
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
A lower threshold should be kept for surgical management in displaced bilateral physeal fractures, especially in adolescent age group with borderline remodeling potential.
Case Report | Volume 10 | Issue 9 | JOCR December 2020 | Page 75-79 | Keyur B. Desai1, Gaurav Waghmare1, Ashwin Sathe, R.Chinraj. DOI: 10.13107/jocr.2020.v10.i09.1910
Authors: Keyur B. Desai[1], Gaurav Waghmare[1], Ashwin Sathe[1], R.Chinraj[2]
[1]Department of Orthopaedics, Seth G.S Medical College and King Edward Memorial Hospital, Mumbai, Maharashtra, India,
[2]Department of Orthopaedics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Keyur B. Desai,
Department of Orthopaedics, Seth G.S Medical College and King Edward Memorial hospital, Mumbai, Maharashtra, India.
E-mail: doctorkbd@gmail.com
Abstract
Introduction: Proximal humerus fractures in the pediatric population are relatively uncommon accounting for <3% of all the fractures. Being the growing end of the bone, these fractures have a high threshold for conservative management. Dilemma does exist when such a fracture occurs in a borderline adolescent age group. Occurrence of bilateral physeal fractures in the same anatomical location is exceedingly rare and such a case of bilateral traumatic physeal fracture of proximal humerus has not been reported in the literature.
Case Presentation: A 14-year-old male child presented with post-traumatic pain and swelling of both the shoulders. Radiographs revealed displaced proximal humerus physeal fracture bilaterally. The displaced fracture was treated with closed reduction and percutaneous fixation using smooth Kirschner wires and cannulated screw.
Conclusion: Considering the bilateral nature of the injury and a borderline age with limited remodeling potential, a lower threshold for conservative therapy must be adopted in young active individuals. High-velocity trauma does form a major cause of such bilateral injuries, however, nutritional deficiencies and metabolic causes should be kept in mind while treating such a rare pattern of injury.
Keywords: Proximal humerus, physeal fracture, bilateral shoulder fracture, adolescent shoulder, bilateral physeal injury.
Introduction
Proximal humeral fractures in the pediatric population are relatively uncommon, accounting for less than 3% of all fractures in children and include 4–7% of all epiphyseal fractures [1, 2]. They are the most common injuries of the shoulder and upper arm among children. Regarding the pediatric age groups, these injuries occur most frequently during the first decade and relatively frequently between 11 and 16 years of age due to the greater exposure to high-energy trauma through sports and accidents. Child abuse is another cause of such an injury in children under 18 months of age [3, 4]. There are a wide variety of mechanisms involved in the occurrence of proximal humerus fractures. In the newborn, it may be a result of abnormal arm position during descent along the birth canal in a compromised position [5]. In the pediatric and adolescent groups, it may be a result of direct injury on the affected shoulder or due to fall on outstretched hand with arm in abducted and externally rotated position [6]. The treatment of the fractures also vary from immobilization in sling to closed/open reduction with fixation using Kirschner wires, intramedullary flexible nails and percutaneous screws.
No mechanism and treatment protocol for the management of bilateral fracture have been described in the literature. The purpose of this study is to know the occurrence of such a rare form of bilateral fracture in adolescent age group, the treatment options, and the functional outcome.
Case Presentation
A 14-year-old male child presented to the orthopedic casualty of a tertiary care center with pain in both the shoulders and unable to move both the upper limbs following fall from a moving train. The patient was referred from level one and level two care centers after primary stabilization. He was conscious and oriented with bilateral shoulder swelling and inability to move both the shoulders. There was an associated degloving injury to the face with intact vision. There were no head, chest, or abdominal injuries. Local examination revealed swelling, bruising, and tenderness on both shoulders with arms held by the side of the body. The range of movement was painful and severely restricted. A 4×6 cm degloving injury near the lateral aspect of the face was noted with intact vision. No neurological or vascular deficits noted in both the upper extremities. Anteroposterior and axillary radiographs of both shoulders revealed displaced proximal humeral physeal injury in both the upper extremities with a right-sided clavicle fracture. The left side had a Salter-Harris type 1 (physeal separation) Neer-Horwitz Grade 4 injury with >2/3rd shaft diameter displacement, with 85.6 varus angulation (Fig. 1a). The right side had Salter-Harris type 2 physeal injury of proximal humerus with Neer-Horwitz Grade 2 injury with 16.5° of valgus angulation (Fig. 1b).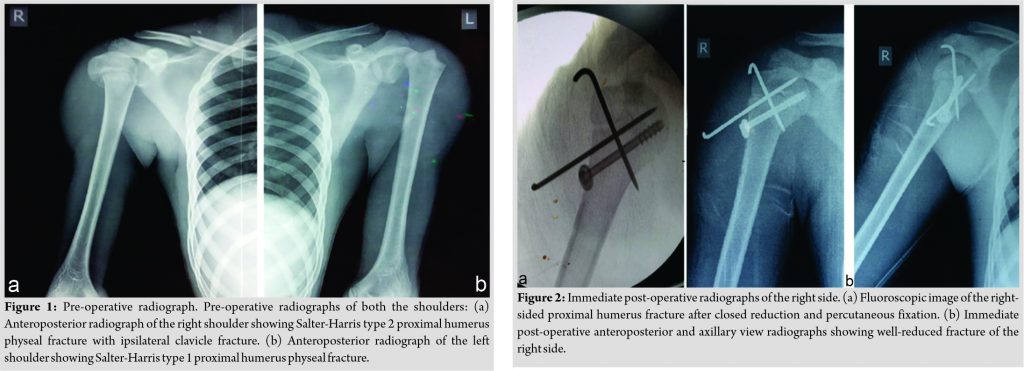
Considering the poor remodeling potential at a borderline adolescent age and the amount of displacement, a decision for closed/open anatomical reduction and fixation was taken. The patient was induced under general anesthesia and a beach chair position was given to ensure adequate fluoroscopic visualization. For the right side, closed reduction by traction, abduction, and rotational maneuver was performed and the fracture reduction was confirmed under orthogonal fluoroscopic imaging. Skin marking was done for the course of the axillary nerve 6 cm distal to the acromion. Two smooth Kirschner wires were inserted percutaneously crossing the physis in a cross pattern. To provide further stability, a 4 mm cannulated cancellous screw was passed with washer across the physis. Stability of the construct was confirmed under fluoroscopy and the pins were bent and placed subcutaneously (Fig. 2a, b).
Similar maneuver was performed on the left side and three smooth Kirschner wires were inserted percutaneously and placed subcutaneously (Fig. 3a, b). Both the arms were placed in a shoulder immobilizer for 3 weeks.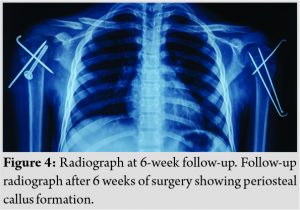
 Gradual passive range of motion exercises were started and the pins were removed at 6 weeks (Fig. 4a, b).Full range of motion was achieved at 3 months postoperatively. The screw removal was scheduled at 6 months, however, the patient was lost to follow-up.
Gradual passive range of motion exercises were started and the pins were removed at 6 weeks (Fig. 4a, b).Full range of motion was achieved at 3 months postoperatively. The screw removal was scheduled at 6 months, however, the patient was lost to follow-up.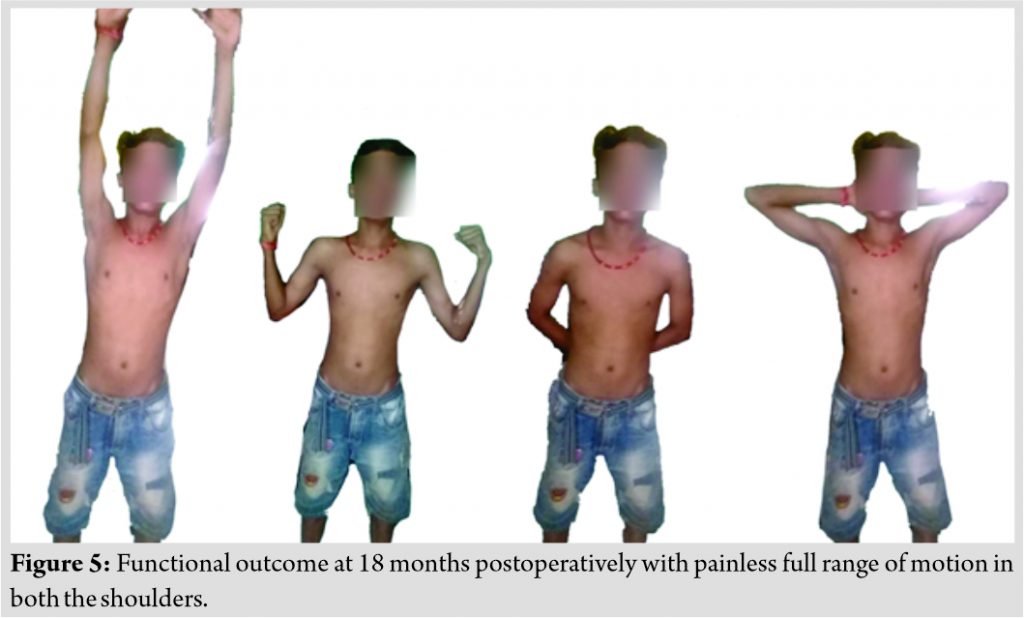
The patient presented at 18 months with full restoration of the function and full range of motion with no pain and the disabilities of the arm, shoulder, and hand (DASH) score of 1.7/100 (Fig. 5).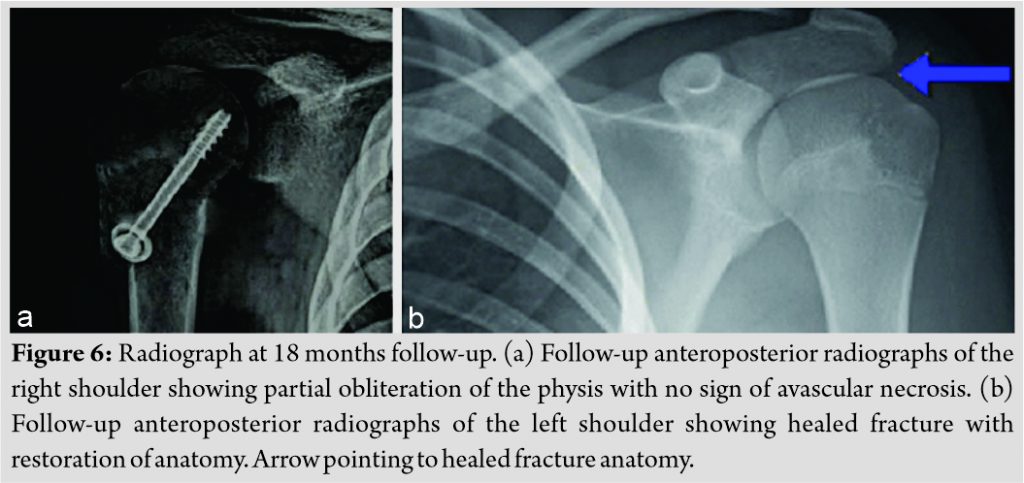
 The right side shows partial obliteration of the physis with no signs of avascular necrosis. The left side healed fracture and restoration of the anatomy (Fig. 6).
The right side shows partial obliteration of the physis with no signs of avascular necrosis. The left side healed fracture and restoration of the anatomy (Fig. 6).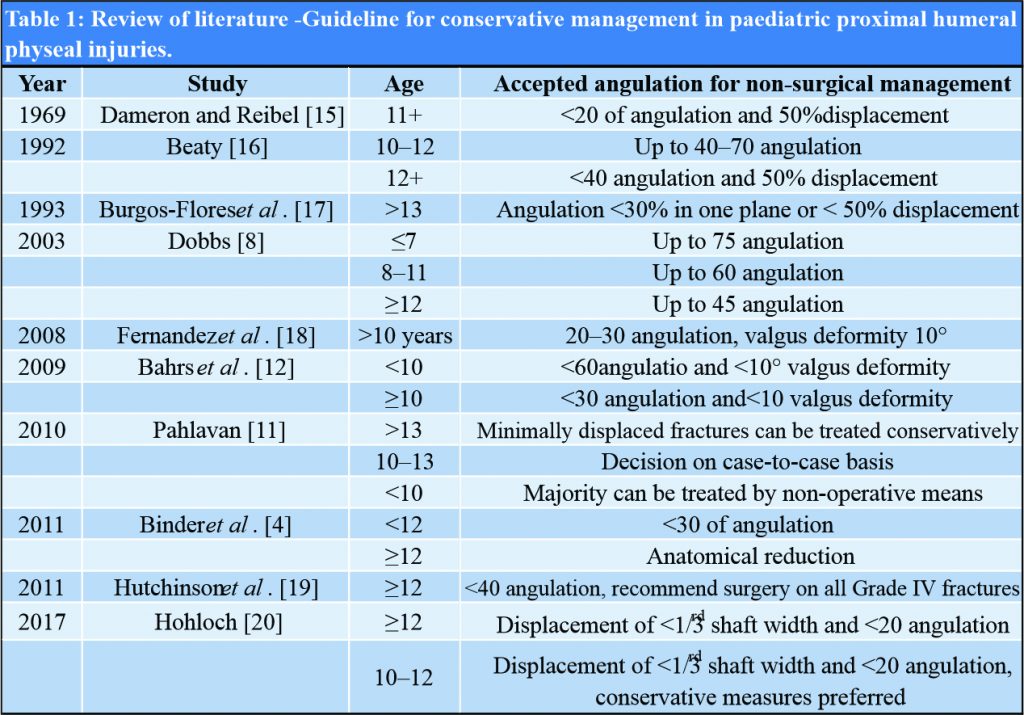

Discussion
Proximal humeral physeal injuries form 0.45% of pediatric fractures. Etiology varies from birth injury, sports injury to high-velocity injuries. Child abuse is a common mode of injury in children presenting before 18 months of age. Proximal humerus is also a common site for unicameral bone cyst, fibrous dysplasia making it more prone to pathological fractures following trivial trauma. Physeal separations in developing countries are common in scurvy [7], but such a bilateral form of injury in the region of proximal humerus has not been previously described. About 80% of the longitudinal growth of the humerus occurs at the proximal humeral physis. This high activity level explains the tremendous remodeling of proximal humerus fractures in the pediatric population. Younger the patient, higher is the remodeling potential.
Most fractures involving the proximal humerus in children aged 5–11 years are metaphyseal, and Salter-Harris type II fractures are predominantly seen in children older than 11 years [8]. Salter-Harris type III and IV injuries are rarely seen and are usually associated with high-energy trauma [9]. Traditional studies showed good to excellent functional results in all age groups of children with pediatric proximal humerus fractures. According to von Laer [10], the patient’s age has a major influence on the treatment of such injuries. Dobbs et al. concluded that Neer-Horwitz Grade I and II proximal humerus fractures in children and older adolescents also should be treated non-surgically. Non-surgical care is not recommended for patients with open Neer-Horwitz Grade I and II fractures, vascular injury, or polytrauma [8]. Controversy exists in the treatment of Neer-Horwitz Grade 3 and Grade 4 injuries, where two factors are considered: (1) Chronological age and (2) amount of displacement and angulation. Table 1 depicts the acceptable alignments for non-surgical management. A systematic review by Pahlavan et al. divided patients based on age groups of <10 years, 10–13 years, and >13 years. Non-surgical management is advocated <10 years because of the good remodeling potential to minimize risk of shortening and malunion. In the age group of >13 years, surgical management is advocated due to the minimal remodeling potential. For children between 10 and 13 years, treatment is to be decided from case to case basis considering remodeling potential [11]. It is in the adolescent age group, that periosteum, long head of biceps tendon, and other structures form a potential impediment to anatomical or near anatomical reduction [12]. Furthermore, as these patients approach skeletal maturity the results of non-operative treatment tend to be potentially worse due to the dismal remodeling potential, especially in non-anatomically reduced fractures. This can lead to long-term restriction in movement and pain [8, 13]. In addition, it remains unclear that even slight malreduction in the proximal humerus may lead to abnormal shoulder biomechanics and bring difficulty to active adolescents involved in high-level sports-related activities [14]. Contemporary literature does not depict clear guidelines for the management of bilateral proximal humeral fracture. A bilateral displaced shoulder fracture, if malunited may add to a significant morbidity in an active adolescent. The treatment was thus undertaken keeping a low threshold for conservative management. Furthermore, the fracture being significantly displaced, surgical management was considered better for an optimal outcome. The patient was advised an implant removal of the cannulated screw at 6 months, however. the relatives did not consent to the same. Considering the age of the child, dismal growing potential, and presence of a multiaxial ball-socket joint proximally, the potential for limb length discrepancy or any future deformity due to partial fusion of the physis was judged to be minimal. At the borderline or late adolescent age, thus the stability of the fracture should be a priority
Conclusion
Open/closed reduction with percutaneous internal fixation can provide excellent outcome in adolescent children with displaced bilateral proximal humerus fractures. The threshold for conservative treatment in severely displaced fractures should be kept low, especially if the injury is bilateral.
Clinical Message
Considering the association of this pattern of injury with a high-velocity trauma, detailed evaluation should be performed to rule out other systemic injuries. Other causes such as child abuse, rickets, and scurvy should be investigated and ruled out. A lower threshold should be kept for surgical management in displaced bilateral physeal fractures, especially in adolescent age group with borderline remodeling potential.
References
1. Neer CS 2nd, Horwitz BS. Fractures of the proximal humeral epiphysial plate. Clin Orthop Relat Res 1965;41:24-31.
2. Rose SH, Melton LJ 3rd, Morrey BF, Ilstrup DM, Riggs BL. Epidemiologic features of humeral fractures. Clin Orthop Relat Res 1982;168:24-30.
3. Ogden JA. Skeletal Injury in the Child. 3rd ed. Philadelphia, PA: Springer Science and Business Media; 2000.
4. Binder H, Schurz M, Aldrian S, Fialka C, Vécsei V. Physeal injuries of the proximal humerus: Long-term results in seventy two patients. Int Orthop 2011;35:1497-502.
5. Ekengren K, Bergdahl S, Ekström G. Birth injuries to the epiphyseal cartilage. Acta Radiol Diagn (Stockh) 1978;19:197-204.
6. Schwendenwein E, Hajdu S, Gaebler C, Stengg K, Vécsel V. Displaced fractures of the proximal humerus in children require open/closed reduction and internal fixation. Eur J Pediatr Surg 2004;14:51-5.
7. Silverman FN. Recovery from epiphyseal invagination: Sequel to an unusual complication of scurvy. J Bone Joint Surg Am 1970;52:384-90.
8. Dobbs M, Luhmann S, Gordon J, Strecker W, Schoenecker P. Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop 2003;23:208-15.
9. Obremskey W, Routt ML Jr. Fracture-dislocation of the shoulder in a child: Case report. J Trauma 1994;36:137-40.
10. Laer L. Verletzungen des Schultergürtels und des Humerusschaftes, Frakturen und Luxationen im Wachstumsalter. Thieme. Germany: Stuttgart; 2007. p. 105-10.
11. Pahlavan S, Baldwin KD, Pandya NK, Namdari S, Hosalkar H. Proximal humerus fractures in the pediatric population: A systematic review. J Child Orthop 2011;5:187-94.
12. Bahrs C, Zipplies S, Ochs BG, Rether J, Oehm J, Eingartner C, et al. Proximal humeral fractures in children and adolescents. J Pediatr Orthop 2009;29:238-42.
13. Larsen CF, Kiaer T, Lindequist S. Fractures of the proximal humerus in children. Nine-year follow-up of 64 unoperated on cases. Acta Orthop Scand 1990;61:255-7.
14. Brenner JS. Overuse injuries, overtraining, and burnout in child and adolescent athletes. Pediatrics 2007;119:1242-5.
15. Dameron TB Jr., Reibel DB. Fractures involving the proximal humeral epiphyseal plate. J Bone Joint Surg Am 1969;51:289-97.
16. Beaty JH. Fractures of the proximal humerus and shaft in children. Instr Course Lect 1992;41:369-72.
17. Burgos-Flores J, Gonzalez-Herranz P, Lopez-Mondejar JA, Ocete-Guzman JG, Amaya-Alarcón S. Fractures of the proximal humeral epiphysis. Int Orthop 1993;17:16-9.
18. Fernandez FF, Eberhardt O, Langendörfer M, Wirth T. Treatment of severely displaced proximal humeral fractures in children with retrograde elastic stable intramedullary nailing. Injury 2008;39:1453-9.
19. Hutchinson PH, Bae DS, Waters PM. Intramedullary nailing versus percutaneous pin fixation of pediatric proximal humerus fractures: A comparison of complications and early radiographic results. J Pediatr Orthop 2011;31:617-22.
20. Hohloch L, Eberbach H, Wagner FC, Strohm PC, Reising K, Südkamp NP, et al. Age- and severity-adjusted treatment of proximal humerus fractures in children and adolescents-a systematical review and meta-analysis. PLoS One 2017;12:e0183157.
 |
 |
 |
 |
| Dr. Keyur B. Desai | Dr. Gaurav Waghmare | Dr. Ashwin Sathe | Dr. R.Chinraj |
| How to Cite This Article: Desai KB, Waghmare G, Sathe A, Chinraj R. Bilateral Traumatic Proximal Humeral Physeal Fracture in an Adolescent Child – A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2020 December;10(9): 75-79. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


