Pediatr Orthop 1986;6:58-60.
16. Muchow RD, Riccio AI, Garg S, Ho CA, Wimberly RL. Neurological and vascular injury associated with supracondylar humerus fractures and ipsilateral forearm fractures in children. J Pediatr Orthop 2015;35:121-5.
17. Suresh SS. Management of “floating elbow” in children. Indian J Orthop 2007;41:386-9.
18. Dhoju D, Shrestha D, Parajuli N, Dhakal G, Shrestha R. Ipsilateral supracondylar fracture and forearm bone injury in children: A retrospective review of thirty one cases. Kathmandu Univ Med J (KUMJ) 2011;9:11-6.
19. Stans AA. Supracondylar fractures of the elbow in children. In: Morrey BF, Sanchez-Sotelo J, Morrey ME, editors. Morrey’s the Elbow and its Disorders. 5th ed., Ch. 27. Philadelphia, PA: Elsevier; 2018. p. 253-68.
20. Delniotis I, Dionellis P, Gekas CC, Arapoglou D, Tsantekidis D, Goulios V, et al. Flexion-type supracondylar humeral fracture with ulnar nerve injury in children: Two case reports and review of the literature. Am J Case Rep 2020;21:e921293.
21. Flynn K, Shah AS, Brusalis CM, Leddy K, Flynn JM. Flexion-type supracondylar humeral fractures: Ulnar nerve injury increases risk of open reduction. J Bone Joint Surg Am 2017;99:1485-7.
 |
 |
| Dr. Mohamad K Moussa | Dr. Doumit Semaan |
| How to Cite This Article: Moussa MK, Semaan D. A pediatric floating elbow associating flexion type supracondylar fracture with both bone forearm fracture and ulnar nerve irritation: A case report. Journal of Orthopaedic Case Reports 2020 December;10(9): 71-74. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


